

Abstract
Objective. To investigate the pathogenesis of pseudarthrosis in ankylosing spondylitis (AS) based on the pathological analysis of specimens harvested during surgery.
Methods. Radiographic and clinical data for 17 consecutive AS patients with pseudarthrosis were retrospectively analyzed. Meanwhile, the pathological analysis of specimens obtained during surgery was also performed.
Results. In total, 18 extensive Andersson lesions were included. Pseudarthrosis located at the apical region were noted in 12 patients. Complete ossified anterior longitudinal ligaments above or below pseudarthrosis and fracture through posterior elements or facet joints were observed in 7 and 6 lesions, respectively. The most definitive pathological characteristic in all cases was proliferating hypovascular edematous fibrous tissue involving disc, bone-disc border, and vertebral body. Fibrinoid necrosis, necrotic bone fragments, hemosiderin deposits, and active subchondral osteogenesis were found, indicating trauma process. Mild perivascular collections of inflammatory cells were detected in only 2 cases.
Conclusion. AS-related pseudarthrosis is more likely to originate from mechanical trauma than inflammation. The above-mentioned radiological and histological findings showed that multiple mechanisms lead to the formation of pseudarthrosis. These mechanisms include excessive stress, insufficiency fracture, and an acute fracture involving a 3-column structure.
Ankylosing spondylitis (AS) is a common chronic inflammatory disorder that mainly affects the spinal column and sacroiliac joints1. In the advanced stage of AS, progressive ossification often produces a fixed and rigid thoracolumbar kyphotic deformity. Spinal pseudarthrosis, a well-known complication of AS, was first described by Andersson in 1937 (named Andersson lesion; AL)2. In 1996, an epidemiological investigation of 147 consecutive AS patients was performed by Kabasakal, et al3. In that study, 12 individuals (8%) with spondylodiscitis involving 32 disc spaces were identified. In 2000, Scarpa4 evaluated the destructive abnormalities in psoriatic arthritis following Cawley’s classifications. Thus, destructive erosions and lesions of the discovertebral junction were identified in 12 patients (12.0%) and seemed to be a characteristic aspect of spondyloarthropathies. Since then, the different terms that have been used to refer to these lesions, including spondylodiscitis, destructive lesion, discitis, or pseudarthrosis, reflect the existence of an ongoing debate regarding the exact etiology of AL2,5,6,7.
Before the 1970s, the term spondylodiscitis was used to describe an inflammation-related etiology of AL. Wholey, et al5 was the first to describe findings in biopsies obtained from 2 patients with AS, stating that the observed changes were consistent between the samples and indicated a chronic inflammatory process. In a more detailed pathological investigation of 1 patient with AS, Hansen, et al6 reported the finding of nonspecific granulomatous inflammatory tissue, also favoring a purely inflammatory origin. However, the relevant changes documented by other authors have included the replacement of bone by fibrous tissue or hemosiderin deposits, both of which indicate that traumatic factors might be involved in the pathogenesis of AL7. Thus, a theory that combined inflammatory processes with mechanical effects on the spinal column became more widely accepted in the early 1980s. Nevertheless, in a study of 35 patients with AS published by Fang, et al, trauma without an inflammatory element was assumed to be the primary cause of extensive lesions based on detailed histological observations of 8 specimens8. Because the above-mentioned studies of pseudarthrosis complicated with AS are largely limited to isolated case reports, a more detailed and comprehensive analysis of pathogenesis is clearly needed. The purpose of our study was to investigate histological findings in radiologic examinations and determine the exact etiology underlying pseudarthrosis.
MATERIALS AND METHODS
Medical records of 75 consecutive AS patients with pseudarthrosis who underwent surgery between January 2001 and December 2016 were reviewed. The inclusion criteria were the following: (1) radiograph, computed tomography (CT), and magnetic resonance imaging (MRI) data were available; and (2) tissue specimens around pseudarthrosis were obtained intraoperatively. Tissue specimens could be obtained in patients by osteotomy through pseudarthrosis, debridement, or decompression around the pseudarthrosis, instead of posterior instrumentation only. Finally, 17 patients with 18 extensive vertebral lesions were included in our study. In this paper, regarding the location of pseudarthrosis, apex was defined as “apical region of global kyphosis (GK).” Meanwhile, above and below were defined as “above the apex of GK” and “below the apex of GK,” respectively. The other 58 patients were excluded because the detected pseudarthroses were not located at the apical region of GK, and severe spinal cord impingement was not identified in these cases; thus, debridement or decompression around the lesions were not performed and tissue specimens were not available (Supplementary Table 1, available with the online version of this article). All lesions were confirmed on anteroposterior and lateral radiographs, CT, and MRI. An excision of the intervertebral disc and part of the adjacent vertebral body was achieved intraoperatively. GK was defined as the “angle between the superior endplate of the maximally tilted upper end vertebra and the inferior endplate of the maximally tilted lower end vertebra on full-length lateral radiographs.1” GK > 50° was regarded as indicative of thoracolumbar kyphosis. This study was approved by the Medical Ethics Committee of our hospital (ethics approval number 2011052), and written informed consent was obtained from all patients prior to testing.
Clinical features
At the time that pseudarthrosis was documented, 12 patients showed rigid thoracolumbar kyphosis. Persistent localized back pain around the lesion was noticed and these symptoms were aggravated when walking but relieved after lying down. The neurological functioning of 17 patients is listed in Table 1. It should be noted that pseudarthrosis frequently involves 3 columns of the spine and is at high risk of spinal instability, thereby leading to the compression of the spinal cord. Thus, surgical intervention should be taken into consideration immediately if patients have progressive myelopathy symptoms and neurological deficit secondary to the spinal instability of those pseudarthrotic lesions. All 17 patients included received only nonsteroidal antiinflammatory drugs (NSAID) to reduce the abnormal inflammatory markers to normal values before surgery. In our present study, the administration of NSAID preoperatively is aimed to relieve the pain and provide a favorable condition for surgery. Recently, Molnar, et al9 analyzed 432 patients with AS for the effect of tumor necrosis factor inhibitors on spinal structural changes. They concluded that the structural damage and radiographic progression can be suppressed only if the treatment with antiinflammatory drugs were used for over 2 years. Also, Haroon, et al10 demonstrated that high NSAID intake for more than 2 years may show benefits for the progression of structural changes in patients with AS. To our knowledge, pseudarthrosis is known as a late complication for AS patients with a longstanding disease course. Thus, the application of antiinflammatory medication for a short period before surgery may not have an effect on the biopsy. No evidence of bacterial infection or tuberculous spondylitis was detected in these patients.
General information and clinical data (n = 17).
Treatment
Four surgical strategies were adopted for these 17 patients (Table 1).
RESULTS
A total of 14 men and 3 women ranging in age from 29 to 60 years were included. Radiographs and CT scans were available in all cases, while MRI data were obtained for 13 of the patients (76%). For the 2 surgical specimens from the same patient, the radiological and pathological manifestations of the lesion were identical.
Radiographs
The average preoperative GK was 69.4° ± 24.8° (range 32° to 114°). Twelve patients were regarded as having thoracolumbar kyphosis. All lesions were observed in the thoracolumbar and lumbar region between T9 and L5. Lesions located at the apex of thoracolumbar kyphosis were noted in 12 patients. The most striking radiographic feature of pseudarthrosis is osteolytic destruction of the vertebral endplate and adjoining reactive sclerosis extending into the vertebral bodies. In 7 lesions, bridging syndesmophytes were noted above and below the pseudarthrosis. A fracture through the posterior elements or unfused facet joints combined with opposite anterior lesions were observed in 6 patients.
CT scans
Irregular central discovertebral osteolysis with a reactive sclerotic zone was identified in nearly all the lesions. Vacuum phenomenon and paraspinal swellings were noted in 11 lesions. Lesions extending into the posterior elements led into the narrow of the spinal canal in 3 cases. Among these lesions, vertebral body dislocation was detected in 1 case. The gap through posterior element and unfused facet joint in 6 lesions revealed the fracture line more accurately in comparison to radiographs.
MRI
Hypointense signal intensity of the vertebral lesion margins at the level of AL was noted in T1- and T2-weighted images. A decreased spinal canal was caused by anterior extradural tissue or posterior hypertrophic ligamentum flavum in 9 pseudarthrotic lesions. Among these lesions, obvious compression of the spinal cord was documented in 4 cases. Moreover, concurrent edematous paraspinal and soft tissue invasions were identified in the posterior element, which showed mixed or decreased intensity in T2-weighted images.
Mechanical trauma
Normal disc tissues were replaced by fibrous tissue without recognizable preserved nucleus pulposus. Proliferating fibroblastic tissue that extended into the disc-bone border or subchondral structure was observed in 11 cases. The hyaline cartilage was replaced by fibrous materials, showed degenerative changes and developed into fibrocartilage in 6 lesions (Figure 1A). In the inner portion of the fibrous tissue and fibrocartilage, extensive fibrinoid necrosis was frequently observed and associated with a loss of chondrocyte nuclei (Figure 2B). Occasionally, necrotic bone fragments enclosed within collagenous tissue in the peripheral disc space indicated a previous traumatic process. In addition, hemosiderosis was detected in the outermost part of the fibrocartilage in 4 lesions, demonstrating old and repetitive hemorrhage caused by a previous trauma (Figure 1B).
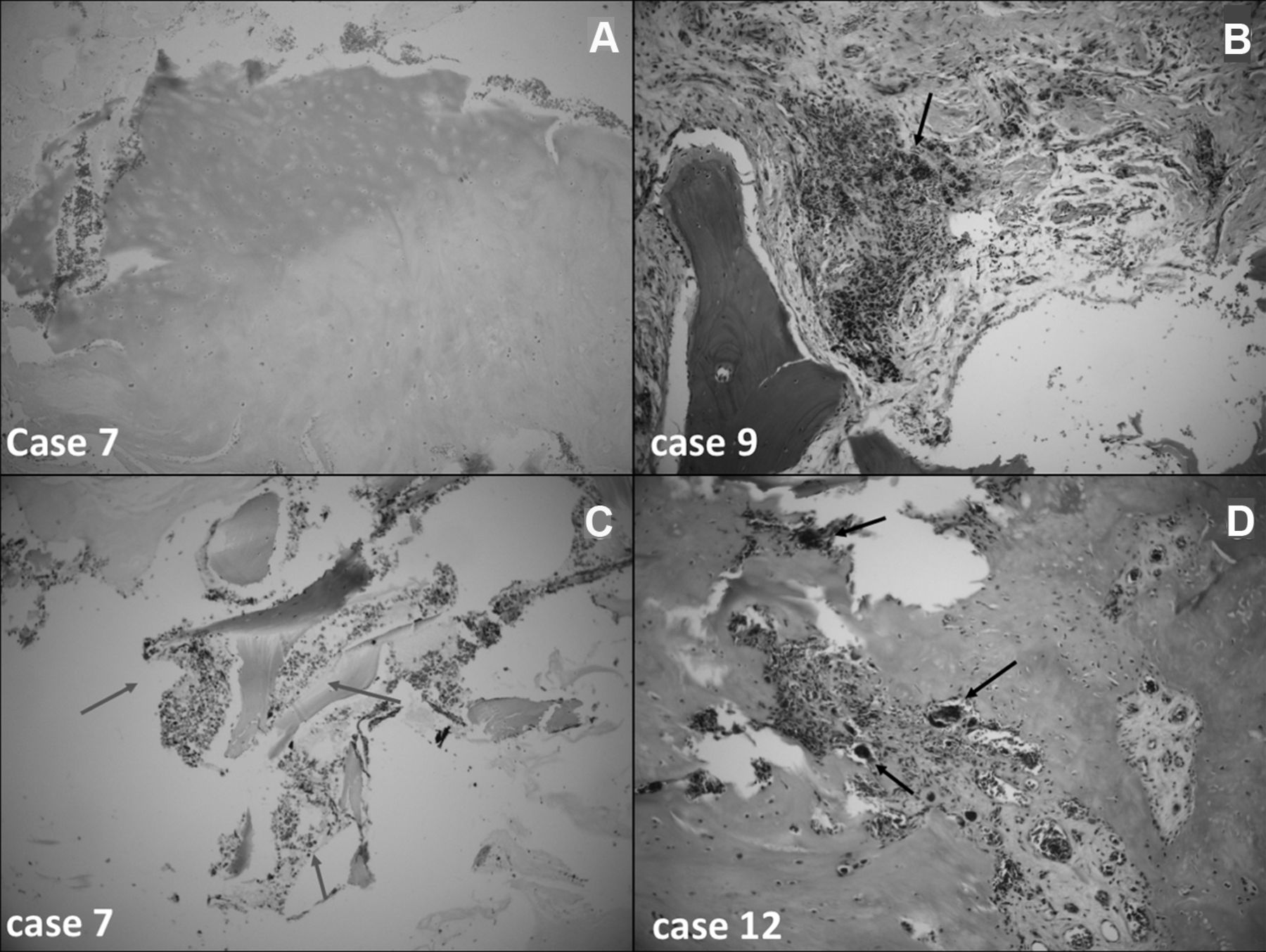
Evidence of mechanical trauma. A. Hyaline cartilage replaced by fibrocartilage. B. Hemosiderin deposit (arrow). C. Scanty perivascular inflammatory cellular infiltration (arrows). D. Active osteoclastic resorption and widespread osteoblasts infiltration (arrows) at the disc-bone border. (A–C H&E; original magnification × 10. D. × 20).

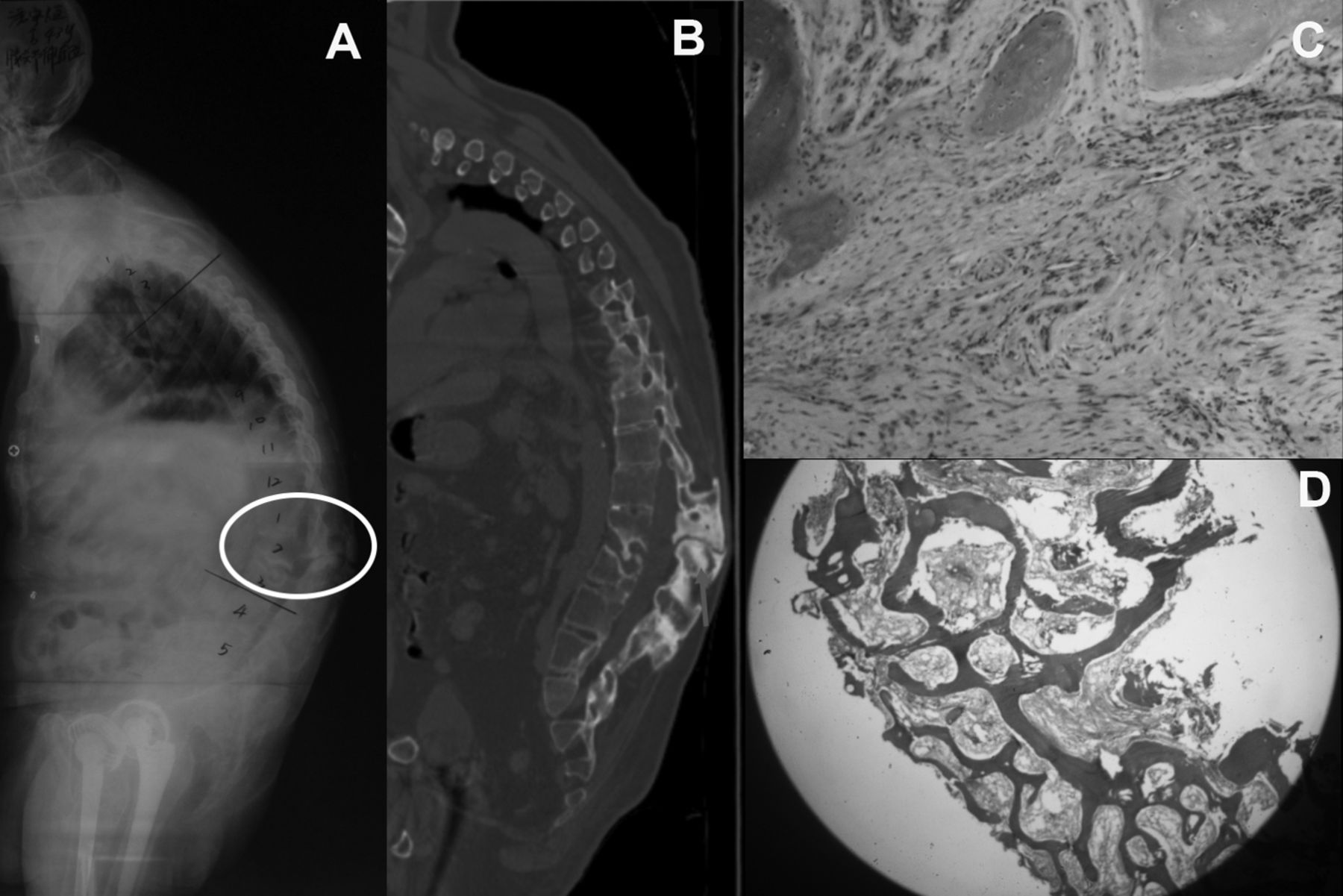
A 41-year-old male with pseudarthrosis at the apex (T10/11). Completely ossified anterior longitudinal ligaments (A) above and (B) below pseudarthrosis. C. Extensive fibrinoid necrosis implied that excessive stress had been applied to the skipped segment. D. Fibrous tissue bearing capillary congeries indicated an ongoing reparative process (arrows). (C–D H&E, × 10).
Fibrous repair
The observed disc changes were consistent across all the lesions. In the intervertebral disc space, the normal structure was completely converted into hypovascular edematous fibrous scar tissue. In 7 lesions, proliferating reparative fibrous tissue had grown from the bone marrow, leading to the erosion and breach of the endplate. Moreover, the increased reversal lines disrupted the disc-bone border, making it unidentifiable. In an attempt to repair the posttraumatic necrotic zones and degenerative cartilaginous tissue, multiple laminae-bearing vessels merged with collagen fibers extending into the vertebral body; these could be observed microscopically in 6 cases. The presence of capillary congeries also revealed that a typical fibrous repair process was ongoing (Figure 2D). Scanty and mild perivascular inflammatory cellular infiltration (e.g., by monocytes, lymphocytes, and plasma cells) was noted in only 2 cases (Figure 1C).
Bony repair
Osteogenesis was more likely to occur near the endplate region instead of the disc space. Focal active osteoclastic resorption is the initiating process of bony repair and was observed in nearly all cases (Figure 1D). Further, chondroid and osseous metaplasia, indicated by widespread infiltration by osteoblasts at the disc-bone border, were also helpful clues to the pathogenesis of pseudarthrosis. Capillary vessels were frequently noted in regions of active osteogenesis. In 5 lesions, clear calcium deposits were observed in the margins of regenerative fibrocartilage, implying that bone formation was an ongoing process. Woven bone was frequently encountered in these lesions, which was the evidence of fracture (Figure 3D).
A 43-year-old female developed pseudarthrosis (A) below the apical region (L2/3). B. An acute fracture through the posterior elements was noted at the ankylosed spinal column. C. Fibrous tissue growing from the bone marrow indicated an active bony reparative process. D. Detected hemosiderin deposition in the outermost part of the fibrocartilage exhibited evidence of old hemorrhage. Woven bone revealed ongoing osteogenesis. (C–D H&E, × 10).
DISCUSSION
Spinal pseudarthrosis is an uncommon but well-recognized condition that occurs in the late stage of AS8. The prevalence of AL ranges from 1 to 28%11,12,13. Since Andersson published the first report of AL in 19372, various terms have been used to describe these lesions. An infectious origin was initially suggested by some authors because of the radiological resemblance between AL and spondylodiscitis14. However, this assumption was not widely accepted because positive cultures were not detected. In a study of 2 patients, Wholey, et al5 was the first to report relevant findings from biopsies. These data showed that the etiology of AL may involve a chronic inflammatory process (Table 2). In 1967, Hackenbroch15 also noted nonspecific inflammation with cell infiltration, which supported a primary inflammatory origin for AL. However, further histological investigations favoring an inflammatory etiology are rare. In 1972, Cawley, et al11 categorized AL into 2 types, localized and extensive lesions. In previous studies, localized lesions were regarded as originating from inflammation and part of a normal AS course16. However, whether inflammatory or traumatic factors are important to the development of extensive lesions (so-called pseudarthrosis) remained unclear. Thus, in our study, we sought to correlate pathological and radiographic findings with inflammatory or traumatic etiologies to determine the specific pathogenesis of pseudarthrosis (Supplementary Tables 2 and 3, available with the online version of this article).
Overview of histological appearances of tissue obtained from AL reported over the past 60 years.
In our current study, a pseudarthrosis located at the apical region of GK was noted in 12 out of 17 patients. It is conceivable that in these patients, the apical region of their fixed and kyphotic spine was subjected to the highest level of stress16. As thoracolumbar kyphosis progressed in advanced AS, repeated stress may have led to the extensive and severe destruction of the discs and resulted in fatigue fractures8,17. Therefore, in fibrous tissue with mild inflammation, the inflammation was most active in the intervertebral disc space, where the normal structure of the disc was totally destroyed and unrecognizable in all of the lesions. These pathological observations are also strongly reflective of the reparative process that occurs after mechanical trauma16. Moreover, widespread cartilaginous degeneration and necrosis were identified in the lesions in these cases. These findings suggest that the tissues had been exposed to repetitive stress and that the fibrocartilage showed higher resistance than hyaline cartilage to trauma. In 7 cases, the spinal segments above and below the pseudarthrosis were completely ossified and showed bridging syndesmophytes anterior to the lesion. The movement of the ankylosed spine was focused on the isolated segment, consistent with “the last mobile segment principle” proposed by Wu, et al17. The skipped segment was consequently exposed to abnormal and excessive stress because of these long lever arms, and this caused a mechanical failure similar to that observed in a long bone fracture. Fibrinoid necrosis was also observed in these cases under microscopic examination, revealing undue stress on the tissues in this area. Generally, the bone and disc space are more susceptible to shearing forces than compressive forces8. Persistent motion at the isolated segment and the loss of structural support caused by the destruction of the fibrous annulus and nucleus pulposus may continue to produce damage, and may hinder repair of the fracture, resulting in the development of an unstable pseudarthrosis. Sclerotic subchondral bone at the level of the pseudarthrosis is evidence of an unfused spinal segment17,18.
Apart from mechanical trauma at non-ankylosed segments, other mechanisms that could potentially lead to the formation of pseudarthrosis included an acute fracture through the ankylosed spine. Because the entire spine is osteoporotic and stiff in AS, a minor trauma can cause a transvertebral, discovertebral, or transdiscal fracture16. In agreement with previous studies, we found that a fracture might initially occur in the posterior column prior to the development of anterior discovertebral lesions, especially when the patient is in a hyperflexion position, because this causes the greatest amount of posterior tension force1,7,8. In our present study, a microfracture through a posterior element that exhibited unfused facet joints was identified in 6 patients. Hemosiderin deposits, scattered necrotic bone fragments, and active osteoclasts and osteoblasts were concurrently detected in these cases, which was consistent with an old fracture and the natural healing process16,17,19,20. In AS patients with a longstanding disease course, inflammation frequently weakens the bony structure, leading to the vertebral body being susceptible to mechanical trauma. Therefore, undue or excessive stress is more likely to develop a pseudarthrotic lesion. In this case, inflammation appears to be the cause of the formation of pseudoarthrosis; however, trauma should instead be regarded as the predominant factor. Further, scant and mild inflammation was frequently accompanied by capillary congeries or vessels and was regarded as a reaction to trauma that played a secondary role in the pathogenesis of pseudarthrosis in AS. These findings support the observations made by Fang, et al8. Hence, for patients with AS in the advanced or late stage, trauma, farm work, and heavy labor that might lead to the development of trauma-originated pseudarthrosis should be avoided.
Although the findings of our study would appear to be partially consistent with the previous studies, we acknowledge the strengths of our study. We were able to (1) analyze the detailed correlation between distinctive radiological features and pathological findings, making multiple mechanisms completely understandable; (2) assess more histological changes as indicators in comparison to the previous literatures, such as woven bone, regenerative fibrocartilage replacing hyaline cartilage, and the like, which can provide a comprehensive understanding of the exact etiology; (3) include the largest amount of tissue specimens and pathological sections, making the pathological observations more persuasive; and (4) exhibit natural history of pseudarthrosis by characteristic radiological data, showing a clear trauma-related process in the formation of pseudarthrosis (Figure 4). The limitations of our study were its retrospective design and a failure to identify an association between clinical data and pathological analysis. Also, the target group mainly involving apex lesions is indeed one of the limitations of our study. The lesions near the apex are also subject to undue stress apart from the apical region, and are likely to result in formation of pseudarthrosis. In our current study, it could be concluded that the formation of apex lesions in AS is attributed to traumatic etiology. However, there were only 5 cases with pseudarthrosis located outside the apical region and because of the small sample size, it was hard to draw a persuasive conclusion for these lesions. Therefore, a better analysis involving more cases with lesions around the apex should be conducted in future investigations to distinguish whether inflammatory or traumatic factors play an important role. Further study using molecular biological methods to investigate the etiology of this condition is certainly warranted.
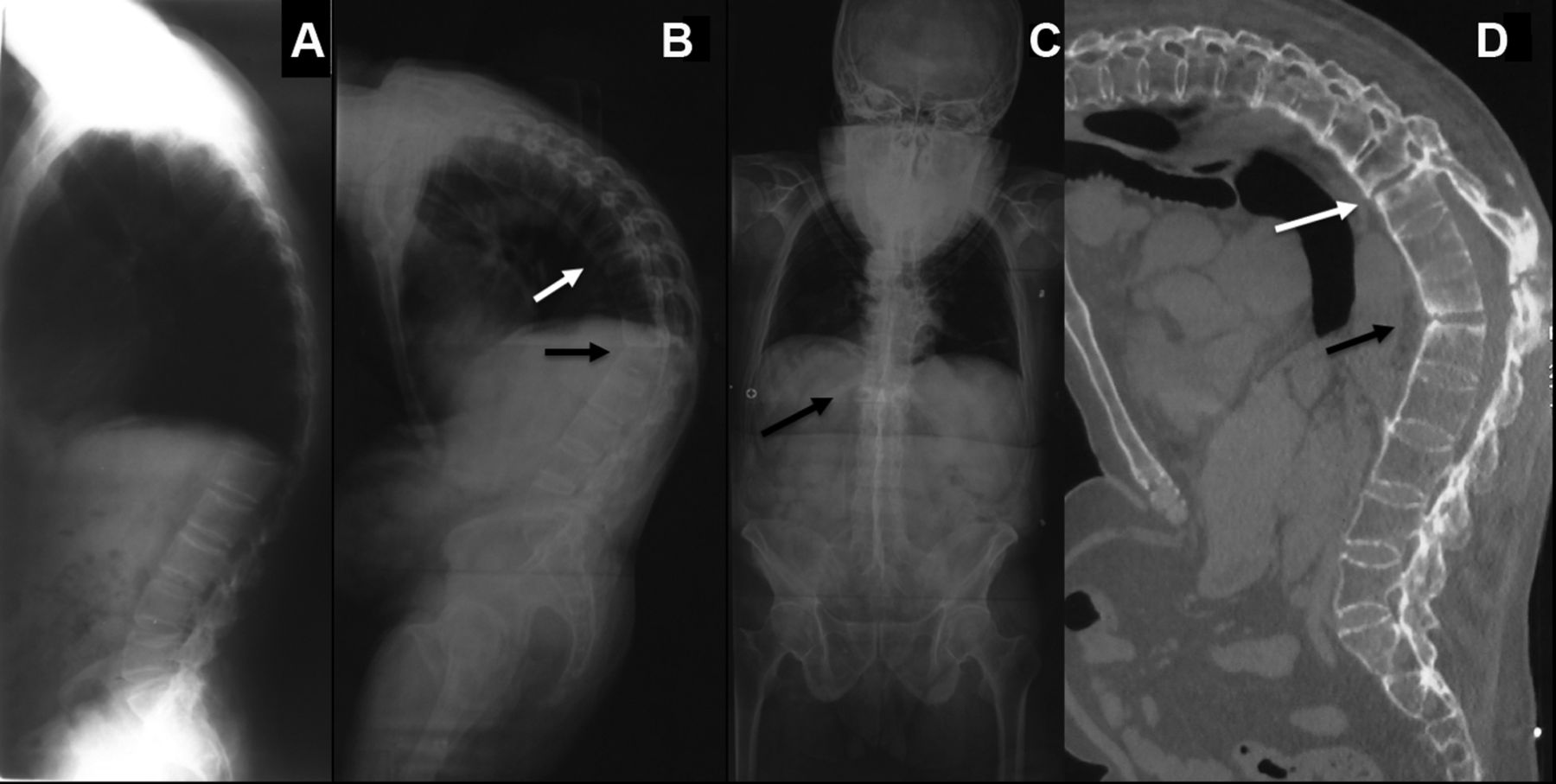
Natural history of pseudarthrosis. A. Initial visit of a 34-year-old male without detected pseudarthrosis. At 11-year followup, the patient had developed pseudarthrosis [B–D, T9/10 (white arrows) and T12/L1 (black arrows)] and exhibited progression of thoracolumbar kyphosis. D. CT sagittal reconstruction image showed the formation of pseudarthrosis involving 3 columns (black arrow). CT: computed tomography.
The traumatic etiology of spinal pseudarthrosis in AS can be histologically confirmed by the presence of mechanical trauma, fibrous, and bony repair. Moreover, a traumatic origin can be established based on evidence of multiple biochemical mechanisms, such as those involved in the “last mobile segment principle,” repetitive stress, and acute fracture. Finally, no pathological evidence of primary inflammatory origin was noted in these cases. Hence, pseudarthrosis is more likely to have originated as a result of mechanical trauma than inflammation.
ONLINE SUPPLEMENT
Supplementary material accompanies the online version of this article.
Footnotes
Financial support from the Key Provincial Talents Program of Jiangsu Province, the Jiangsu Provincial Key Medical Center (ZX201107), and the National Natural Science Foundation of China (81372009).
- Accepted for publication June 21, 2018.








{kind=link}
{kind=link}
{kind=link}
{kind=link}