

Abstract
Objective. A variety of infectious agents, including varicella zoster virus (VZV), have been hypothesized to play a role in the pathogenesis of giant cell arteritis (GCA). The detectability of the virus in patients with GCA is debatable. To further investigate an association between GCA and VZV infection, 10 years of GCA cases were evaluated for VZV by immunohistochemistry (IHC).
Methods. All temporal artery biopsies and ascending aortic resections positive for GCA from 2007 to 2017 at Brigham and Women’s Hospital were immunostained using a VZV antibody cocktail (SG1-1, SG1-SG4, NCP-1, and IE-62).
Results. Forty-one temporal artery biopsies and 47 ascending aortic resections positive for GCA were identified, all of which were found to be negative for VZV by IHC. Twelve temporal artery biopsies in this cohort were previously analyzed by unbiased metagenomics sequencing and were negative for VZV DNA.
Conclusion. These results argue against a clinically relevant association between VZV infection and GCA, and support neither routine testing for VZV nor treatment with antiviral drugs.
Over the last several years, significant progress has been made in understanding the pathogenesis of giant cell arteritis (GCA). While much is known about activated dendritic cell–mediated recruitment of inflammatory cells and stimulation of intimal hyperplasia leading to symptomatic vascular occlusion, the initial activating event remains unclear1,2. Several bacterial and viral pathogens have been proposed as potential infectious triggers including Chlamydia pneumoniae, herpes simplex virus, varicella zoster virus (VZV), cytomegalovirus, parvovirus B19, and human para-influenza 13. VZV reactivation has received attention owing to the similarity of its demographics to those of GCA; herpes zoster predominates in older adults, and 90% of cases of GCA occur in individuals older than 60 years. Herpes zoster occurs because of reactivation of latent virus in ganglia, which has been attributed to waning immunity that can be partially negated by vaccination4. It has been hypothesized that reactivated VZV spreads transaxonally from ganglia to arterial adventitia, where an immune response could be stimulated.
Reactivation of VZV has been proposed as an infectious trigger of GCA5, and it has been recommended that antiviral therapy be included in the treatment of GCA6. However, while initial reports described widespread detection of VZV antigen in the majority of GCA cases, subsequent studies from other institutions found only minimal or nonspecific immunostaining in temporal artery biopsies7,8,9. To determine whether a clinically significant association is present between GCA and VZV in our own patient population, we examined temporal artery biopsies and aortic artery resections over a 10-year period for evidence of VZV.
MATERIALS AND METHODS
This study was conducted with institutional review board approval at the Brigham and Women’s Hospital, Boston, with waived patient consent for use of excess human material (Protocol #: 2017P000840; approved June 22, 2017). Cases of GCA diagnosed by temporal artery biopsy or ascending aortic resection were identified over a 10-year period (2007–2017) at the Brigham and Women’s Hospital along with representative age-matched controls. Immunohistochemistry (IHC) was performed on 5-micron sections using a VZV antibody cocktail (SG1-1, SG1-SG4, NCP-1, and IE-62; Cell Marque) at 1:100 dilution with a 10-min protease digestion and alkaline phosphatase (red chromogen) for detection. For aortic resections, a single block per case exhibiting the greatest number of giant cells was selected for IHC. Temporal artery biopsies consisted of 1 block per case, with the exception of a single case with 2 blocks; sections from all blocks were evaluated by IHC. Positive controls were contemporaneously stained in the same runs. All H&E, elastin, and IHC slides were reviewed by 2 study pathologists, one with subspecialty expertise in neuropathology and infectious disease pathology, and the other in cardiovascular pathology. Statistical significance was determined by the Student t test or chi-square test with p value < 0.05.
RESULTS
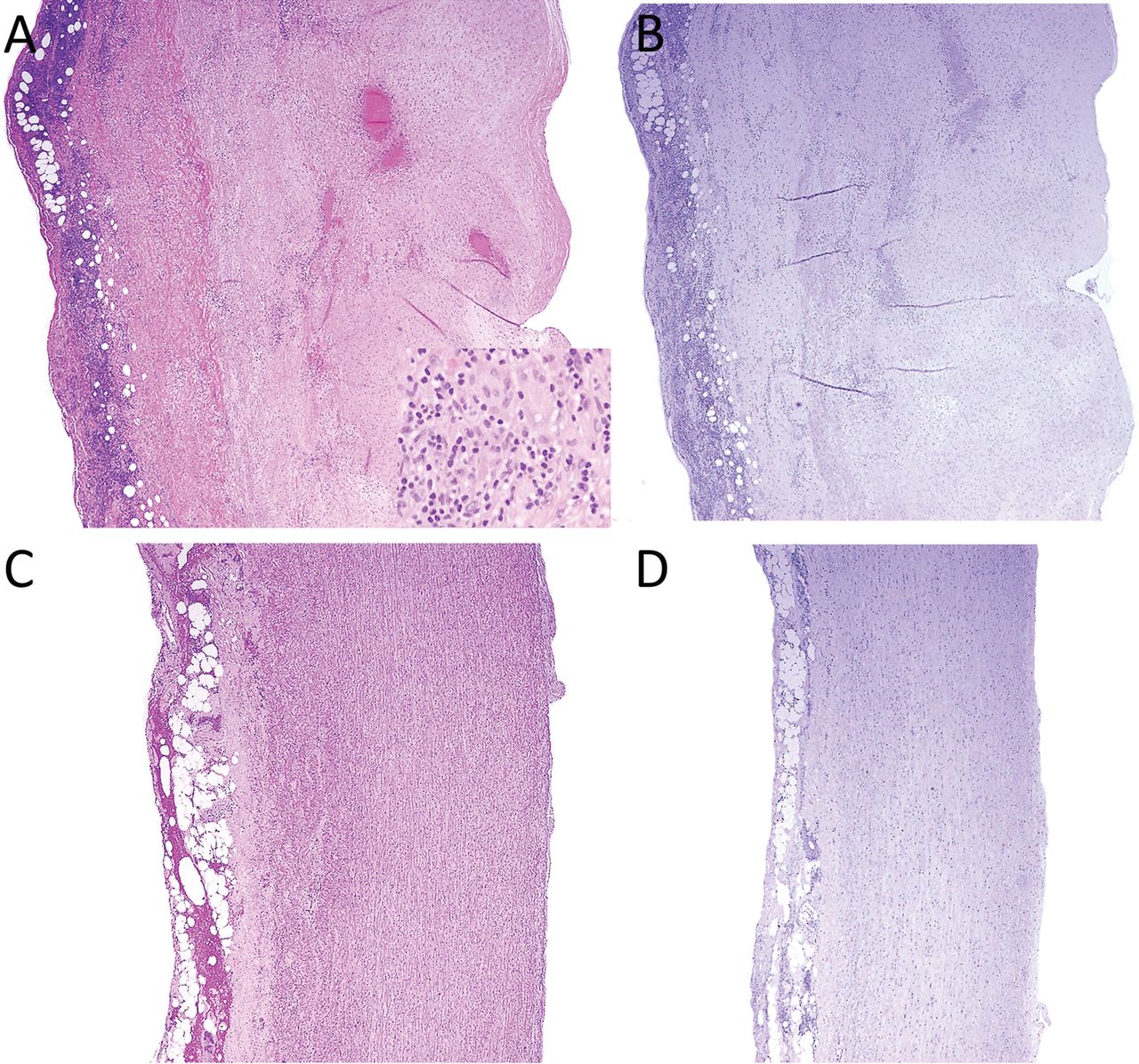
Over a 10-year period, 399 temporal artery biopsies were identified, including 41 diagnostic of GCA. Representative negative controls (n = 10) were matched for age and sex (Table 1). In all GCA-positive cases, a moderate to severe transmural lymphohistiocytic and giant cell infiltrate was observed, with resultant thickening of vessel walls; narrowing of the lumens was often present (Figure 1A). Control cases exhibited vessel walls with normal thickness, clearly demarcated intimal, medial, and adventitial layers with intact internal elastic lamina, and no medial inflammation (Figure 1C). No viral cytopathic effects were identified in any of the vascular layers, and VZV IHC was negative in all 41 GCA-positive cases and 10 negative controls (Figure 1B and 1D; Table 1).

No evidence of varicella zoster virus (VZV) in temporal artery biopsies. A. Biopsy of a temporal artery from a patient with giant cell arteritis shows transmural, non-necrotizing inflammation, stromal hyperplasia, and narrowing of the lumen. Occasional giant cells are present (inset). B. Immunohistochemistry for VZV (red) is negative. C. Biopsy of a temporal artery negative for giant cell arteritis shows no significant inflammation, thickening of vessel wall, and an intact lumen. D. Immunohistochemistry for VZV (red) is negative. Images taken with 10× (A–D) or 40× (panel A inset) objectives.
Search for VZV antigen in GCA-positive or -negative temporal artery biopsies.
Over the same 10-year period, 1255 ascending aortic resections were identified, including 47 with evidence of giant cell aortitis. All but 2 patients (45/47, 96%) underwent surgery for an uncomplicated aortic aneurysm; the remaining 2 were resected for aortic dissection. Representative controls from noninflammatory aneurysm resections (n = 10) were matched for age and sex (Table 2). Similar histologic findings were observed to those in the temporal artery biopsies, including the presence of moderate to severe transmural lymphohistiocytic and giant cell infiltrates with focal medial necrosis; the adventitia typically was fibrotic with chronic inflammatory infiltrates (Figure 2A). Control cases exhibited bland medial degeneration and elastin fragmentation changes, thinner vessel walls with intact layers, and no medial inflammation (Figure 2C). No viral cytopathic effects were identified, and VZV IHC was negative in all 47 GCA-positive cases and 10 negative controls (Figure 2B and 2D; Table 2).

No evidence of varicella zoster virus (VZV) in aortic artery resections. A. Sections of an aortic artery resection from a patient with giant cell arteritis (GCA) shows transmural, non-necrotizing inflammation and stromal hyperplasia. Occasional giant cells are present (inset). B. Immunohistochemistry for VZV (red) is negative. C. Resection from an aortic artery resection negative for GCA shows no significant inflammation or thickening of the vessel wall. D. Immunohistochemistry for VZV (red) is negative. Images taken with 4× (A–D) or 40× (panel A inset) objectives.
Search for of VZV antigen in GCA-positive or -negative ascending aortic resections.
Positive control cases, including VZV-infected skin and central nervous system VZV-vasculitis lesions, contemporaneously stained with the aortas and temporal arteries, were appropriately positive (Figure 3).

Positive varicella zoster virus (VZV) immunohistochemistry in controls. A. Biopsy of a vesicular skin lesion showed cells containing viral cytopathic effects (not pictured) associated with varicella zoster immunoreactivity (red). B. Biopsy of a middle cerebral artery lesion exhibited focal areas of VZV immunoreactivity (red) consistent with VZV vasculopathy. C. Biopsy of a skin lesion from a giant cell arteritis patient 3 months after initiation of high-dose corticosteroids shows squamous epithelium with marked viral cytopathic effects, including frequent nuclear inclusions and binucleated cells, with marked acute inflammation, consistent with the diagnosis of herpes zoster. D. Immunohistochemistry highlights extensive VZV (red). Images taken with 10× (A), 20× (B), or 40× (C–D) objectives.
A subset of the 41 temporal artery biopsies positive for GCA have previously been analyzed by an unbiased metagenomics assay to evaluate for evidence of potential infectious agents and have been reported elsewhere10. In the 12 cases examined, no DNA from VZV or any other pathogens with proposed links to GCA were identified.
DISCUSSION
Over a 10-year period, 41 temporal artery biopsies and 47 ascending aortic resections diagnostic of GCA were identified, all of which were negative for VZV by IHC. Falsely negative results can be excluded on the basis of the strong and specific IHC signal seen in our positive control cases, comprising lesions from VZV-infected skin and central nervous system VZV-vasculitis. These results contrast with findings described by Gilden and colleagues, who reported in a series of studies that the majority of GCA-positive temporal artery biopsies (70–74%) were positive for VZV by IHC, as well as a large number of GCA-negative temporal artery biopsies (58–64%) and normal controls (8–22%)5,11,12; they also found 11/11 (100%) GCA-positive aortas and 5/18 (28%) controls to be positive for VZV13.
A possible source of the discordance between these results is a difference in antibodies or IHC protocols. The present study used a mouse monoclonal cocktail targeting glycoprotein I, glycoprotein E, nucleocapsid protein, and IE-62 (SG1-1, SG1-SG4, NCP-1, and IE-62; Cell Marque) at 1:100 dilution with protease digestion. Gilden, et al primarily used a mouse monoclonal antibody raised against glycoprotein E (Santa Cruz) at 1:500 dilution on formalin-fixed paraffin-embedded (FFPE) tissue5. This antibody is in fact recommended for use in Western blots and for immunofluorescence on fresh frozen tissue, not for IHC of FFPE tissue14. Another possible explanation for the discrepant IHC results is differences in the number of levels examined by IHC. In the present study, 1 section per case was stained for VZV, versus 50 sections/case by Nagel, et al11. The likelihood of missing a single (1/50) positive level in 88 consecutive cases is low (16.9%), and there is a 0.009% chance of missing 5/50 positive levels. Differences in the number of levels examined are thus unlikely to account for the discordant results for VZV positivity of 0% in our study and 70–74% in the studies of Gilden, et al5,11,12,13.
There are issues with the interpretation of the IHC findings as presented by Gilden, et al5,11,12,13. Many of the reported areas of VZV positivity do not conform anatomically to the outline of cells, as would be expected from a true positive stain of an intracellular organism; rather, the areas of staining (Figure 1 panels A, B, C, E, M, O, and Q from Gilden, et al, 20155) are present in extracellular matrix, which is not inhabited by VZV during its life cycle. True staining for VZV is strongly positive within the nucleus and cytoplasm of infected cells, with little staining of the extracellular matrix (Figure 3). In addition, a variety of cases including 4 GCA-positive temporal artery biopsies and 5 negative controls were stained using a mouse monoclonal anti-glycoprotein I antibody (Millipore) that is recommended for IHC of FFPE tissue7,15. Staining was observed in cardiac muscle, skeletal muscle, and smooth muscle cells in the arterial media and adventitia, all interpreted by the authors of that study as false positivity for VZV. Similar findings were reported using rabbit antiserum against VZV IE-63, for which adventitial staining in macrophages was observed in GCA-positive and -negative cases with no correlation to detection of VZV DNA, also interpreted by the authors as likely false positivity due to cross-reactivity of the antibody with antigen on the adventitial histiocytes16.
The interpretation of histopathologic descriptions in the Gilden work is similarly problematic. VZV is an intracellular pathogen that produces characteristic viral cytopathic changes. None of the light microscopic images provided in the studies by Gilden, et al5,11,12,13 exhibits these changes, and in our own experience of reviewing about 1000 temporal artery biopsies, we have never observed viral cytopathic changes suggestive of VZV in either GCA or negative cases. Additionally, the histopathology of bona fide active VZV infection shows viral cytopathic changes, including epithelial multinucleated giant cells, necrosis, and an acute inflammatory reaction with abundant neutrophils, but the host reaction to VZV does not include macrophage-derived giant cells, as are common in GCA.
Gilden, et al also described electron microscopic (EM) findings interpreted as diagnostic of VZV infection5. VZV has characteristic ultrastructural features, including an icosahedral nucleocapsid surrounded by tegument and envelope, which are not evident in either of the study’s EM images. The image in Figure 2F (Gilden, et al5) does not show any specific cellular structure, and lacks any recognizable context that would assist in interpretation of the pathology. The image in Figure 2G5 shows a classic apoptotic cell with membrane blebbing, not viral egress from a cell as is claimed.
While IHC is a widely used and effective method for the diagnosis of VZV infections in skin and other tissue specimens, molecular assays have also been used. Molecular testing was not part of the current study, but prior analysis of a subset of 12 temporal arteries positive for GCA, using unbiased next-generation DNA sequencing, showed no evidence for VZV10. These results again contrast with the reported detection by Gilden, et al of VZV DNA in 18/61 (30%) temporal arteries and 7/11 (64%) aortas with GCA characterized as positive for VZV by immunostaining5,13.
Other investigators have also found it difficult to confirm an association between VZV and GCA. Regarding IHC, 2 groups tested the same mouse monoclonal anti-glycoprotein E antibody used by Gilden, et al for analysis of temporal artery specimens positive for GCA. Positive results were found in only 1/34 (3%) cases at 1:250 dilution in one study, and in 3/25 (12%) cases and negative in all controls at 1:500 dilution with microwave antigen retrieval in another study8,9. Using a variety of VZV targeted PCR assays, 4 independent studies were negative for viral DNA in a combined total of 109 cases8,17,18,19. In an effort to minimize formalin-fixation artifacts, frozen tissue has also been tested in a pair of recent reports, with no VZV DNA detected in 8 aortas or a combined total of 15 temporal artery biopsies from patients with GCA8,20. Earlier studies also reported mixed results, including detection of VZV IE-63 DNA in a minority of GCA cases (9/35, 26%) compared to 0/29 controls (unsupported by confirmatory EM or IHC16). In contrast, no difference in VZV DNA prevalence was detected in GCA-positive temporal artery biopsies (18/57, 32%) compared to negative controls (18/56, 32%)21.
We report negative VZV immunostaining in 41 temporal artery biopsies and 47 ascending aortic resections from individuals with GCA, findings consistent with the majority of previously published studies. Molecular evidence for VZV is similarly lacking. A clinically relevant association between GCA and VZV cannot be verified. Testing for VZV by IHC or molecular assays is not warranted, nor is treatment of GCA with antiviral agents.
Acknowledgment
This study would not have been possible without the assistance of the Brigham and Women’s Hospital Histology and Immunohistochemistry Laboratories.
- Accepted for publication December 5, 2018.








{kind=link}
{kind=link}
{kind=link}