

Abstract
Objective. To describe the longitudinal health status from childhood to adulthood in patients with juvenile idiopathic arthritis (JIA), compare outcomes after 19 years with those of controls, and identify early predictors of physical functioning, pain, and physical health-related quality of life (HRQOL).
Methods. Between 1995–2003, 96 patients with JIA (mean 6.1 ± 4.0 yrs, 67% female) were assessed within 18 months of diagnosis and every 6 months for the next 3 years with measures of JIA disease activity, physical functioning, pain, fatigue, and well-being. They were reassessed a mean of 18.9 ± 1.5 years later (mean age 25.1 ± 4.2 yrs) with measures of physical disability [Health Assessment Questionnaire–Disability Index (HAQ-DI)], pain, fatigue, well-being (visual analog scale), and physical and mental health-related quality of life (HRQOL; Medical Outcomes Study 12-item Short Form Health Survey, version 2).
Results. During the first 3 years, physical disability improved (p < 0.001) and the proportion of patients reporting best possible well-being increased (p = 0.013), while pain and fatigue did not change. At 3- and 19-year followups, patients had similar levels of physical disability, well-being, and pain, but fatigue increased (p = 0.016) and the number of patients with HAQ-DI = 0 decreased (p = 0.001). After 19 years, patients had worse pain and physical HRQOL than controls (p < 0.001). Pain, active joints, and physical disability during the first 3 years were associated with more disability and pain and worse physical HRQOL after 19 years (p < 0.001–0.047).
Conclusion. Patients with JIA reported similar physical functioning, well-being, and pain at 3- and 19-year followups, but more fatigue after 19 years. Patients also had worse health status than controls after 19 years. Pain, active joints, and physical disability were early predictors of unfavorable outcomes.
About 40–60% of patients with juvenile idiopathic arthritis (JIA) have continuous or recurrent disease activity extending into adulthood1,2,3,4. An important goal in the treatment of JIA is for patients to grow up to have the best possible quality of life. Health-related quality of life (HRQOL) is often measured through individuals’ subjective appraisals of their physical and psychosocial health, as defined by the World Health Organization5.
Physical disability, increased pain and reduced HRQOL have been reported in adults with a history of JIA2,4,6,7,8,9. However, the patients participating in these previous studies were diagnosed 1–2 decades before biologic agents were available and early methotrexate (MTX) was rarely used. New studies are needed because changes in treatment options since then may limit their present relevance10,11,12,13.
A few previous studies have examined the longterm longitudinal changes in health status among patients with JIA1,2,14,15. However, only 1 study included children early in their disease course, and these children were included in 1984–19862. Studies have indicated that early control of disease activity leads to better outcomes among children with JIA16,17. The identification of early predictors of longterm outcome into adulthood has been scarce, and only Bertilsson, et al used a prospective design during the early disease course2,3,18,19,20. Because different patterns of disease activity early in the disease course have been identified in children with JIA21, sequential assessments may increase the predictive ability of the assessed variables. Although longitudinal studies of the early disease course in children with JIA have been performed16,22,23,24, the effect of sequential assessment on longterm outcome has not been explored previously.
Pain is a commonly reported symptom of JIA12,25. To the best of our knowledge, no study has explored early predictors of pain in adults with a history of JIA. Further, pain intensity at a group level could be masking different pain trajectories within the group. Therefore, longitudinal studies of pain early in the disease course are needed to determine whether they are associated with health status in adulthood.
Given these gaps in the research literature, the objective of our study was to describe the longitudinal changes of health status in patients with JIA from childhood to adulthood, compare health status in adults with JIA to controls from the general population, and identify early predictors. The patients in this study were diagnosed from 1995 to 2000. Although biologic agents were not available at disease course, they became available during the first few years of their disease course. The patients were prospectively followed over 3 years early in the disease course and reassessed after 19 years to provide a greater understanding of the association between early disease course and health status in adulthood.
MATERIALS AND METHODS
Study population
Patients with JIA and < 18 months of disease duration were recruited from Oslo University Hospital from April 1995 to December 1999, examined by a pediatric rheumatologist and assessed by questionnaires every 6 months for the next 3 years, and reassessed 19 years later. The patients were classified according to the International League of Associations for Rheumatology guidelines based on physicians’ clinical examinations in the patients’ medical records26. Disease onset was defined as the day a physician documented symptoms or signs of JIA. Controls matched for age and sex were selected randomly from the National Registry. The patients resided throughout Norway (except the Northern region), whereas controls resided in Oslo and the surrounding county of Akershus, which contains both rural and urban areas.
The Regional Committees for Medical and Health Research Ethics approved the study (approval number 2015/532), and informed consent was obtained in accordance with the Declaration of Helsinki.
Data collection early in the disease course (1995–2003)
A rheumatologist examined all patients and information regarding medication was prospectively collected. Patients were assessed using the following indicators of JIA disease activity: physician’s global assessment (PGA) of disease activity (5-point Likert scale where 1 = best possible score), number of joints with active arthritis, number of joints with limited range of motion (LROM), and erythrocyte sedimentation rate (ESR). The Childhood Health Assessment Questionnaire (CHAQ) was used to assess physical disability27, and visual analog scales (VAS) were used to assess patients’ pain, fatigue, and overall well-being22,28,29. All VAS scales in our study were measured on a 10-cm scale where 0 = best and 10 = worst possible score. Pain intensity and well-being ratings were obtained from children ≥ 8 years of age and by proxy reports from parents for children < 8 years. Fatigue and physical disability (CHAQ) ratings were obtained from children ≥ 12 years of age and by proxy reports from parents for children < 12 years. Based on a previous study of adolescent with JIA, pain scores > 3 were defined as moderate to severe pain25.
Data collection at 19-year followup
At 19-year followup, demographic information (age, sex, marital status, occupational status, and highest level of education) was collected from patients and controls. Additionally, HRQOL was assessed with the Medical Outcomes Study 12-item Short Form Health Survey, version 2 (SF-12) including the physical component summary (PCS) and mental component summary (MCS)30. Pain severity and pain interference (effect of pain on daily functioning) were assessed with the Brief Pain Inventory (BPI) short form, fatigue with a VAS scale, and signs of anxiety and depression with the Hopkins Symptom Checklist 528,31,32. For JIA patients only, physical disability was assessed using the Health Assessment Questionnaire–Disability Index (HAQ-DI), supplemented with VAS ratings of pain intensity and overall well-being28,33. Information regarding current and previous use of medication and number of active joints was obtained using self-report questionnaires34. Questionnaires were delivered and returned by mail.
Statistical analysis
Comparisons between groups were performed using chi-square test of independence, independent sample t test and Wilcoxon–Mann-Whitney test. Independent sample analyses were selected to accommodate missing data without reducing sample size, but paired sample test was also conducted to confirm that the results were similar. Differences between repeated measures were analyzed with 1-way repeated measure ANOVA, Friedman’s test of variance, Cochran’s Q test, Wilcoxon signed-rank test, and McNemar’s test. Linear regression analyses were conducted to identify possible predictors of pain (VAS) and physical HRQOL (SF-12 PCS). Logistic regression analyses were used to assess predictors of physical disability (assessed by HAQ-DI). Independent variables associated with the dependent variable in the univariate analyses (p < 0.10) were evaluated in the multivariate analyses (manual backward regression method). BPI ratings of pain severity and pain interference were not included in the regression analyses because of multicollinearity between each other and with VAS pain (r > 0.7). Imputation of missing values on continuous variables at 1- and 3-year followups was performed by median substitution, with < 3% of the values being replaced.
Growth mixture modeling (GMM) was used to divide individuals into groups based on their trajectory of pain over time. The number of latent classes was decided based on the change in the likelihood function and the proportion of observations in each class. Individuals were assigned to classes based on posterior probabilities, and the discrimination among the classes was found to be clear. The analysis was carried out using the GLLAMM package in Stata. All other statistical analyses were performed using SPSS software Version 22 (IBM Corp.). A 2-tailed p value < 0.05 was considered statistically significant.
RESULTS
Demographic variables of patients and controls
Of the 197 patients who participated in the initial study from 1995 to 2003, at the 19-year followup, 4 had died, 1 had been re-diagnosed, 16 could not be located, and 80 patients chose not to participate (Appendix 1). A total of 96 (50%) of the 192 living patients with JIA agreed to participate in the 19-year followup and were compared with 96 controls. No significant differences were found between the patients who declined participation, could not be located, or had died, and the participants regarding age at disease onset, sex, polyarticular disease course, and scores on the CHAQ and VAS pain at 3-year followup (data not shown).
The sample was predominantly female (67%) with a mean (SD) age of 6.1 (± 4.0) years at disease onset and 25.1 (± 4.2) years at 19-year followup (Table 1). Educational achievement was similar between the patients and controls, although fewer adults with JIA were in full-time employment/study (p = 0.036) and more were receiving disability or social benefit allowance (p = 0.005).
Clinical characteristics of patients and health status and demographic characteristics of patients and controls at 19-year followup.
Health status in patients and controls at 19-year followup
No physical disability (HAQ-DI = 0) was found in 52 patients (54%) and severe disability (HAQ-DI ≥ 1.5) was found in 3 patients (3%; Table 2). Moderate to severe pain (VAS pain > 3) was reported by 26 patients (27%) and poor overall well-being (VAS well-being > 3) by 26 (27%). More pain and higher effect of pain on daily functioning (BPI pain severity and pain interference) were found in patients with JIA compared with controls (p ≤ 0.001) and a higher percentage of patients reported moderate to severe fatigue (VAS fatigue > 3) compared with controls (p = 0.001; Table 1). Poorer physical HRQOL was found on the SF-12 PCS score and the subscales: role physical, bodily pain, general health, and vitality (all p ≤ 0.001). HAQ-DI > 0 and VAS pain were the most important correlates of reduced physical HRQOL as measured by the SF-12 PCS (Table 3). No differences were found between patients and controls regarding mental HRQOL as measured by the SF-12 MCS.
Changes over time in variables assessed at baseline and at 1-, 3-, and 19-year followup (n = 96).
Relationship between demographic and health-related variables assessed at 19-year followup and physical HRQOL measured by the SF-12 PCS in 96 patients with JIA.
Disease-modifying antirheumatic drug (DMARD) use
Overall, 45 patients (47%) had received biological DMARD (bDMARD) and 67 (70%) had received MTX at some point during the followup period. In the first 3 years of followup, 7 patients (7%) were treated with bDMARD and 52 (54%) with MTX [including 4 (4%) prior to baseline and 20 (21%) since baseline]. At the 19-year followup, 52 patients (54%) were using DMARD (Table 1). Of the 44 (46%) not using DMARD, 6 (6%) had used bDMARD and 24 (25%) had used MTX within the last 10 years, but not at the 19-year followup. Comparisons of patients currently being treated with bDMARD (alone or in combination with synthetic DMARD; n = 37) and patients treated only with synthetic DMARD (n = 15) indicated no significant differences in physical disability [HAQ-DI median 0.19 (range 0–2.13) vs 0.13 (range 0–1.38), pain (VAS pain median 1.7, range 0–10 vs 1.1, range 0–8), and physical HRQOL (SF-12 PCS mean 46.9 ± 11.3 vs 51.5 ± 7.8)].
Changes in disease variables over time
During the first 3 years of followup, improvements were found in all disease activity variables (p < 0.001). The level of physical disability (CHAQ/HAQ-DI) improved during the first 3 years (p < 0.001), and the proportion of patients with no physical disability increased (p < 0.001; Table 2). Patients’ experience of pain and fatigue did not change during the first 3 years, but the proportion of patients reporting best possible well-being increased (p = 0.013). Levels of physical disability, pain, and well-being were similar at 3- and 19-year followups, but the level of fatigue worsened (p = 0.016) and the proportion of patients with no physical disability decreased (p = 0.001).
Early predictors of physical limitation, pain, and physical HRQOL after 19 years
Results from the univariate analyses showed that pain at baseline and both PGA and CHAQ ≥ 1 at 3 years were associated with physical limitations (HAQ-DI > 0) at the 19-year followup (p = 0.007–0.037; Table 4). Pain intensity after 19 years was associated with age and number of active joints, ESR, CHAQ ≥ 1, and VAS pain at baseline, and CHAQ ≥ 1 at 3 years (p < 0.001–0.02). Number of active joints, ESR, CHAQ ≥ 1, pain, and patient’s overall well-being at baseline, as well as PGA, presence of active joints, CHAQ ≥ 1, and fatigue at 3 years were associated with physical HRQOL at the 19-year followup (p < 0.001–0.044).
The relationships of health- and disease-related variables assessed at baseline and after 3 years to physical limitations (HAQ-DI > 0) after 19 years (n = 96)*.
In the multivariate analyses (adjusted for age and sex), physical limitations (HAQ-DI > 0) at 19-year followup were predicted by pain at baseline and physical disability (CHAQ ≥ 1) at 3 years (p = 0.013–0.041; Table 4). Pain intensity at 19-year followup was predicted by number of active joints and physical disability (CHAQ ≥ 1) at baseline and physical disability (CHAQ ≥ 1) at 3 years (p = 0.001–0.013). Physical HRQOL (measured by SF-12 PCS) at 19-year followup was predicted by number of active joints and pain at baseline and presence of active joints and physical disability at 3 years (p < 0.001–0.047).
Using GMM, 3 latent classes of pain within the first 3 years of disease duration were identified and named “recurrent pain” (n = 16; 17%), “late pain recovery” (n = 10; 10%), and “low pain” (n = 70; 73%; Figure 1). Late pain recovery during the early disease course was associated with physical disability (HAQ-DI ≥ 1), more pain, and poorer physical HRQOL after 19 years (p = 0.002–0.013; Table 5).
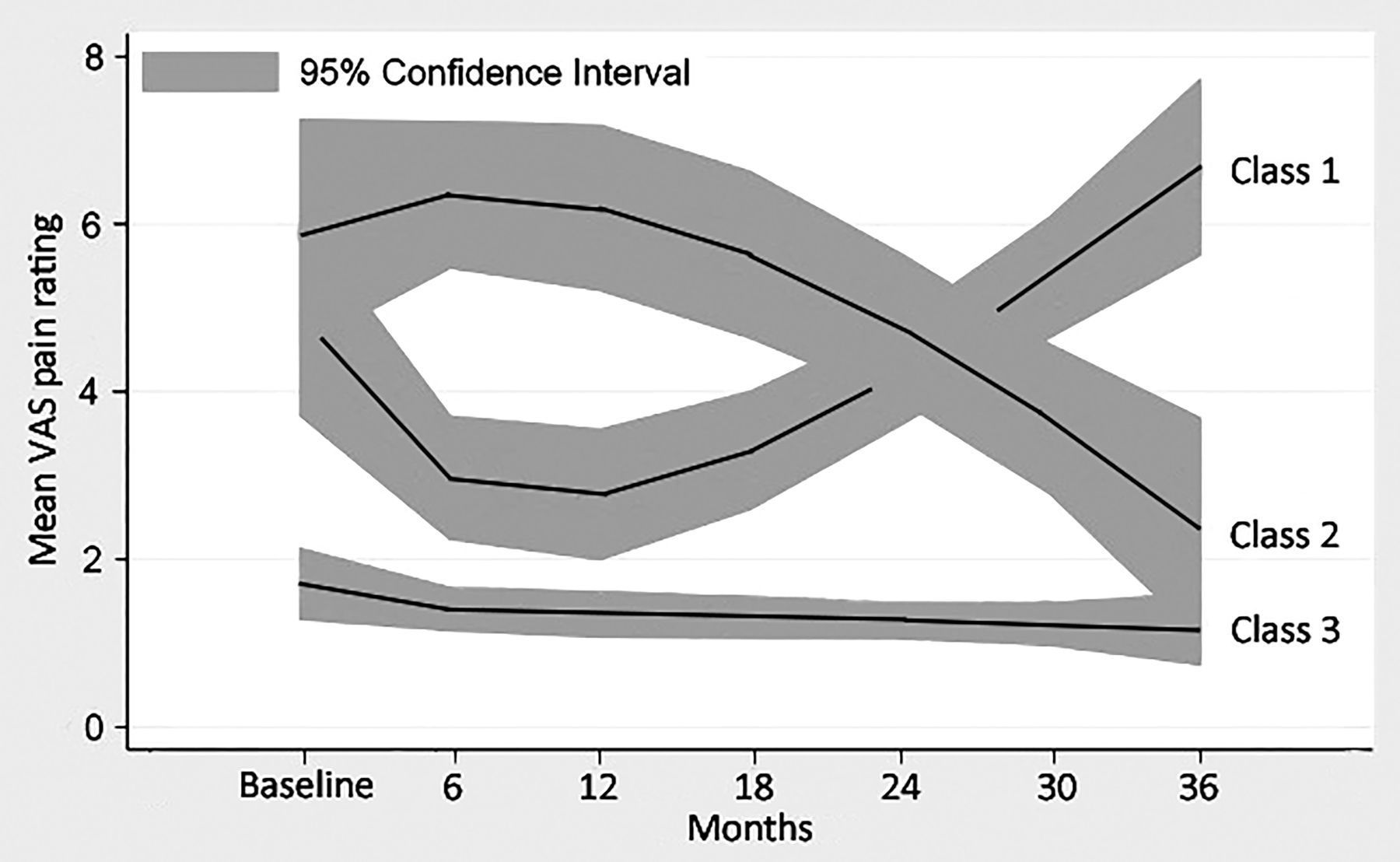
Trajectories of pain assessed every 6 months for 3 years at early disease course. Class 1 = recurrent pain, n = 16 (17%). Class 2 = late pain recovery, n = 10 (10%). Class 3 = low pain, n = 70 (73%). VAS: visual analog scale.
The relationships of health- and disease-related variables assessed at baseline and after 3 years to pain intensity (VAS pain) after 19 years (n = 96) #.
The relationships of health- and disease-related variables assessed at baseline and after 3 years to physical HRQOL (SF-12 PCS) after 19 years (n = 96) #.
Multiple regression models examining pain trajectory group membership early in the disease course as a predictor of physical disability, pain intensity, and physical HRQOL at 19-year followup (n = 96)*.
DISCUSSION
In our cohort of patients with JIA, the levels of physical disability (CHAQ/HAQ-DI), pain intensity, and overall well-being were similar at the 3- and 19-year followups, while fatigue worsened. After 19 years, patients had higher levels of pain severity and pain interference (measured by the BPI), poorer physical HRQOL (SF-12 PCS), and less work participation than controls from the general population. Pain intensity, active joints, and physical disability within the first 3 years of followup were early predictors of physical limitations, pain, and poorer physical HRQOL after 19 years. Further, late pain recovery during the first 3 years was associated with physical limitations, pain, and poorer HRQOL after 19 years.
Physical disability level, pain intensity, and overall well-being were similar, and fatigue was worse at the 19-year followup compared to the 3-year followup, despite improvements in JIA disease activity variables during the first 3 years of followup, as previously described22. Our results are in contrast to those of Zak, et al and Calabro, et al, who reported increased physical disability in their longitudinal followups of patients with JIA included in their studies in the 1960s and 1970s14,35. Different methods used to assess disability may have influenced the results. In particular, it should be noted that physical disability was assessed using the CHAQ in childhood and HAQ-DI in adulthood, and although they measure the same concepts and have the same structure, they are not equivalent to each other and comparisons should be made with caution. Nonetheless, our results regarding stable physical disability level and pain between the 3- and 19-year followup are in accordance with more recent longitudinal longterm studies of JIA2,15. However, in contrast to our present study, a decline in overall well-being between 15 and 30 years of disease duration was found in another Norwegian cohort6. We also found an increased level of fatigue between 3- and 19-year followups. This finding is consistent with the study by Nijhof, et al36 who reported more fatigue with increasing age among adolescents with JIA, but it contradicts the study by Ostlie, et al, who found a stable level of fatigue between 9- and 18-year followups15. Fatigue is a multidimensional concept with various causes, for which potential mediators in young adults with JIA need to be explored further.
No physical disability (HAQ-DI = 0) was found in 54% and severe disability (HAQ-DI ≥ 1.5) in 3% of patients after 19 years. This frequency of HAQ-DI = 0 is in line with several previous studies of adults with JIA2,6,14,37,38. Low frequencies of severe disability (HAQ-DI ≥ 1.5) have also been reported in other more recent studies of longterm outcomes in JIA. Tollisen, et al6 reported HAQ-DI ≥ 1.5 in 3% after 30 years in 2017 and Bertilsson, et al2 reported no patients with HAQ-DI > 1.5 after 17 years in 2013. On the other hand, Minden, et al reported HAQ-DI ≥ 1 in 7% after 17 years in 2002, and Ruperto, et al reported HAQ-DI > 1.5 in 4% after 15 years in 199739,40. Measured by the Steinbrocker method, severe disability was present in 3% in a study published in 2002, and 15–17% in cohorts described around 199035,38,41. Our results support that there has been a decline in the frequency of severe disability in adults with JIA during the last 2 decades.
A total of 27% of patients reported moderate to severe pain (VAS > 3) after 19 years and the patients in our study had higher scores on pain severity and effect of pain on daily functioning (assessed by BPI) than age- and sex-matched controls. Our study tends to confirm that pain is an important dimension of the burden of the disease in patients with JIA, which is also supported by other publications11,12,42.
Adult patients with JIA had poorer physical HRQOL than controls, while mental health status and academic achievement were similar; these findings are consistent with those of other studies2,6,7,8,19. We found less work participation in our patients compared to controls. Occupational outcomes in adults with a history of JIA have varied in previous studies6,7,38,39,43,44,45, and differences in the social insurance system and level of disease severity among the study populations may influence these differences.
Physical disability (CHAQ ≥ 1) at baseline predicted more pain at 19-year followup, and CHAQ ≥ 1 at 3 years predicted physical limitations, lower physical HRQOL, and more pain at 19 years. Number of active joints at baseline predicted more pain and lower physical HRQOL, while presence of active joints at 3 years predicted lower physical HRQOL at 19 years. Bertilsson, et al found no significant baseline predictors of physical disability after 17 years2. However, similar to our study, they found an association between CHAQ at 5 years and physical limitations at 17 years, as well as associations between number of joints with arthritis and CHAQ at 5-year followup and physical HRQOL at 17 years2. Identification of early prognostic factors of longterm outcomes in JIA has been difficult20, and the value of physical disability and active joints early in the disease course for predictions of later health status warrants further study.
Pain intensity at baseline predicted physical limitations (HAQ-DI > 0) and lower physical HRQOL at 19-year followup. During the first 3 years of followup, 3 different pain trajectories were identified within this patient group. We found associations between late pain recovery early in the disease course and physical disability, pain, and physical HRQOL at the 19-year followup. It should however be taken into account that the group of patients demonstrating late pain recovery is small (n = 10) and further studies with larger samples are required. The longterm effect of pain in JIA has not been well studied, despite pain being considered a main symptom of JIA12,25,46. The pathogenesis of pain in children with JIA is multifactorial and not fully understood, hence regular pain assessment and treatment should be promoted in clinical practice47,48.
This study has some limitations. No assessments were done between the 3- and 19-year followups and no clinical examinations were performed at the 19-year followup; therefore, results should be interpreted with caution. Moreover, we do not have information regarding remission status among the participating patients, although 54% of the patients were currently being treated with synthetic and/or bDMARD at 19-year followup. Also, 59% of the patients reported active joints (self-reported pain or swelling in combination with LROM), but this result should also be interpreted with caution. Dijkstra, et al reported a patient tendency to overestimate the presence of active joints, although patient indication of absence of arthritis proved to be highly reliable34. It should also be noted that patients in our cohort were diagnosed in the prebiologic era, since biologic treatments were introduced to patients with JIA in 2000. Although only 7 patients used bDMARD during the first 3 years, 67% of our patients received bDMARD at some time during the 19-year followup period.
The patients in our cohort are referral-based, hence there was an increased probability for participants with more severe disease compared to population-based cohorts. However, the patients were comparable to patients with JIA in a number of epidemiological studies regarding sex, age at onset, and distribution of diagnostic subgroups2,8,49,50. Additionally, at baseline no significant differences were found between the participants and nonparticipants regarding age, sex, and disease subtype. The healthcare system in Norway is largely tax-funded with equal access to specialist care for all patients with JIA, which also increases the probability of a patient being included regardless of disease activity level.
This study, with its longitudinal and prospective design, adds valuable information to the scarce data on longterm patient-reported outcomes of patients treated with synthetic and/or biological DMARD early in the disease course. Similar levels of physical disability, pain, and well-being were found at 3- and 19-year followup, but patients reported more fatigue and a lower percentage reported no physical disability after 19 years. JIA has a detrimental effect on physical disability, pain, and physical HRQOL 19 years after disease onset. The early predictors in our study were pain, physical disability (CHAQ ≥ 1), and active joints at baseline and/or at 3 years. Late pain recovery early in the disease course was associated with poorer health status after 19 years. However, further studies are required to explore early predictors of patient-reported outcomes in adults with JIA.
Acknowledgment
We thank Leiv Sandvik and Magne Thoresen (Institute of Basic Medical Science, Faculty of Medicine, Oslo University, Oslo, Norway) for statistical support; Thorhild Garen, Trude Ingebrigtsen (Department of Rheumatology, Oslo University Hospital), and Gunn-Helen Malmstrøm (Unger-Vetlesens Institutt, Lovisenberg Diaconal Hospital) for technical assistance; Caryl Gay (University of California/Lovisenberg Diaconal Hospital) for useful comments on the manuscript; and Joachim Sagen (Children and Youth Rheumatology Association) for useful comments on the questionnaires.
APPENDIX 1.

Participant flow chart.
Footnotes
This project was supported by the Norwegian Foundation for Health and Rehabilitation.
- Accepted for publication February 13, 2019.








{kind=link}
{kind=link}