

Abstract
Objective. To assess the prevalence of myofascial inflammatory lesions visible by magnetic resonance imaging (MRI) and their changes after tocilizumab (TCZ) therapy in active polymyalgia rheumatica (PMR).
Methods. We conducted a posthoc analysis of data from the TENOR study of TCZ monotherapy in PMR. The 18 patients each received TCZ injections at weeks 0, 4, and 8. The shoulder and pelvic girdles were assessed at baseline then at weeks 2 and 12 using T1- and T2- short-tau inversion recovery–weighted MRI. Radiologists blinded to patient data assessed each muscle group for localized myofascial inflammation on baseline, Week 2, and Week 12 MRI. Reproducibility was estimated by having 2 radiologists assess the Week 2 MRI of 13 patients, then computing the κ coefficient.
Results. For myofascial lesion detection, intraobserver reproducibility was almost perfect (κ = 0.890) and interobserver reproducibility was substantial (κ = 0.758). At baseline, all patients had at least 1 inflammatory myofascial lesion; sites involved were the shoulder in 10 (71.4%) patients, hip in 13 (86.7%), ischial tuberosity in 9 (60.0%), and pubic symphysis in 12 (80.0%). Sites involved at Week 12 were the shoulder in 8 patients (53.3%), hip in 5 (33.3%), ischial tuberosity in 1, and pubic symphysis in 3 (20.0%). At Week 12, of 103 muscle groups studied in all, 43 (41.7%) had no inflammatory lesions, compared to 33 at baseline (p = 0.002); improvements were noted in 66 (64.1%) muscle groups, worsening in 2 (1.9%), no change in 35 (34.0%; p = 0.034).
Conclusion. Localized myofascial inflammatory lesions are common in recent-onset PMR and improve during TCZ therapy. Clinicaltrials.gov (NCT01713842).
Polymyalgia rheumatica (PMR) is an inflammatory disease of unknown origin whose onset usually occurs after 50 years of age1 and whose main symptoms are inflammatory pain in the shoulder and pelvic girdles with prolonged morning stiffness. When combined with laboratory evidence of systemic inflammation, these symptoms strongly suggest PMR in patients without other causes of inflammation. A rapid response to systemic glucocorticoid therapy, which is the current treatment of reference, confirms the diagnosis2,3.
Longterm glucocorticoid therapy induces adverse events4. Other treatment options are therefore needed, particularly for patients who have risk factors for intolerance to systemic glucocorticoids (osteoporosis, diabetes, hypertension) or become steroid-dependent. Tocilizumab (TCZ) is a monoclonal antibody that inhibits the proinflammatory mediator interleukin 6. In the TENOR study, first-line TCZ monotherapy was effective in patients with recent-onset PMR5. Thus, TCZ may hold promise as an alternative to glucocorticoid therapy in selected patients with PMR6,7,8. Magnetic resonance imaging (MRI) is highly sensitive for detecting inflammatory lesions9. Thus, most patients in the TENOR study had MRI signs of synovitis (effusion in glenohumeral and coxofemoral synovitis) or bursitis (subacromial bursitis at shoulders, trochanteric and iliopsoas bursitis at hips) at baseline (the proportions of shoulders and hips with bursitis were 93 and 100% and the corresponding proportions for intraarticular effusions/synovitis were 100 and 100%), which improved with TCZ therapy10.
The MRI performed for the TENOR study showed evidence of localized myositis and fasciitis at the shoulder and pelvic girdles. In everyday practice, myofascial lesions are not usually evaluated on MRI obtained for patients with PMR.
The primary objective of our study was to assess the prevalence and changes under TCZ therapy of myofascial lesions visualized by MRI at the shoulder and pelvic girdles in patients with active recent-onset PMR.
MATERIALS AND METHODS
Patients
The population of the TENOR study is described elsewhere5. Briefly, patients were enrolled prospectively at the university hospital in Brest, France. Inclusion criteria were PMR meeting Chuang’s criteria11, onset within the past 12 months, active disease defined as PMR Disease Activity Score (PMR-AS) > 1012, no history of glucocorticoid therapy longer than 1 month and stopped at least 7 days before inclusion, age 50–80 years, C-reactive protein (CRP) > 10 mg/l and/or erythrocyte sedimentation rate (ESR) > 40 mm/h, and no evidence of other inflammatory rheumatic or connective tissue disease. PMR-AS was computed as the sum of morning stiffness in minutes, elevation of the upper limbs rated 0–3, physician’s global assessment on a 10-point visual analog scale (VAS), pain intensity determined by the patient on a 10-point VAS, and CRP level in mg/dl. Any nonsteroidal antiinflammatory drug therapy had to be stopped at least 2 days before inclusion. Exclusion criteria were clinical symptoms suggesting giant cell arteritis, immunosuppressive therapy, uncontrolled dyslipidemia or cardiovascular disease, chronic infection, evidence of hydroxyapatite crystal disease, chondrocalcinosis or severe osteoarthritis (OA) of the hip and/or shoulder, symmetrical peripheral arthritis, active thyroid disease, and drug-related myalgia. Each patient received a TCZ injection at weeks 0, 4, and 8, without glucocorticoid therapy.
The study received ethics committee approval and all patients provided written informed consent before study inclusion. The protocol was registered on Clinicaltrials.gov (NCT01713842).
MRI protocol details
A 3T Philips Achieva was used, with a 32-channel surface antenna, to image the shoulder and pelvic girdles at weeks 0, 2, and 12. Three sequences were used: axial T1 turbo spin echo (TSE), axial T2 short-tau inversion recovery (STIR), and coronal T2 STIR. Axial TSE variables were as follows: repetition time (TR), 659 ms; echo time (TE), 20 ms; slice thickness, 4 mm; matrices, 828 × 420 for the shoulders and 720 × 404 for the pelvis; and fields of view (FOV), 53 × 32 cm for the shoulders and 46 × 31 cm for the pelvis. For the axial T2 STIR sequence, TR was 2721 ms, TE 75 ms, slice thickness 4 mm, matrices 524 × 210 (shoulders) and 468 × 264 (pelvis); and FOV 47 × 28 cm (shoulders) and 46 × 35 (pelvis). Finally, for the coronal T2 STIR sequence, TR was 4828 ms, TE 65 ms, slice thickness 5 mm (shoulders) and 4 mm (pelvis), matrices 328 × 382 (shoulders) and 356 × 420 (pelvis), and FOV 32 × 48 cm (shoulders) and 35 × 52 cm (pelvis).
Data collected
Myofascial lesions were defined as a high T2 STIR signal that was either diffuse within the muscle or formed a line surrounding the muscle. Enthesitis, tendinitis, and bursitis were not evaluated in the current study. At the shoulder girdles, myofascial lesions were sought at the infraspinatus, supraspinatus, subscapularis, and teres minor muscles. At the pelvic girdles, the sites assessed for myofascial lesions were the gluteal, iliopsoas and pelvitrochanteric muscles at each hip; the semitendinosus, semimembranosus, and long head of the biceps femoris at each ischial tuberosity; and the adductors at the pubic symphysis. Thus, 7 muscle groups were studied in each patient. A muscle group was considered positive if at least 1 muscle in the group showed a lesion.
Reading
The MRI were read by 2 radiologists, one senior (FG) and the other junior (JPL), who were blinded to all patient data and worked independently from one another. To allow an estimation of intraobserver repeatability and interobserver reproducibility of myofascial lesion detection, each radiologist assessed the Week 2 MRI on 2 separate occasions. To allow a similar assessment for the change in MRI findings over time, the Week 0 and Week 12 MRI were read once by both radiologists, who recorded the findings as no change, worsening, or improvement.
For the description of myofascial lesions, when the 2 radiologists disagreed, they worked together to reach a consensus.
Statistical analysis
Categorical variables were described as n (%). Intraobserver and interobserver reproducibility was estimated by computing Cohen’s κ coefficients, which were interpreted as follows: slight, 0–0.20; fair, 0.21–0.40; moderate, 0.41–0.60; substantial, 0.61–0.80; and almost perfect, 0.81–1. To compare values between 2 timepoints, we used the Wilcoxon signed-rank test for paired data and the chi-square test or McNemar test for categorical variables. All statistical tests were performed with SPSS 24.0, version 2016 (SPSS Inc.).
RESULTS
Patients
We included 18 patients, 11 men and 7 women, with a mean age of 71 years (SD 58–83 yrs) and a mean body mass index of 28 ± 1 (kg/m2). All patients met both Chuang’s criteria and those of American College of Rheumatology/ European League Against Rheumatism (ACR/EULAR)13.
At baseline, 16 patients (89%) had shoulder girdle pain and 16 (89%) had pelvic girdle pain; at 12 weeks, these numbers had dropped to 5 (28%) and 3 (17%), respectively. Mean VAS pain score was 6 ± 0.5 at baseline and 2.2 ± 0.4 at 12 weeks. Mean serum CRP was 82 ± 16 mg/l at baseline and 3 ± 12 mg/l at 12 weeks. Mean PMR-AS was 38 ± 2 at baseline and 7 ± 1 at 12 weeks. Table 1 shows the evolution (median and interquartile range) during treatment by TCZ.
Clinical evolution during the tocilizumab period.
Repeatability and reproducibility of MRI assessments of localized myofascial lesions
MRI was performed at Week 2 in 13 of the 18 patients. Thus, in all, 91 (or 13 × 7) muscle groups were assessed for the presence of localized myofascial inflammatory lesions. Intraobserver reliability (κ = 0.890, 95% CI 0.842–0.938; and 0.846, 95% CI 0.79–0.902 for the senior and junior rheumatologist, respectively) was almost perfect and interobserver reliability was substantial (κ = 0.758, 95% CI 0.69–0.826).
MRI at weeks 0 and 12 were available for 15 patients (Table 2, Figure 1, and Figure 2); however, in 1 of those patients, severe shoulder pain precluded MRI of the shoulder girdle at Week 0. Thus, 103 muscle groups were studied in all. Interobserver reproducibility of the change between weeks 0 and 12 was moderate to substantial (κ = 0.601, 95% CI 0.522–0.680).
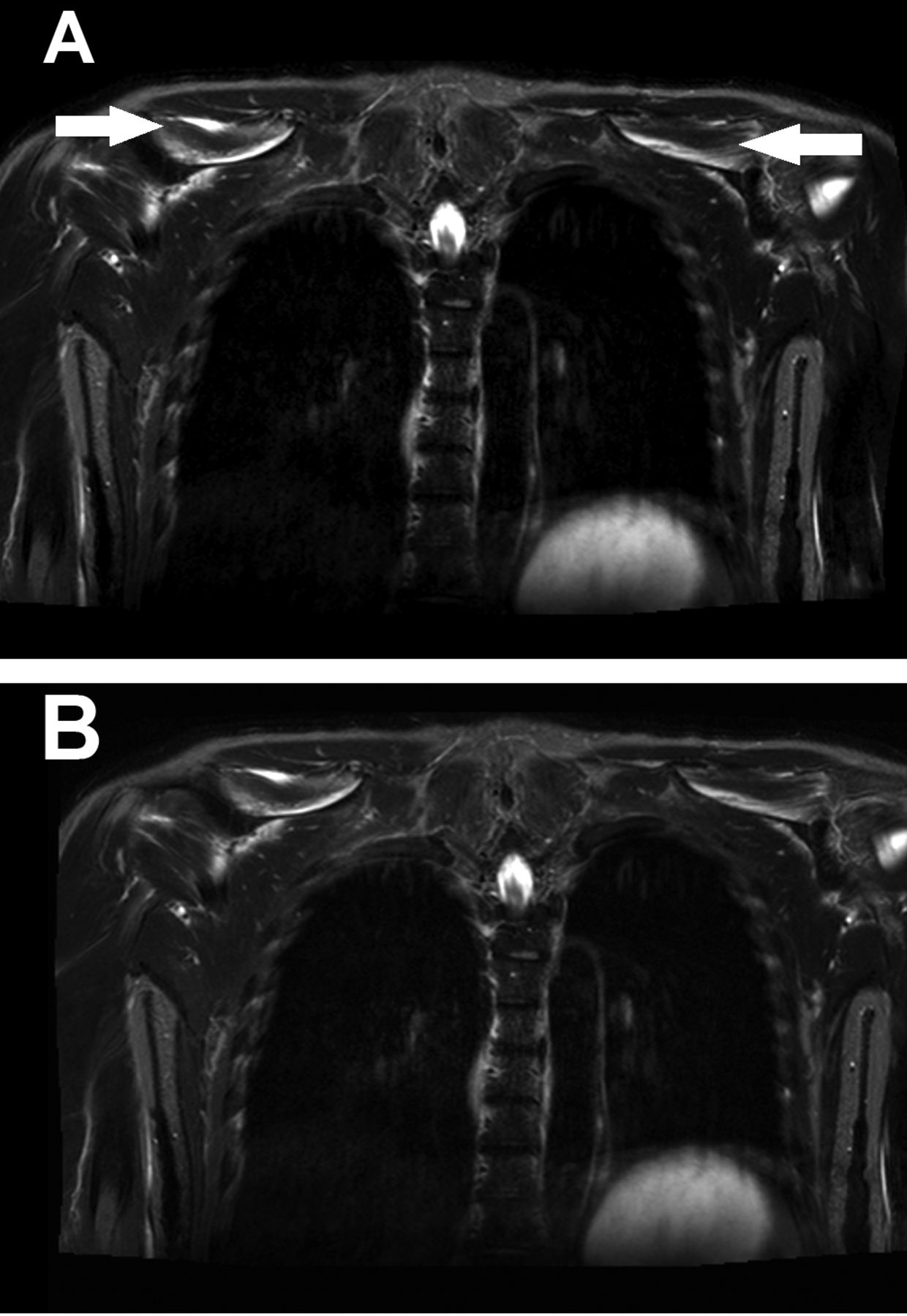
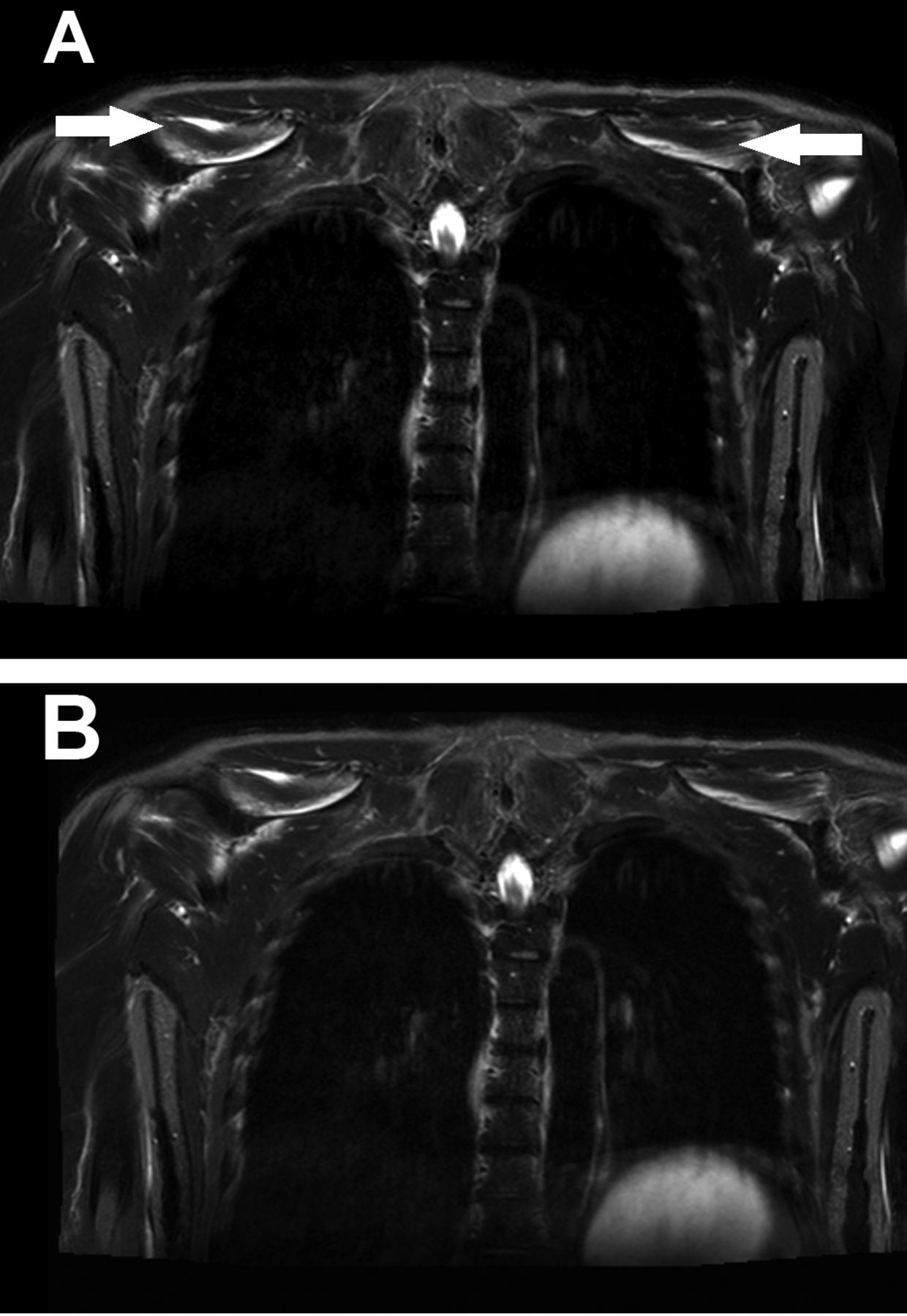
Coronal magnetic resonance imaging views showing the change in myofascial lesions from baseline (A, arrows) to 12 weeks after tocilizumab initiation (B).

Axial magnetic resonance imaging views showing the change in myofascial lesions from baseline (A, arrows) to 12 weeks after tocilizumab initiation (B).
Muscle groups showing myofascial lesions by magnetic resonance imaging at baseline (Week 0) and 12 weeks after tocilizumab therapy initiation.
Localized myofascial lesions seen by MRI
At baseline (Table 2, Figure 3), all patients had at least 1 localized inflammatory myofascial lesion. These lesions were seen at the shoulder in 10 (71.4%) patients, hip in 13 (86.7%), ischial tuberosity in 9 (60.0%), and pubic symphysis in 12 (80.0%). The total number of muscle groups with myofascial lesions at baseline was 70 of 103. Involvement was bilateral at the shoulders in 7 (50.0%) patients, hips in 13 (86.7%), and ischial tuberosities in 6 (40.0%). There was at least 1 shoulder girdle lesion in 10 (71.4%) patients and at least 1 pelvic girdle lesion in 13 (86.7%) patients.
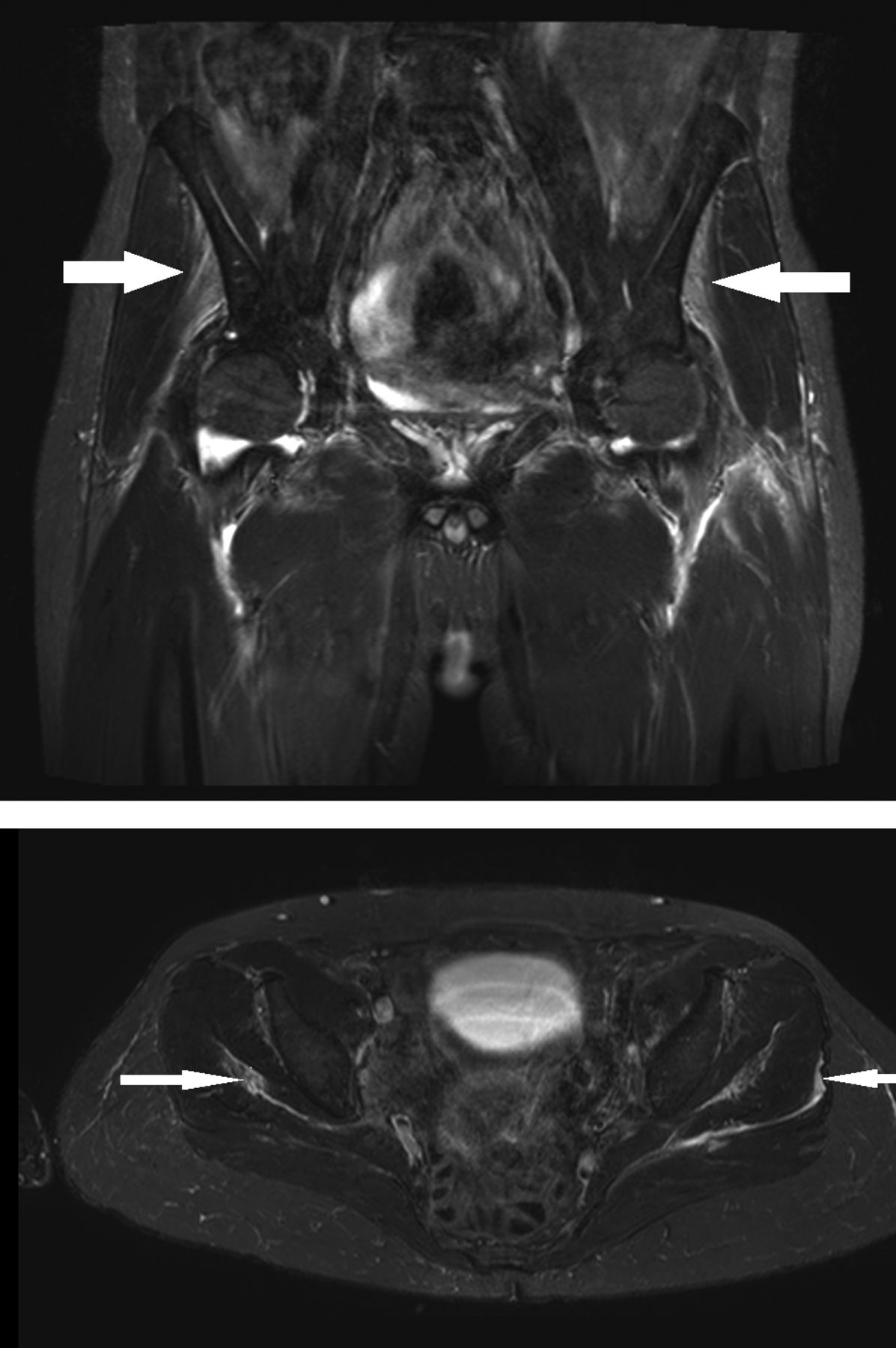
Magnetic resonance imaging of the gluteal muscles showing muscle inflammation (top, arrows) and fascial inflammation (bottom, arrows).
At 12 weeks (Table 2), 8 (53.3%) patients had shoulder lesions, 5 (33.3%) had hip lesions, and 3 (20.0%) had pubic symphysis lesions; none had ischial tuberosity lesions. There was at least 1 shoulder girdle lesion in 8 (53.3%) patients and at least 1 pelvic girdle lesion in 7 (46.7%) patients.
Changes with TCZ therapy
Of the 103 muscle groups studied in all, 70 had localized inflammatory myofascial lesions at baseline and 60 at 12 weeks (p = 0.002; Table 2). Over the 12-week period, the lesions improved in 66 (64.1%) muscle groups, worsened in 2 (1.9%), and remained unchanged in 35 (34.0%; p = 0.034; Table 3).
Changes in myofascial lesions visible by magnetic resonance imaging from baseline (Week 0) to 12 weeks after tocilizumab therapy initiation.
DISCUSSION
Localized myofascial lesions visible by MRI were common in patients with recent-onset PMR and improved during TCZ therapy. Intraobserver repeatability and interobserver reproducibility were good for detecting myofascial lesion and assessing their course over time.
In previous studies, MRI of the shoulder and pelvic girdles in patients with recent-onset PMR were reported to show periarticular inflammation described as extracapsular soft tissue edema14 or periarticular soft tissue edema15. Another study found that many patients had extracapsular inflammatory lesions around the shoulders and knees16. None of the study reports describe localized myofascial lesions. In our study, all patients had 1 or more localized inflammatory myofascial lesions at the shoulder and/or pelvic girdles at baseline. The lesions were usually bilateral. Nevertheless, myofascial inflammation appeared less frequently than bursitis and synovitis of the shoulder and pelvic girdles, which remain the hallmark of PMR. Thus, at baseline in the TENOR study, 93% and 100% of the patients had bursitis by MRI at the shoulders and hips, respectively, and 100% had synovitis at both sites10. In a study of ultrasound (US) and MRI abnormalities in recent-onset PMR meeting Healey’s criteria16, all patients had subacromial bursitis (bilateral in 96%)17 and trochanteric bursitis (bilateral in 90%)18.
The diagnosis of PMR is based on suggestive clinical findings and laboratory tests combined with the absence of other plausible diagnoses19,20. Criteria for PMR have been developed by Chuang, et al11, Healey16, and more recently by the ACR/EULAR, which developed a criteria set that includes US findings20. All these criteria sets have high sensitivity but limited specificity for PMR21. Conceivably, adding other investigations such as MRI might improve specificity. The main differential diagnosis is rheumatoid arthritis (RA), most notably in the variant presenting as a PMR-like disease in patients older than 60 years22. Other differential diagnoses include spondyloarthritis (SpA), crystal deposition disease, other inflammatory joint diseases, inflammatory myopathies, OA, endocrine disorders, and cancer22. In a prospective study of diagnoses in patients presenting with girdle pain and ESR elevation, no early clinical or laboratory features reliably distinguished between RA and PMR23.
Few studies have compared imaging findings between PMR and other diagnoses. Two studies by the same group compared US and MRI for detecting bursitis in cases with PMR and controls with girdle pain due to other diagnoses (RA, psoriatic arthritis, knee or hip OA, fibromyalgia, or connective tissue disease) and onset after 50 years of age18,19. In the groups with PMR, subacromial/subdeltoid and trochanteric bursitis was significantly more common and more often bilateral than in the control groups. There was no difference for glenohumeral or hip synovitis, tenosynovitis of the long head of the biceps, iliopsoas bursitis, or ischio-gluteal bursitis. A study with US found that subacromial/subdeltoid bursitis and tenosynovitis of the long head of the biceps were significantly more common in patients with PMR than those with RA presenting with bilateral shoulder pain, whereas glenohumeral synovitis was more common in the RA group24. With MRI, no difference between PMR and RA was found for synovitis, bursitis, or tenosynovitis; and extracapsular edema adjacent to the capsule or in the soft tissues in the PMR group was the only significant difference14. Thus, intracapsular inflammation may be comparable in the 2 diseases and extracapsular inflammation more common in PMR. A 2015 systematic review showed that the performance of imaging studies for diagnosing PMR cannot be quantified accurately based on the data available so far but suggested a supportive role for imaging when the diagnosis is in doubt25.
MRI muscle abnormalities have not been reported in recent-onset RA26 or SpA27. Their presence may therefore support a diagnosis of PMR. If such is the case, then adding MRI findings to diagnostic criteria sets might improve specificity. It would therefore be of interest to compare the frequency of localized inflammatory myofascial lesions in patients with PMR and in those with other diagnoses such as RA and SpA.
After 12 weeks of TCZ monotherapy, the MRI localized myofascial lesions were usually improved. Thus, 66 (64.1%) muscle groups showed less inflammation, including 43 (41.7%) with no inflammation at all. These findings are consistent with the improvements in clinical and laboratory features seen in the TENOR study: 85% of patients achieved very low disease activity (PMR-AS < 7) by Week 12, and CRP levels returned to normal5. It is also consistent with the significant decrease in maximal standardized uptake shown by 18F-fluorodeoxyglucose positron emission tomography/computed tomography28. The 64.1% proportion of improved muscle groups was higher than the corresponding 32% and 52% proportions of improved synovitis and bursitis, respectively, and worsening was noted for only 2% of the muscle groups compared to 10% and 5% for synovitis and bursitis, respectively10. Thus, the muscle may be the site that responds best to the therapeutic effect of TCZ. Improvements were most common (80%) at the hip and pubic symphysis muscle groups. Nevertheless, the MRI myofascial lesions remained unchanged in 34.0% of muscle groups, despite a clinical improvement. The proportion of sites with no change was 57% for synovitis and 43% for bursitis10. Thus, the MRI abnormalities seem to change more slowly than do the clinical manifestations, possibly because of the high sensitivity of MRI for inflammation. The proportion of improved sites would perhaps be higher if MRI were performed after a longer followup.
Interestingly, a recent publication by Fruth, et al29 evaluating 40 contrast-enhanced pelvic MRI of patients with PMR on a predefined scoring system also found an enhancement of the proximal rectus femoris origin in 100% and of the adductor muscles at the inferior medial pubic bone in 90% of cases.
The main limitations of our study are the small sample size and absence of controls. Given the absence of a placebo arm, whether the changes observed were induced by TCZ therapy or occurred spontaneously cannot be determined.
In addition to synovitis and bursitis, PMR causes localized myofascial inflammation of the shoulder and pelvic girdles. TCZ therapy improves the myofascial lesions, in addition to the clinical and laboratory features.
Acknowledgment
We thank the rheumatologists and general practitioners who referred their patients to the TENOR study. We are grateful to Marie Jezequel and Nathalie Bihannic (Clinical Investigations Center) for centralizing the material and to Audrey Le Goff-Coquet and Valentine Guiton (Clinical Research and Innovation Agency) for coordinating the TENOR study. We also thank the staff for their time and commitment to this work.
Footnotes
The TENOR study received an unconditional grant and the tocilizumab used for the study was donated by Roche-Chugai, which manufactures tocilizumab. Roche-Chugai had no role in the design or conduct of the TENOR study or the current study; data collection, analysis, or interpretation; or preparation, revision, or approval of the manuscript.
- Accepted for publication February 20, 2019.








{kind=link}
{kind=link}
{kind=link}