

Abstract
Objective. Few factors have consistently been linked to antibiotic-refractory Lyme arthritis (ARLA). We sought to identify clinical and treatment factors associated with pediatric ARLA.
Methods. We performed a case-control study in 3 pediatric rheumatology clinics in a Lyme-endemic region (2000–2013). Eligible children were aged ≤ 18 years with arthritis and had positive testing for Lyme disease by Western blot. Cases were 49 children with persistently active arthritis despite ≥ 8 weeks of oral antibiotics or ≥ 2 weeks of parenteral antibiotics; controls were 188 children whose arthritis resolved within 3 months of starting antibiotics. We compared preselected demographic, clinical, and treatment factors between groups using logistic regression.
Results. Characteristics positively associated with ARLA were age ≥ 10 years, prolonged arthritis at diagnosis, knee-only arthritis, and worsening after starting antibiotics. In contrast, children with fever, severe pain, or other signs of systemic inflammation were more likely to respond quickly to treatment. Secondarily, low-dose amoxicillin and treatment nonadherence were also linked to higher risk of ARLA. Greater antibiotic use for children with ARLA was accompanied by higher rates of treatment-associated adverse events (37% vs 15%) and resultant hospitalization (6% vs 1%).
Conclusion. Older children and those with prolonged arthritis, arthritis limited to the knees, or poor initial response to antibiotics are more likely to have antibiotic-refractory disease and treatment-associated toxicity. Children with severe symptoms of systemic inflammation have more favorable outcomes. For children with persistently active Lyme arthritis after 2 antibiotic courses, pediatricians should consider starting antiinflammatory treatment and referring to a pediatric rheumatologist.
Lyme disease (LD) is the most common vector-borne disease in the United States and Europe, and its incidence is rising1. After erythema migrans, arthritis is the second most common LD-specific manifestation and the predominant feature of late-disseminated disease1,2. The Infectious Disease Society of America (IDSA) and the American Academy of Pediatrics recommend treatment of Lyme arthritis (LA) with up to 8 weeks of oral antibiotics or 2–4 weeks of intravenous (IV) antibiotics3,4. Most people with LA experience resolution after antibiotics, but about 10% continue to have arthritis despite adequate antibiotic treatment — a condition known as antibiotic-refractory LA (ARLA)5. The underlying pathophysiology of ARLA remains unclear, but this condition likely results from a combination of microbial and host-specific factors5.
Many studies have investigated factors associated with ARLA, yielding few consistent findings. In a predominantly adult cohort with LA, age and other demographics, symptoms, joint counts, and disease duration were not associated with antibiotic response5. Pediatric studies have linked variable findings to ARLA, including female sex6, higher Lyme Western blot band count6, high platelet count7, development of arthritis in additional joints after starting antibiotics8, and the presence of inflammatory back pain or enthesitis8. However, these findings have not been replicated. Several pediatric studies have suggested that older children might be more likely to have ARLA6,7,8; however, this finding did not reach statistical significance in some studies7,8 and was not identified in others9,10. In both children and adults, one feature implicated in ARLA is intraarticular glucocorticoid (IAGC) injection before antibiotic initiation, possibly by impairing early host immune defense5,11.
Refractory post-LD symptoms sometimes lead to prolonged antibiotic treatment, an approach that has not been proven efficacious for cognitive symptoms12,13 or LA14. This lack of efficacy along with the risks of prolonged antibiotics are strong incentives to limit the duration of antibiotic treatment for ARLA. Further, several antiinflammatory and antirheumatic agents prescribed by rheumatologists may be used to treat ARLA5,6,7,10. To better understand the pathophysiology of ARLA, promote judicious antibiotic usage for LA, and ensure timely referral to specialists, we sought to identify characteristics of individuals least and most likely to respond to guideline-compatible treatment. Given the lack of replicability of prior exploratory research and the risks of false-positive findings in such studies, we identified 13 potential explanatory demographic and clinical variables suspected a priori to be related to the development of ARLA in children (Supplementary Table 1, available with the online version of this article).
MATERIALS AND METHODS
Study design and setting
We performed a case-control study of children with LA from 3 pediatric rheumatology referral centers [Children’s Hospital of Philadelphia (CHOP), Nemours/A.I. duPont Hospital for Children, and Penn State Hershey Children’s Hospital] that routinely see children from 4 Lyme-endemic states (Pennsylvania, New Jersey, Delaware, and Maryland).
This study was approved by the institutional review boards of the participating centers (CHOP IRB 14-010818, Nemours #598679, Hershey STUDY00000431) and Rutgers University (PRO Pro20170002088), with a waiver of consent/assent for this minimal-risk retrospective research.
Study population
The study consisted of children aged ≤ 18 years at LA diagnosis who were seen in a participating rheumatology clinic between January 1, 2000, and December 31, 2013. Potential participants were screened through queries of electronic health records (EHR) for children evaluated in a pediatric rheumatology clinic with a diagnosis of LD (International Classification of Diseases-9-Clinical Modification code 088.81). Clinical LA diagnosis was confirmed by record review according to these criteria: (1) documented positive serologic Lyme testing with ≥ 5 IgG bands present on Western blot testing performed using standard methods; and (2) documented arthritis on physical examination or arthrocentesis, with other causes of arthritis excluded. Arthritis on examination was defined by the presence of joint effusion or 2 other signs of inflammation (warmth, tenderness, restricted or painful range of motion) documented by a physician. Although several local clinical laboratories did not routinely perform screening ELISA before Western blot testing as recommended by guidelines3,4, children with arthritis and positive Western blot testing alone were routinely treated for LA at participating centers. Therefore, children lacking Lyme ELISA results were included in the study and excluded from sensitivity analyses (see Statistical Analysis below).
Case definition
Cases had ARLA as defined by IDSA guidelines: persistently active LA documented ≥ 2 months after completion of ≥ 8 weeks of oral antibiotics (amoxicillin, doxycycline, cefuroxime) or ≥ 2 weeks of IV antibiotics (ceftriaxone, cefotaxime), with negative synovial fluid Lyme PCR testing if performed (primary case definition)5. Because some individuals had prolonged arthritis but did not receive sufficient treatment per IDSA guidelines, sensitivity analyses considered a second set of cases with persistently active arthritis for ≥ 6 months after initiating antibiotics, irrespective of treatment.
A comparator group of controls consisted of eligible participants whose LA resolved within 3 months after antibiotic initiation. Clinical resolution of LA was defined as having resolution of all pain and stiffness and no more than a small joint effusion on examination. We considered small, asymptomatic effusions as consistent with clinical resolution because (1) LA can cause prolonged (if mild) joint swelling even after apparent eradication of detectable borrelial infection, and (2) this clinical state was considered a suitable endpoint for both treatment and followup in all 3 centers.
Independent variables
Primary explanatory variables included demographics, clinical features at the time of diagnosis, and clinical features observed within 6 weeks of antibiotic initiation (Supplementary Table 1, available with the online version of this article). These variables were selected a priori based on the literature and investigators’ clinical experiences. A 6-week window for certain variables was selected because (1) early clinical changes after treatment initiation could have important prognostic value, and (2) certain symptoms and signs suggesting chronicity might be recognized or reported only by specialists seeing patients who previously started treatment but did not respond. We also collected information on other demographic, clinical, and treatment characteristics evaluated in exploratory secondary analyses. We collected information about medication-associated toxicities while participants received antibiotics. Missing duration for the 4 main antibiotics (amoxicillin, doxycycline, ceftriaxone, and cefuroxime) was imputed at the median, 28 days (Supplementary Table 2, available with the online version of this article). This imputation was considered reasonable given the small proportion of courses lacking duration data and minimal variability in prescribing across sites, which broadly adhered to guidelines for treatment duration3,4. Variables with missing data (e.g., arthritis duration, antibiotic dose) were considered missing at random, given available data associated with missingness including center, specialty of diagnosing clinician, time to first rheumatology visit, and outcome. Thus, we imputed missing data by multiple imputation of 20 datasets using chained equations15.
Data collection
Study data were abstracted from each center’s EHR using standardized forms by an attending pediatric rheumatologist, pediatric rheumatology fellow with ≥ 1 year of clinical training, or trained research staff. Charts extracted by nonclinical research staff were reviewed by supervising physicians to ensure accuracy. Data inconsistencies prompted repeat EHR review and data abstraction as needed. Clinical data related to care preceding the first visit to pediatric rheumatology clinic were extracted from primary documentation (e.g., primary care notes) where available or otherwise from rheumatologists’ consultation notes. Data were collected and managed using REDCap (Research Electronic Data Capture) tools hosted at Nemours16.
Statistical analysis
Characteristics of cases and controls were compared using standard descriptive statistics. Primary explanatory variables associated with ARLA in univariate analyses (p < 0.2) were included in a multivariable logistic regression model. We retained model variables that were significantly associated with ARLA (p < 0.05) or changed adjusted OR (aOR) between age and ARLA by ≥ 10%. We did not adjust for multiple comparisons because each primary explanatory variable was hypothesis-driven. We tested for statistical interactions between age and other variables, considering p < 0.1 to represent a significant interaction. Exploratory secondary models incorporated additional covariates that were considered clinically relevant posthoc, such as characteristics of initial antibiotic treatment (e.g., dose, frequency).
We performed several sensitivity analyses to assess the influence of our assumptions: additional adjustment for treatment center; alternative outcome definition of persistent LA ≥ 6 months after antibiotic initiation; exclusion of children without documented Lyme ELISA; exclusion of children with antibiotic courses of unknown duration; exclusion of children who did not receive IV antibiotic treatment despite lack of improvement on oral antibiotics, in accordance with treatment recommendations3; and categorization of participants who were lost to followup as (1) having ARLA (worst case imputation) or (2) having ARLA if (a) the imputed date of resolution was ≥ 2 months after completion of sufficient treatment, or (b) there was insufficient treatment to qualify for ARLA before loss to followup.
All analyses were performed using Stata 12.1 (StataCorp LP). Two-sided p values < 0.05 were considered significant.
RESULTS
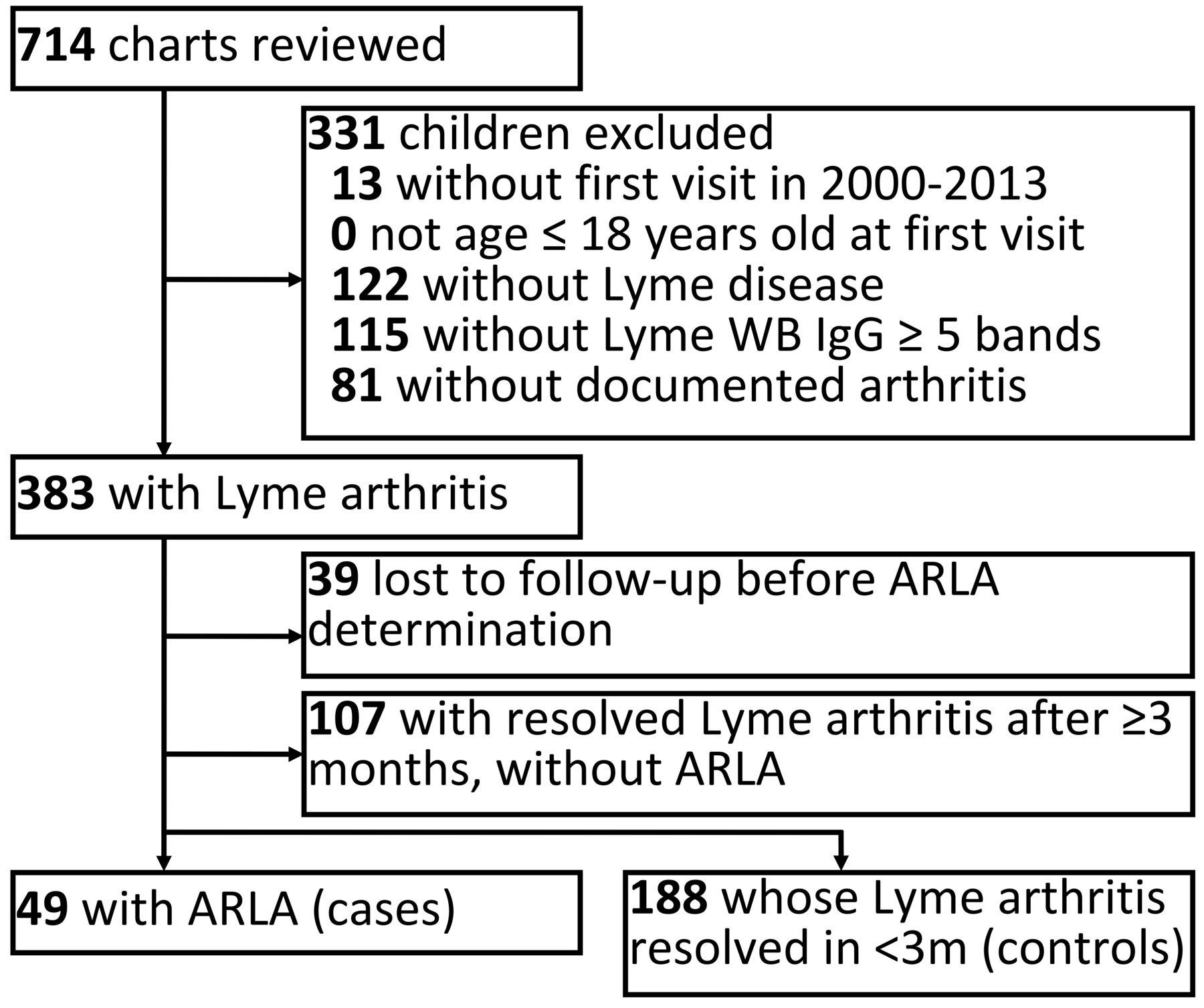
Of 383 children with LA, 49 children developed ARLA (cases), and 188 children had arthritis that resolved within 3 months after starting antibiotics (controls; Figure 1). Each center contributed different numbers of cases (n = 28, 7, 14) corresponding to their respective sample size, but the percentage of subjects with ARLA did not significantly differ across centers (18%, 23%, 30%; p = 0.19). Of the remaining 146 children with LA, 107 had LA resolve ≥ 3 months since starting antibiotics, and 39 were lost to followup before ARLA determination. Compared with children with faster resolution of arthritis, children with ARLA were more frequently older [median age 11.6 yrs (interquartile range; IQR 9.0–13.8) vs 9.0 yrs (IQR 6.9–11.8)] and less likely to be seen by pediatric rheumatologists early in treatment (Table 1). Children with ARLA were more likely to present with prolonged continuous joint symptoms [median 15 days (IQR 5–45) vs median 5 days (IQR 2–10)] and arthritis affecting a single knee (90% vs 63%). In contrast, children whose arthritis resolved within 3 months were more likely to present with fever (24% vs 16%), elevated erythrocyte sedimentation rate (ESR; 35% vs 16%), and severe pain (32% vs 6%), sometimes leading to hospitalization (16% vs 6%); 58% of controls had at least 1 feature of this severe phenotype versus 22% of cases. Many measured baseline characteristics did not differ between groups, including history of prior LD episodes or early LD symptoms, history of symptoms or diagnoses of autoimmune diseases, family history, or year of presentation. After starting antibiotics, children with ARLA were more likely to have markedly worsening arthritis, including new massive effusions, rupture of joint capsule or popliteal cyst causing painful lower leg swelling, or symptomatic recruitment of additional arthritic joints (20% vs 5%).
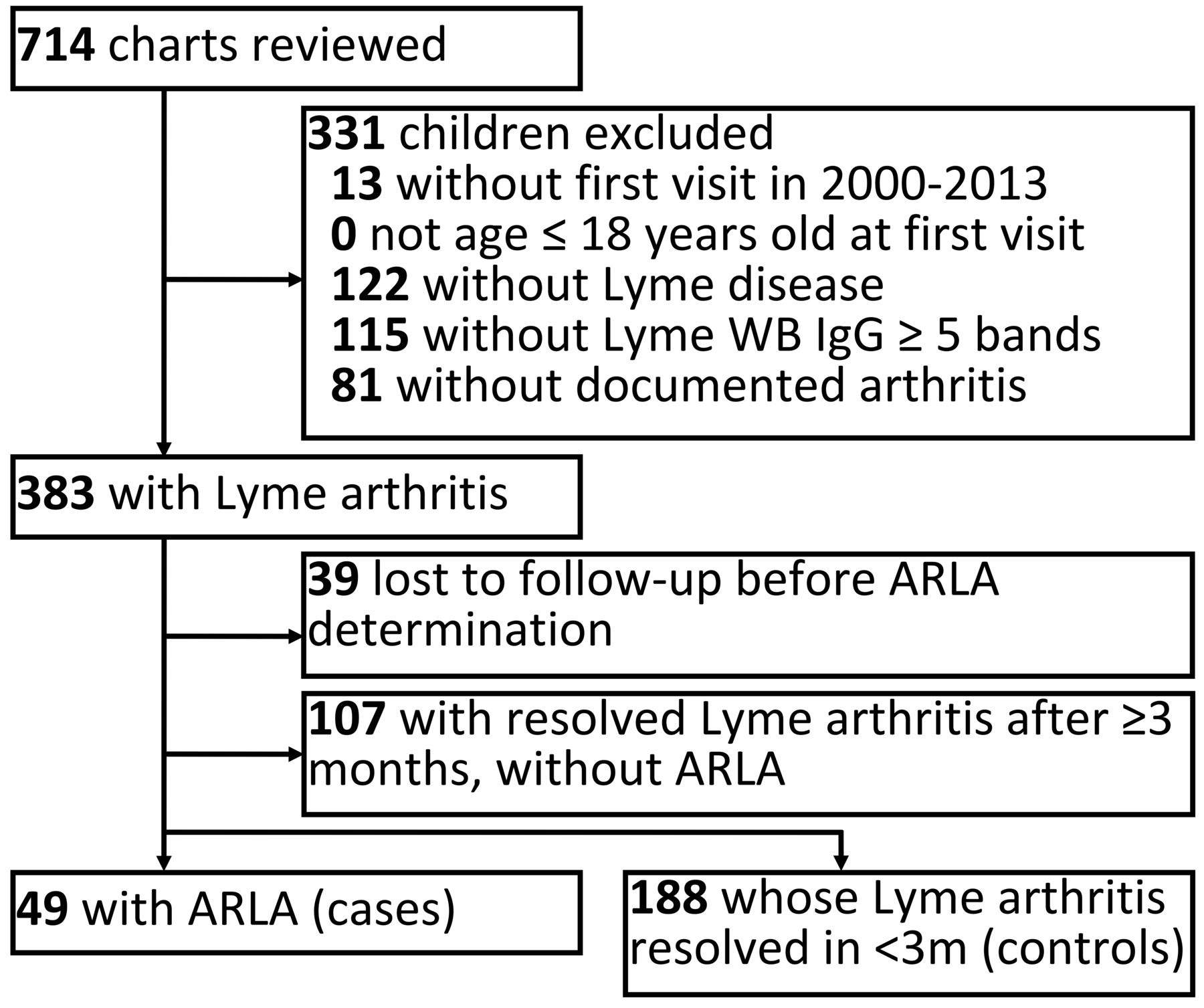
Subject selection diagram. This flowchart details the process of selecting 237 study participants (49 cases and 188 controls) after exclusion of 331 children without documented Lyme arthritis and 148 others who did not meet criteria for either cases or controls. ARLA: antibiotic-refractory Lyme arthritis; m: months; WB IgG: Western blot immunoglobulin G.
Characteristics of children with and without ARLA.
Regarding treatment characteristics, children with ARLA were less likely to receive antibiotics at guideline-recommended doses (usually amoxicillin) and more likely to report not taking most or all prescribed antibiotic doses. In contrast, there were no reported differences in antibiotic frequency (amoxicillin thrice daily vs twice daily) or early use of daily nonsteroidal antiinflammatory drugs (NSAID; Table 1). Children with ARLA were more likely to have taken doxycycline, consistent with their older ages (Table 2). Notably, among children age ≥ 8 years, a similar percentage of cases (65%) and controls (64%) took doxycycline as a first-line antibiotic (p = 0.91). Over half of cases were prescribed > 10 weeks of antibiotics, while controls were prescribed antibiotics for a median of 30 days (IQR 28–35). Cases were also more likely to receive IV antibiotics (57% vs 7%) and be prescribed NSAID at any point (80% vs 30%). Consistent with this higher treatment burden, reported adverse events during the antibiotic treatment period were more common among children with ARLA (37% vs 15%), including rash (18% vs 4%), headache (8% vs 1%), and hospitalization for adverse events [6% (3 cases) vs 1% (1 control)]. Reasons for hospitalization of cases were allergic reaction with rash, abdominal pain and vomiting from suspected biliary sludging, and allergic reaction plus a mechanical IV line problem (all with ceftriaxone); 1 control taking amoxicillin was hospitalized for rash.
Antibiotic use and treatment-associated adverse events among children with and without ARLA.
In primary multivariable analysis, 4 clinical factors were significantly associated with increased risk of ARLA: age ≥ 10 years (aOR 2.5, 95% CI 1.1–5.6), presence of continuous joint symptoms for ≥ 6 weeks at diagnosis (aOR 9.4, 95% CI 2.5–34.7), arthritis at diagnosis limited to one or both knees (aOR 5.1, 95% CI 1.4–19.2), and clinical worsening on initial antibiotic treatment (aOR 4.2, 95% CI 1.4–12.6; Table 3). In the same model, features of severe inflammation (fever, severe pain with or without hospitalization, or high ESR) were collectively associated with a decreased ARLA risk (aOR 0.4, 95% CI 0.2–0.9). There was no evidence of statistical interaction between age and other model variables (p > 0.1). In a separate model, 2 additional treatment-related factors — prescription of amoxicillin at subtherapeutic doses and poor reported antibiotic adherence — were also associated with ARLA (Table 3).
Association of explanatory factors with ARLA.
In sensitivity analyses, associations with all variables in the primary model remained consistent, but the effect size for certain variables was attenuated (Supplementary Table 3, available with the online version of this article).
Of 49 children with ARLA, 36 (73%) received ≥ 2 oral antibiotic courses. Fifteen of them subsequently received IV antibiotics. Nonantibiotic treatments (e.g., IAGC) and time to clinical resolution did not differ between children who did and did not receive ceftriaxone (Table 4). Six children had arthritis spread to new joints in the postantibiotic period, all of whom had received prior ceftriaxone (p = 0.03). Among children with ARLA, 4 of 5 children who received subtherapeutic oral antibiotics and 3 who were nonadherent to oral antibiotics also received ceftriaxone. Among 21 children who received oral but not IV antibiotics, 17 (81%) experienced clinical improvement with oral antibiotics alone. Four children (8% of children with ARLA) did not receive ceftriaxone despite lack of improvement after 2 courses of oral antibiotics, including 1 child with subtherapeutic amoxicillin. Exclusion of these 4 cases did not substantively change our results (Supplementary Table 3, available with the online version of this article).
Followup clinical characteristics of children with ARLA.
Among children with ARLA, half (24, 49%) had recurrent arthritis after full or clinical resolution of arthritis at a median of 273 (IQR 206–385) days after antibiotic initiation. Recurrences were more common after full, documented resolution of effusions (17) than in children with small, asymptomatic effusions (7). Children with fully resolved effusions did not differ from children with small, asymptomatic effusions in the number of prior antibiotic courses, number of prior IAGC injections, or time to first recurrence (p > 0.1).
DISCUSSION
In a large multicenter cohort of pediatric LA, we identified 4 of 9 hypothesized factors that were associated with increased risk of antibiotic-refractory disease: older age, arthritis limited to the knee(s), prolonged continuous joint symptoms, and clinical worsening at initial treatment. Of several factors hypothesized to decrease ARLA risk, we found that children who favorably responded to antibiotics more often had fever, severe pain, or other signs of systemic inflammation. Notably, not only did children with ARLA receive antibiotics for longer periods of time, but over half were prescribed more than 10 weeks of antibiotics despite treatment guidelines recommending no more than 6–8 weeks of antibiotics for LA3. The more intensive, prolonged treatment of children with ARLA was associated with higher rates of treatment-associated adverse events, including hospitalizations.
Our findings support prior research suggesting older age as a risk factor for ARLA in children6,7,8. The biologic basis for this finding is unclear. Doxycycline is used almost exclusively in older children and adolescents because of perceived risk of dental staining at earlier ages, but initial antibiotic choice did not explain the increased risk with age. Multiple lines of evidence suggest ARLA may be a postinfectious autoimmune condition, including associations of ARLA with HLA-DR417,18, genetic polymorphisms relating to immune response19, autoantibodies20, and pathogenic changes in regulatory T cells21,22 and Th17 cells23. ARLA may also result from immune dysregulation24 or abnormal immune response to persistent articular borrelial antigens25,26. The greater risk of older children to develop ARLA could relate to factors underlying the rising incidence of other autoimmune diseases in adolescence27. Further investigation should clarify whether the greater risk of ARLA among older children relates to one or more of these potential mechanisms. Our study also echoes previous research suggesting that new joint recruitment while taking antibiotics is a risk factor for ARLA in children8. Unlike the previous study, our definition of clinical worsening while receiving treatment also encompassed the development of massive effusions and rupture of large popliteal cysts, which we have observed clinically as other early prognosticators of treatment resistance.
Previous studies have not found any relationship between the duration of joint symptoms at diagnosis and ARLA in children6,7,10 or in a predominantly adult cohort5. We hypothesized that sustained arthritis at diagnosis would be associated with ARLA based on clinical experience. The positive finding in our study could relate to its larger sample size or differences in the study population (e.g., pediatric vs adult, United States vs Europe28) or design (comparators responding within 3 months) and bears replication. Others have observed that younger children with LA more likely present with fever and pain6, but our results suggest that systemic inflammatory response is a marker of favorable response to antibiotics irrespective of age. The mechanism behind this finding is unclear but may relate to more effective spirochetal killing among patients with high early levels of Th1- or Th17-associated cytokines29. Further, the association between knee-only arthritis and ARLA is also a novel, previously unreported finding.
We were unable to substantiate the previous observation that premature IAGC increases ARLA risk5,11. The few children we identified with early injections limited our ability to study this potential risk factor. We did find that children treated with insufficient doses of amoxicillin were more likely to develop ARLA, lending support for the recommended daily dosage in pediatric LA3,4. In contrast, outcomes did not differ when amoxicillin was prescribed twice daily instead of 3 times daily, as per treatment recommendations3,4. Notably, there was little deviation from guidelines in the prescribed dosage or frequency of doxycycline or ceftriaxone.
Treatment guidelines recommend that patients whose LA does not respond to oral antibiotics receive IV antibiotics3. Most patients in our cohort (all but 4) received care consistent with these recommendations, and exclusion of these 4 individuals from regression models did not change our findings. Further, children who received only oral antibiotics had similar outcomes compared with children who received IV ceftriaxone, except that children who received IV antibiotics were more likely to experience new postantibiotic joint recruitment. Our results support the notion that IV antibiotics may be required for adequate spirochetal killing in children who do not respond to oral antibiotics, even though IV antibiotic therapy does not prevent ARLA or the need for nonantibiotic treatment for all children. Given the lack of high-quality evidence about second-line treatment regimens, the risks of IV antibiotics, and the potential benefit of early IAGC injection for LA30, pediatricians should consider referring children to pediatric rheumatologists for LA that remains persistently active after 2 antibiotic courses.
Our study has several strengths. We assembled the largest cohort of pediatric LA to date across several referral centers in a Lyme-endemic region, giving us greater statistical power and generalizability to identify important clinical factors. Unlike similar previous studies, we focused on factors hypothesized to relate to ARLA, making our findings less likely to result from chance alone, and thus more scientifically credible. In addition, our study highlights the potential dangers of overtreating LA with antibiotics after the infection itself is cleared and antibiotics are ineffective5,31,32. This treatment-related risk is noteworthy because, in other settings, antibiotic use and antibiotic-associated dysbiosis may contribute to the development of acute and chronic arthritis in children33,34.
Our study also has several limitations. Given the setting at pediatric rheumatology referral centers, the study population and the high proportion of children with ARLA were not representative of all pediatric LA. For this reason, certain factors that we identified may relate to patterns of rheumatology referral more than ARLA risk, and our results may not generalize to all children with LA. Nonetheless, children with persistently active LA are commonly referred to pediatric rheumatologists, and results were similar across 3 centers with geographically and demographically distinct referral populations. A population-based case-control or cohort study would help further validate our findings. Another limitation was the high prevalence of missing data for certain variables, including baseline symptom duration, a primary explanatory variable associated with ARLA. Many children with ARLA were first seen in participating rheumatology clinics months after diagnosis, which led to higher rates of missing early clinical data. Nonetheless, we used available clinical data and referral patterns to impute missing data, and our findings were robust across multiple sensitivity analyses. Incomplete early documentation among many cases may also have underestimated nonadherence and the actual burden of early treatment toxicity. Finally, not all children were followed until full resolution of joint effusions, compatible with the clinical practice of participating centers. We found no evidence that recurrent arthritis was more common after incomplete resolution of effusions.
We identified several factors associated with the development of ARLA in children referred to pediatric rheumatologists, including older age, prolonged joint symptoms at diagnosis, knee-only arthritis, and clinical worsening on initial treatment. Children presenting with fevers or severe pain generally have more rapid and favorable response to antibiotics. Children with ARLA frequently receive multiple antibiotic courses, often exceeding current guidelines, resulting in more treatment-related toxicity. For children with persistently active LA after 2 antibiotic courses, pediatricians should consider starting antiinflammatory treatment and referring to a pediatric rheumatologist.
ONLINE SUPPLEMENT
Supplementary material accompanies the online version of this article.
Acknowledgment
The authors thank Jenna Tress for assisting with regulatory documentation and data collection. The authors also thank Meredith Buckley, Kelly Collier, Janille Diaz, Elizabeth Kaufman, Valerie Levy, Bernadette Lewcun, and Amanda Schlefman for collecting data.
Footnotes
This study was funded by the US National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS) of the National Institutes of Health (NIH) under award numbers F32-AR066461, L40-AR070497, and K23-AR070286, and the Eunice Kennedy Shriver National Institute of Child Health and Human Development of the NIH under award number T32-HD064567. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH, NIAMS, or the Eunice Kennedy Shriver National Institute of Child Health and Human Development.
Dr. Rose has received grant funding from GSK through a subcontract from the University of Leuven, Leuven, Belgium, for research unrelated to the present study.
- Accepted for publication October 9, 2018.








{kind=link}