

Abstract
Objective. We assessed construct validity of high-resolution peripheral quantitative computed tomography (HR-pQCT) joint space outcomes by comparison with radiographs in patients with rheumatoid arthritis.
Methods. In 43 patients, quantitative, volumetric, HR-pQCT measurements were compared with ordinal Sharp/van der Heijde scoring (SvdH) in the 2nd and 3rd metacarpophalangeal joints.
Results. Generalized estimating equations showed that joint space minimum, SD, and asymmetry by HR-pQCT were associated with SvdH scores (p < 0.05). There was a considerable range in HR-pQCT measurements at SvdH equal to 0.
Conclusion. HR-pQCT demonstrated construct validity outcomes and provides improved 3-D visualization of joint space.
- RHEUMATOID ARTHRITIS
- RADIOGRAPHIC MICRO-COMPUTED TOMOGRAPHY
- RADIOGRAPHY
- METACARPOPHALANGEAL JOINT
- OMERACT
Patients with rheumatoid arthritis (RA) develop joint damage as a result of an immune process involving synovium and periarticular bone, which manifests radiographically as joint space loss1,2. The importance of joint space narrowing on function has been demonstrated3. Conventional radiographs (CR) remain a feasible standard in clinical practice and research, but have known limitations in resolution, sensitivity, and responsiveness4. Radiograph scoring systems may be predisposed to floor and ceiling effects because significant progression is required for changes in ordinal scores, and scoring systems cannot demonstrate ongoing damage once the highest ordinal score has been achieved5,6,7.
State-of-the-art high-resolution peripheral quantitative computed tomography (HR-pQCT) is a sensitive tool used in the assessment of metacarpophalangeal (MCP) joints to describe joint space width (JSW), erosion number and size, as well as bone density and microarchitecture with high precision8,9,10,11. JSW outcomes are calculated volumetrically using an operator-independent algorithm12 and are minimally sensitive to positioning13. However, to date no comparisons have been made between HR-pQCT and radiography across the full range of joint damage scored on radiograph. To establish the construct validity of HR-pQCT–derived 3-D volumetric JSW outcomes, according to the OMERACT 2.0 filter14,15, a comparison with outcomes from CR is required. The purpose of our study was to compare HR-pQCT–derived outcomes of JSW with the radiographs evaluated using the joint space domain of the van der Heijde-modified total Sharp (SvdH) score system.
MATERIALS AND METHODS
Study design
Forty-three patients who met the 2010 American College of Rheumatology-European League Against Rheumatism Classification for RA16 were recruited for a larger study on the effects of biologic therapy on HR-pQCT outcomes. HR-pQCT scans were performed at the University of Calgary between 2014 and 2016 and CR were performed as standard of care and obtained from medical records. For this analysis, we paired an individual’s HR-pQCT scan and radiograph, conducted within 2 months of each other. Therapy was maintained for 3 months prior to HR-pQCT scans and did not change between radiography and HR-pQCT scans. All participants provided written informed consent prior to participation. Approval for all procedures was obtained by the Conjoint Health Research Ethics Board at the University of Calgary (REB 13-0743).
Conventional radiography
CR of the hands were scored using the SvdH score by a single experienced reader from Imaging Rheumatology International (Meersen, the Netherlands)17. Only the joint space domain from the second and third MCP of the dominant hand was used for this analysis, to match the joints scanned by HR-pQCT. Joint space narrowing was scored as 0 = normal, 1 = focal, 2 = generalized (> 50% of original joint space left), 3 = generalized (< 50% of the original joint space left or subluxation), and 4 = bony ankylosis or complete luxation.
HR-pQCT image acquisition
HR-pQCT scans of the second and third MCP joints of the participant’s dominant hand were acquired. The hand was secured in a custom positioning device (XtremeCTII, Scanco Medical) using an established protocol18. We obtained a reference radiograph in the coronal plane, and a reference line was placed at the distal cortical surface of the 2nd metacarpal head. Beginning 3 mm distal to the reference line, a total of 30.6 mm was acquired in three 10.2-mm sections or “stacks” with a nominal isotropic resolution of 60.7 µm using manufacturer standard settings (68 kVp, 1470 µA, 43 ms integration time).
HR-pQCT image processing and analysis
All image processing was conducted using Image Processing Language (Scanco Medical). The outer, periosteal surfaces of the 2nd and 3rd metacarpal and phalangeal bones were identified using an automated method9,19. To segment bone from soft tissue, a Gaussian filter (sigma = 0.5, support = 1) and fixed global threshold (12% of maximum greyscale value) were applied. Each scan was evaluated for motion in each stack using the manufacturer’s standard scoring system from 1–5. Scans that included a motion score of 4 or 5 were excluded.
Volumetric joint space was quantified using an algorithm developed by consensus from the Study grouP for eXtreme Computed Tomography in Rheumatoid Arthritis (SPECTRA)12. The 3-D JSW including mean (JSW.Mean, mm), maximum (JSW.Max, mm), minimum (JSW.Min, mm), SD (JSW.SD, mm), asymmetry [defined as JSW.Asymm = ratio of JSW.Max/JSW.Min, (1)] as well as volume (JSV, mm3) were calculated. Cuts through the sagittal and coronal planes (2-dimensional) were automatically generated for visualization. A rheumatologist with HR-pQCT expertise reviewed all joints and scored for degree of luxation (none, subluxation, luxation) and bone-on-bone contact (yes, no).
Statistical analyses
Data were visualized using strip charts to compare radiographic and HR-pQCT outcomes. Generalized estimating equations (GEE) were used to obtain an estimate of the ability of HR-pQCT outcomes to predict CR scoring, and account for the correlation between joints within a participant. All statistical analyses were performed using R (v3.3) and RStudio (v1.0.136).
RESULTS
Demographics
Five joints were excluded because of motion artifact in the HR-pQCT scans. One joint was excluded because of the inability of the algorithm to correctly define the joint space. The final dataset included 80 joints (40 2nd MCP and 40 3rd MCP) from 43 participants (34 female, 9 male). The participants had a mean age of 56 years (range 22–82 yrs, SD 13 yrs), and a mean disease duration of 12 years (range 0.5–39.1 yrs, SD 8.5 yrs). The mean time interval between radiograph and HR-pQCT acquisition was 1.5 weeks (range 0–9.1 weeks, SD 1.5 weeks).
JSW results
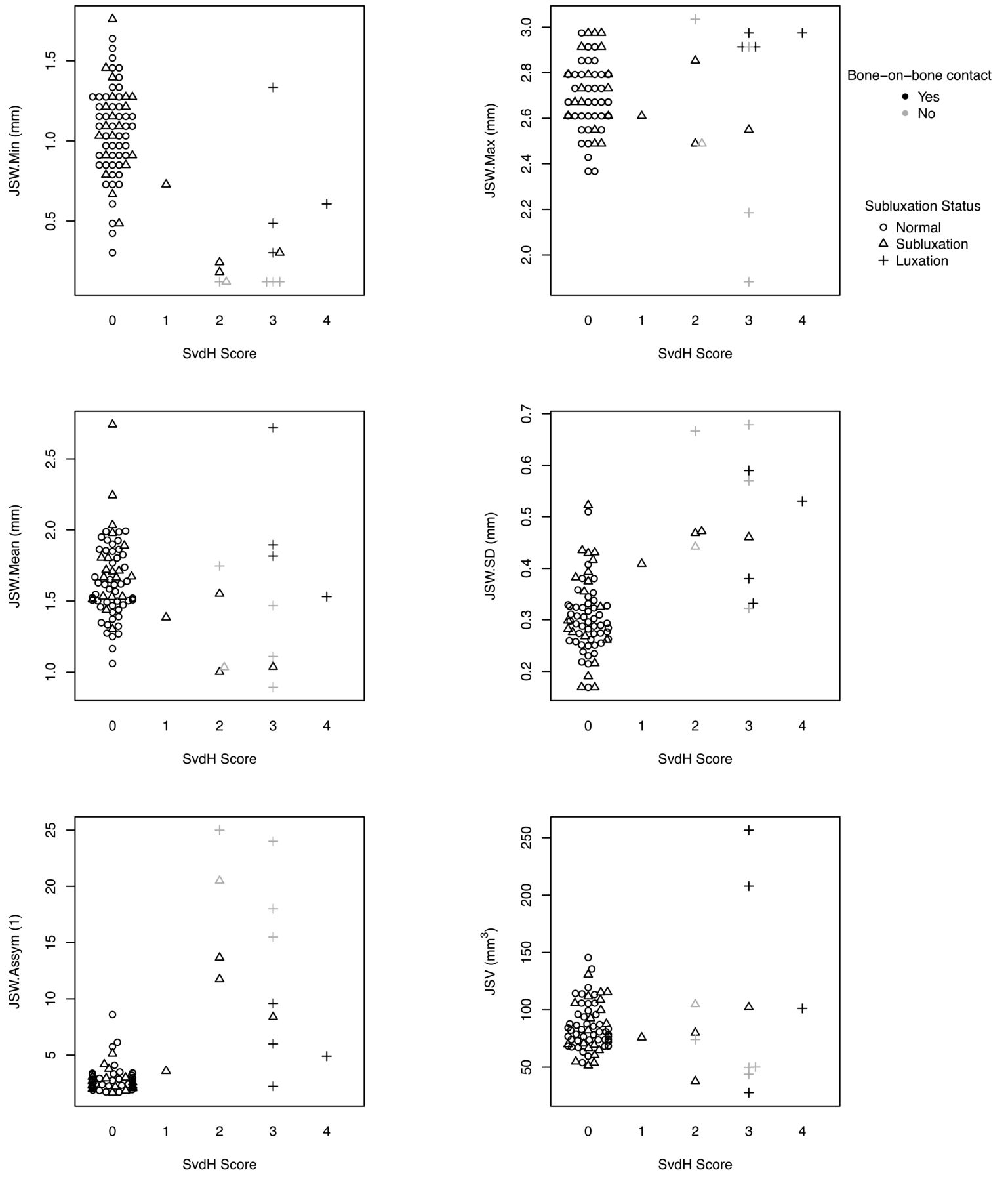
Distribution of SvdH scores for the 2nd and 3rd MCP is shown in Table 1. Figure 1 shows the distribution of HR-pQCT measurements by SvdH scores. More (sub)luxations were identified by HR-pQCT than radiograph. Bone-on-bone contact was observed in 5 joints on HR-pQCT, despite an absence of ankylosis observed on radiograph. GEE results indicated that decreased JSW.Min, increased JSW.SD, and increased JSW.Asymm were associated with increasing SvdH score (p < 0.05). However, no significant relationship was observed for JSW.Max, JSW.Mean, or JSV (p > 0.05). Visual examples of congruent and incongruent HR-pQCT and SvdH are shown in Figure 2.

Comparison between volumetric joint space outcomes derived from HR-pQCT with van der Heijde-modified Sharp joint space scores (SvdH) from conventional radiographs for the 2nd and 3rd MCP (n = 80 joints from 43 participants). MCP: metacarpophalangeal; JSW: joint space width; HR-pQCT: high-resolution peripheral quantitative computed tomography.
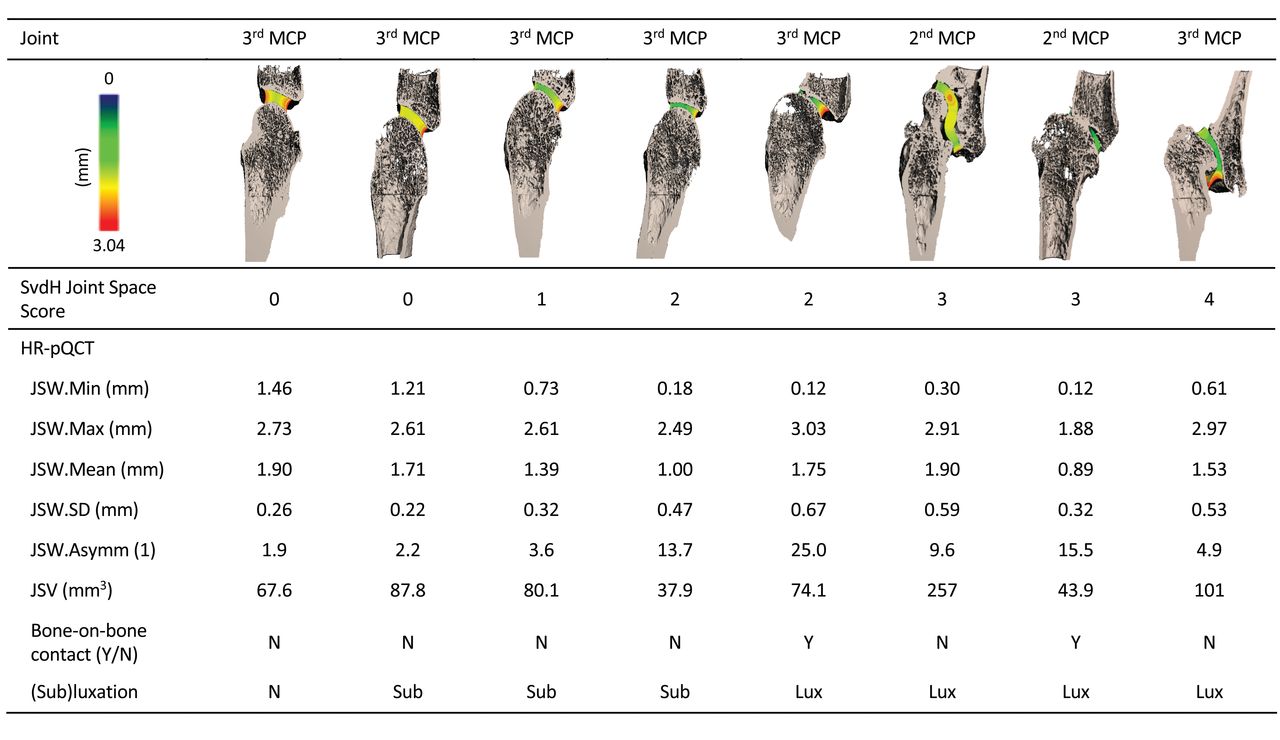
Examples of 3-D volumetric renderings of HR-pQCT scans and corresponding HR-pQCT outcomes across the range of van der Heijde-modified Sharp joint space scores (SvdH). HR-pQCT: high-resolution peripheral quantitative computed tomography; MCP: metacarpophalangeal; JSW: joint space width; JSV: joint space volume; sub: subluxation; lux: luxation.
Frequency of joint space narrowing scored using the van der Heijde-modified Sharp scoring system on conventional radiographs (n = 80 joints from 43 participants).
DISCUSSION
Minimum JSW, SD, and asymmetry assessed by HR-pQCT were correlated with the joint space domain of a radiograph scoring system. However, large variability for SvdH scores across all quantitative outcomes confirms that the radiographic score is indeed an ordinal scale, and consequently progression would not be linear. The considerable number of subluxations, luxations, and bone-on-bone contact observed with HR-pQCT, and in previous studies using the current gold standard clinical CT20, suggests there may be a degree of subluxation and ankylosis that precedes detection of this damage on radiograph. Finally, it is difficult to interpret disease progression based on a single quantitative HR-pQCT outcome, such as volume, because there is a nonlinear association with radiographic score. The relationship between these pathological manifestations and clinical and patient-reported outcomes needs to be further investigated to understand how they relate to disease outcome.
HR-pQCT may provide advantages over radiography for monitoring disease progression, particularly in the context of clinical trials. HR-pQCT quantitative measurements appear less susceptible to floor and ceiling effects because there is a wide range of measurements in JSW.Min and JSW.SD when the ordinal score is assigned 0, and there is no maximum limit to SD and asymmetry outcomes. The quantitative design of the analysis and sensitivity of the technique will allow observation of increases or decreases in joint space. Further, automated image processing makes HR-pQCT outcomes less susceptible to reader interpretation.
A key limitation of HR-pQCT might be that fewer joints are accessible than in radiography; however, focusing on the 2nd and 3rd MCP of the dominant hand somewhat overcomes that limitation because those are the most commonly affected joints in RA. Although this cohort consisted of participants with severe disease activity, the most common SvdH score was 0. This is likely reflective of the general RA population, in which there is a need for more sensitive measures relevant to earlier stages of joint damage. Further, interpretation of volumetric joint space outcomes in (sub)luxed joints is a challenge, and whether progression in these highly damaged joints can be observed, and follows a similar quantitative pattern to less damaged joints, needs to be determined in a longitudinal analysis. While our study used second-generation HR-pQCT, the results should be directly applicable to first-generation HR-pQCT, because the algorithm accounts for changes in spatial resolution and we have previously observed minimal difference between measurements of the same joints on both scanner generations. Finally, because the algorithm identifies thickness of the joint space, joints with bone-on-bone contact typically correspond to a minimum width of 1 or 2 voxels rather than 0. There are plans to identify this bone-on-bone contact in the future; however, because the discrepancy between the current algorithm and the absolute minimum is smaller than our reproducibility error, this small discrepancy does not affect the results.
We have demonstrated aspects of construct validity for HR-pQCT against a well-established radiographic scoring system. Because HR-pQCT provides 3-D visualization of the joint that is not available using CR, its utility for assessing disease prior to evidence of radiographic joint space damage and with levels of significant joint space damage is promising. Further longitudinal studies are planned to understand the sensitivity of HR-pQCT outcomes to change over a wide range of joint damage and repair.
Acknowledgment
We thank Tessa Linkert for assistance with patient recruitment and data collection, Shaheer Chishti for assistance with data analysis, and Dr. Tak Fung for assistance with statistical analysis.
Footnotes
The study was funded by The Arthritis Society. PGC is supported in part by the UK NIHR Leeds Biomedical Research Centre.
- Accepted for publication November 14, 2018.








{kind=link}
{kind=link}