

Abstract
Objective. To determine the predictors of remission and low disease activity state (LDAS) in patients with systemic lupus erythematosus (SLE).
Methods. Three disease activity states were defined: Remission = SLE Disease Activity Index (SLEDAI) = 0 and prednisone ≤ 5 mg/day and/or immunosuppressants (maintenance dose); LDAS = SLEDAI ≤ 4, prednisone ≤ 7.5 mg/day and/or immunosuppressants (maintenance dose); and non-optimally controlled state = SLEDAI > 4 and/or prednisone > 7.5 mg/day and/or immunosuppressants (induction dose). Antimalarials were allowed in all groups. Patients with at least 2 SLEDAI reported and not optimally controlled at entry were included in these analyses. Outcomes were remission and LDAS. Multivariable Cox regression models (stepwise selection procedure) were performed for remission and for LDAS.
Results. Of 1480 patients, 902 were non-optimally controlled at entry; among them, 196 patients achieved remission (21.7%) and 314 achieved LDAS (34.8%). Variables predictive of a higher probability of remission were the absence of mucocutaneous manifestations (HR 1.571, 95% CI 1.064–2.320), absence of renal involvement (HR 1.487, 95% CI 1.067–2.073), and absence of hematologic involvement (HR 1.354, 95% CI 1.005–1.825); the use of immunosuppressive drugs before the baseline visit (HR 1.468, 95% CI 1.025–2.105); and a lower SLEDAI score at entry (HR 1.028, 95% CI 1.006–1.051 per 1-unit decrease). These variables were predictive of LDAS: older age at entry, per 5-year increase (HR 1.050, 95% CI 1.004–1.098); absence of mucocutaneous manifestations (HR 1.401, 95% CI 1.016–1.930) and renal involvement (HR 1.344, 95% CI 1.049–1.721); and lower SLEDAI score at entry (HR 1.025, 95% CI 1.009–1.042).
Conclusion. Absence of mucocutaneous, renal, and hematologic involvement, use of immunosuppressive drugs, and lower disease activity early in the course of the disease were predictive of remission in patients with SLE; older age was predictive of LDAS.
A treat-to-target strategy has been proposed in systemic lupus erythematosus (SLE)1,2, but the proper target remains to be elucidated. Remission, especially without therapy, is uncommon; for example, in the GLADEL (Grupo Latino Americano De Estudio de Lupus) study cohort, only 3.7% of patients achieved remission at least once in the interval between 2 visits during their followup; per protocol, visits were performed every 6 months3. In the Toronto cohort, 1.7% of patients achieved remission for at least 5 years and 10.2% for at least 1 year4; and in the LCTC registry (Lupus Clinical Trials Consortium), 5.4% of patients achieved remission for at least 1 year5. In predominantly white cohorts, the incidence of remission is higher; for example, in an Italian study, 7.1% of the patients achieved remission for at least 5 years6, whereas 12.8% did so in a cohort from the Netherlands7.
An alternative outcome, remission with therapy, is still rare: 16.5% of patients in the GLADEL cohort achieved this at least once in the intervals between 2 visits during followup3, whereas 18.9% of the Toronto cohort4 and 7.6% of the LCTC cohort5 achieved this outcome for at least 1 year.
A less stringent target, low disease activity state (LDAS), was achieved in 14.2% of patients from the GLADEL cohort at least once in the intervals between visits during followup3 and in 14.9% of those from the LCTC5; additionally, for those in remission, 85% of the patients in the Asia-Pacific Lupus Collaboration (APLC) achieved LDAS at least once8, whereas 76.0% of patients in the Netherlands cohort did so7.
Because either remission or LDAS seem to be protective from new damage3,6,7,8,9,10,11, mortality10, and the occurrence of flares10, achieving these states seems quite important in the management of patients with SLE. However, how long these states should last and how frequently they need to be assessed remains to be elucidated. The Definitions of Remission in SLE (DORIS) group has suggested that duration should be examined at 6 and 12 months from disease onset and then at 2 and 5 years12.
We evaluated the factors associated with achieving remission or LDAS in patients with SLE from the GLADEL cohort who were not optimally controlled.
MATERIALS AND METHODS
Patients
The GLADEL cohort is an observational inception cohort study started in 1997 in 34 centers from 9 Latin American countries. A common protocol, consensus definitions, and outcome measures were established. General characteristics and composition of the GLADEL cohort patients have been described13,14. However, because this cohort was started in 1997, when signed informed consent for observational research studies was not required at all participating centers, we do not have such documentation for each patient; similarly, in 1997 most participating GLADEL centers did not have formal ethics committees. Nevertheless, the study was performed in accord with the Declaration of Helsinki protocol for research in humans and following local institutional review board regulations.
For these analyses, 3 disease activity states were defined as follows:
Remission: SLE Disease Activity Index15 (SLEDAI) = 0 and a prednisone dose ≤ 5 mg/day and/or use of immunosuppressive drugs (maintenance dose)
LDAS: not on remission and SLEDAI ≤ 4, prednisone dose ≤ 7.5 mg/day and/or use of immunosuppressive drugs (maintenance dose)
Non-optimally controlled state: SLEDAI > 4 and/or prednisone dose > 7.5 mg/day and/or use of immunosuppressive drugs (induction dose)3.
Antimalarials were allowed in all groups. These 3 states were evaluated using the interval between 2 SLEDAI measurements or the last SLEDAI and the end of the followup. Only patients who were non-optimally controlled at the time of the first SLEDAI measurement and who had at least 1 subsequent SLEDAI measurement were included in the analyses.
Variables
Demographic characteristics including sex, age at diagnosis, ethnicity, socioeconomic status (SES)16, level of education, urban/rural residence, and health insurance were evaluated.
Characteristics such as disease duration at entry to the study cohort and organs or systems affected at or before entry were included. Clinical manifestations were grouped into 11 domains, as follows: general manifestations (fever, weight loss and lymphadenopathies); muscle manifestations such as myalgia and myositis; articular manifestations such as arthralgia, arthritis, Jaccoud’s arthropathy, overall musculoskeletal related to SLE, and osteonecrosis; cutaneous manifestations such as alopecia, photosensitivity, malar rash, discoid rash, mucosal ulcers, panniculitis, livedo reticularis, subacute cutaneous lupus, bullous lupus, Raynaud phenomenon, and overall cutaneous related to SLE; ocular manifestations such as xerophthalmia, keratoconjunctivitis sicca, scleritis, episcleritis, uveitis, retinopathy, cytoid bodies, amaurosis, and overall ophthalmic related to SLE and cataracts; respiratory manifestations (lung serositis, interstitial lung disease, alveolar hemorrhage, pulmonary thromboembolism, pulmonary hypertension, shrinking lung, lung infarction, and overall respiratory related to SLE); cardiovascular manifestations (pericarditis, myocarditis, endocarditis, rhythm disorders, hypertension, ischemic heart disease, coronary artery disease, atherosclerosis, thrombosis, peripheral artery disease, and overall cardiovascular related to SLE); renal manifestations (proteinuria, cellular casts, glomerulonephritis, tubular interstitial alterations, renovascular disease, acute or chronic renal failure, and overall renal related to SLE); neuropsychiatric manifestations such as psychosis, seizures, neurologic syncope, vertigo, mood disorders, cognitive dysfunction, acute confusional state, dementia, motor/sensitive disorders, movement disorders, myelopathy, mononeuritis multiplex, polyneuropathy, cranial neuropathy, autonomic neuropathy, lupus headache, and overall neurologic related to SLE; digestive manifestations (peritoneal serositis, xerostomy, and overall digestive related to SLE); and hematologic manifestations (autoimmune hemolytic anemia, leukopenia, lymphopenia, thrombocytopenia, and overall hematologic related to SLE).
Disease activity was ascertained using the SLEDAI15 and was assessed, per protocol, twice a year.
Disease damage was measured using the Systemic Lupus International Collaborating Clinics/American College of Rheumatology Damage Index17 per protocol once a year.
Glucocorticoid use was recorded as the highest dose at or before entry to the study cohort and was categorized as low dose: prednisone ≤ 7.5 mg/day; medium dose: > 7.5 to ≤ 15 mg/day; high dose: > 15 to < 60 mg/day; or very high dose: ≥ 60 mg/day. Parenteral glucocorticoids were not included. Use of antimalarials and immunosuppressive drugs was recorded as ever used or not used. Treatment was recorded at or before entry to the study.
Statistical analyses
Patients with and without remission and LDAS during followup were compared using frequencies and percentages for categorical variables and medians and 25th–75th percentiles for continuous variables. Cox regression models were used to derive p values comparing the incidence of these outcomes for each baseline characteristic. For each outcome, a multivariable Cox regression model was derived using a backward selection method with α-level to stay in the model set at 0.05. Antimalarials use was included as a time-dependent covariate. All variables included in the descriptive analysis were considered candidates for inclusion in the multivariable model, except education level and immunological involvement, which were excluded because of missing values. Two alternative models were performed, one excluding serology and the second excluding manifestations that are probably not related to disease activity, including the variables grouped per organ/system or individually, for those manifestations present in at least 20% of the patients. Continuous variables were tested for linearity and linear splines were used in case of nonlinearity. The proportional hazard assumption was tested using the Schoenfeld residuals. Statistical analyses were performed using SAS v9.4 (SAS Institute).
RESULTS
At entry, 902 patients were non-optimally controlled (Supplementary Figure 1, available with the online version of this article); 809 (89.7%) were female, with a median age at diagnosis of 26 (20–36) years. The median length of followup was 56.3 (35.6–7.16) months. Characteristics of patients are given in Table 1.
Characteristics of patients with systemic lupus erythematosus (SLE) in this study.
One hundred ninety-six patients (21.7%) achieved remission; of them, 97 were followed for at least 3 years after achieving remission and 47 (48.5%) of them achieved prolonged remission. There were 314 (34.8%) who achieved LDAS; of them, 164 were followed for at least 3 years after achieving LDAS; 92 (56.1%) out of 164 experienced prolonged LDAS. The characteristics among those who achieved remission or not are given in Table 2, and for those who achieved LDAS or not in Table 3. Briefly, those who achieved remission more frequently had a higher SES and were better educated; they also had a lower frequency of mucocutaneous and renal involvement and a lower SLEDAI at baseline. Patients who achieved LDAS were older at diagnosis and at baseline; had a higher SES; were more educated; had lower frequency of general, mucocutaneous, and renal involvement; had used higher doses of prednisone; and had a lower SLEDAI at baseline.
Variables associated with remission by univariable analyses.
Variables associated with low disease activity state (LDAS) by univariable analyses.
In multivariable analyses, these were predictors of patients achieving remission: the absence of mucocutaneous manifestations (HR 1.571, 95% CI 1.064–2.320), of renal involvement (HR 1.487, 95% CI 1.067–2.073), and of hematologic involvement (HR 1.354, 95% CI 1.005–1.825); the use of immunosuppressive drugs before baseline (HR 1.468, 95% CI 1.025–2.105); and a lower SLEDAI at entry (HR 1.028, 95% CI 1.006–1.051 per 1-unit decrease). These were also predictive of patients achieving LDAS: older age at entry, per 5-year increase (HR 1.050, 95% CI 1.004–1.098); absence of mucocutaneous manifestations (HR 1.401, 95% CI 1.016–1.930) and renal involvement (HR 1.344, 95% CI 1.049–1.721); and a lower SLEDAI at entry (HR 1.025 (95% CI 1.009–1.042). The final multivariable models are depicted in Tables 4 and 5. Kaplan-Meier curves representing these multivariable analyses are shown in Figure 1 and Supplementary Figure 2, available with the online version of this article.
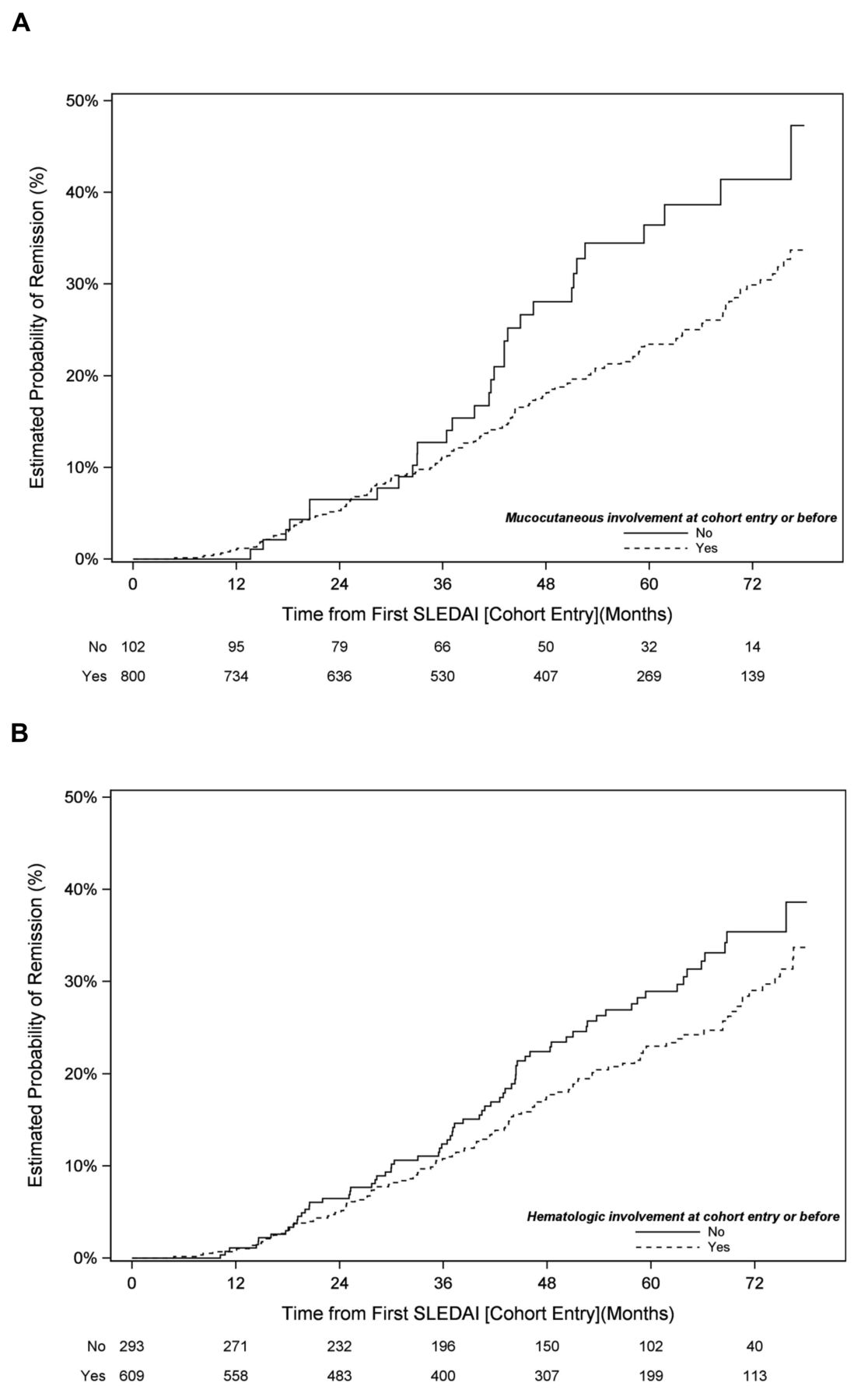
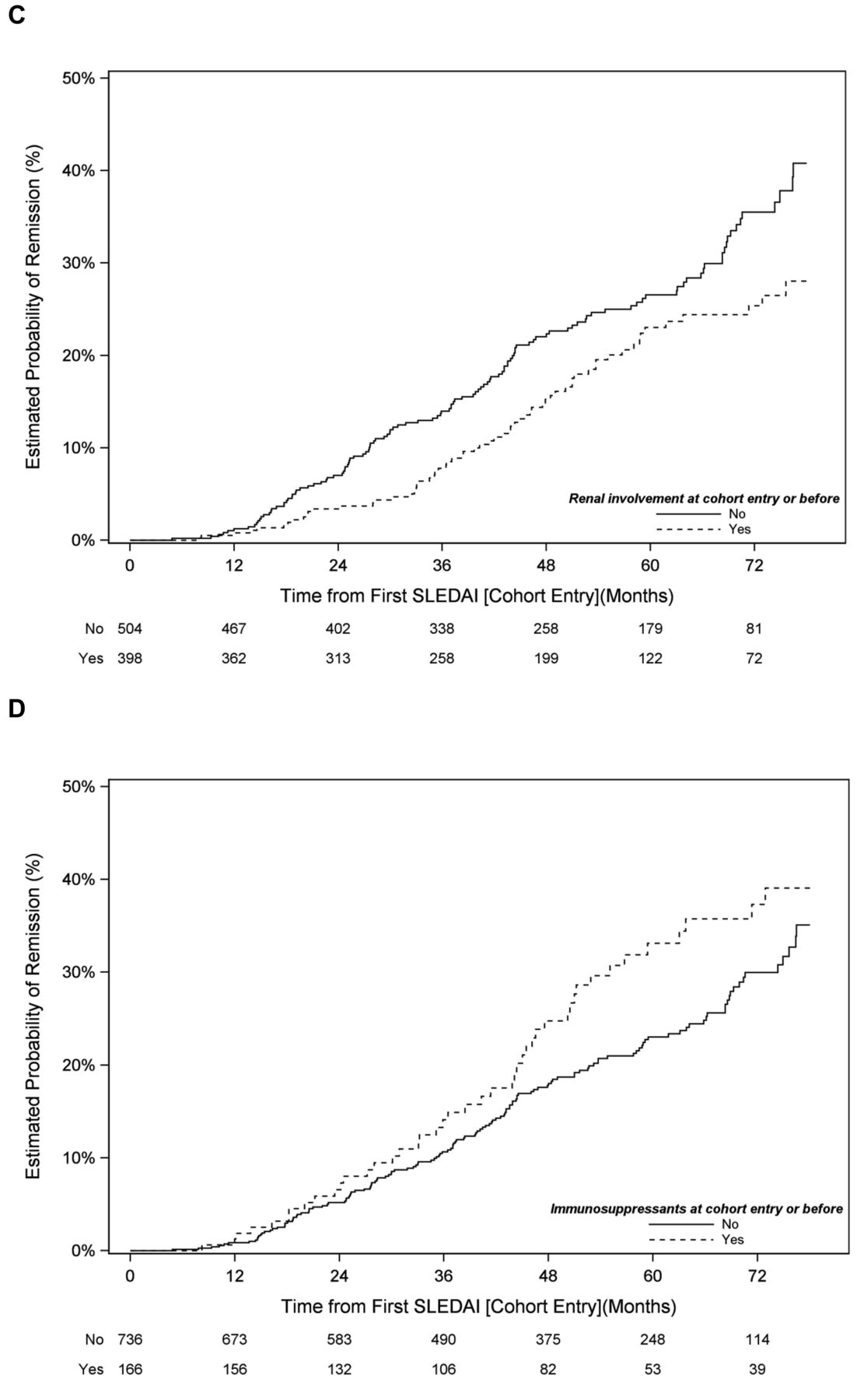
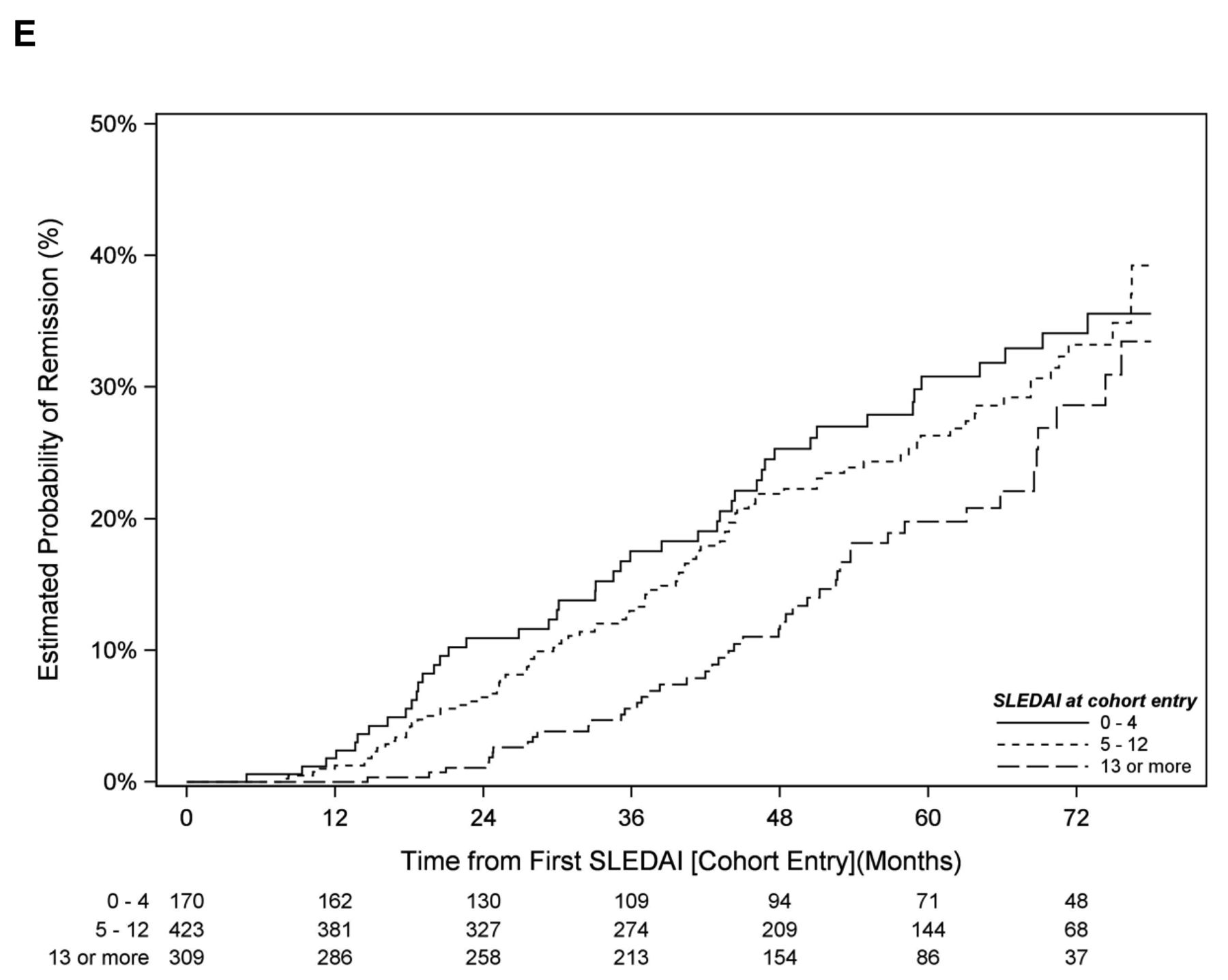
Predictors of remission in the GLADEL cohort. A. Presence of mucocutaneous involvement. B. Presence of hematologic involvement. C. Presence of renal involvement. D. Use of immunosuppressive drugs. E. SLEDAI at baseline (categorized). SLEDAI: Systemic Lupus Erythematosus Disease Activity Index.
Predictors of remission; multivariable model.
Predictors of low disease activity state; multivariable model.
Using alternative models, when we excluded serology, the results were very similar to those that included serology; and when we included independently those manifestations presented in at least 20% of the patients, the predictors of remission were the absence of fever, photosensitivity, cellular casts, and hematologic involvement as well as the use of immunosuppressive drugs and a lower SLEDAI (data not shown).
DISCUSSION
Using longitudinal data from GLADEL, a multiethnic, multinational inception cohort, we evaluated the predictors of achieving remission or LDAS/remission in patients with SLE. Of note, the absence of mucocutaneous manifestations and renal involvement, and lower disease activity early in the course of SLE were associated with a higher probability of patients achieving remission and LDAS. A higher SES was associated with an increased probability of remission, and a medium prednisone dose was associated with a higher probability of LDAS.
Although there is no uniformity among the factors associated with achieving remission and LDAS, some variables have been found in more than 1 study. For example, as in the current study, older age has been reported to be associated with remission or LDAS in studies from the UK18, China19, and the Netherlands7. Ethnicity was found to be associated with remission in the Toronto Cohort; those who achieved prolonged remission (> 5 yrs) were more frequently white9; this was also the case in the UK cohort18. Being white was also associated with LDAS in the Netherlands cohort, where whites more frequently achieved LDAS for at least 50% of the followup time7. Conversely, in the Hopkins Lupus Cohort, African Americans had a lower probability of achieving remission20. We found no such association in our cohort. However, the association between ethnicity and a lower probability of achieving remission or LDAS may relate to factors associated with ethnicity (health disparities, lower SES) and not necessarily to ethnicity per se.
As in our findings, the absence of mucocutaneous involvement was found to be associated with a higher probability of remission in some studies, but not in all. A higher probability was found in the Toronto cohort9 and the UK study18, but not in the Padua6, Netherlands7, Hopkins20, or a Chinese19 SLE cohort; absence of mucocutaneous involvement was also associated with a higher probability of achieving LDAS in the APLC cohort21. On the other hand, absence of renal involvement has been associated with a higher probability of achieving remission in several cohorts (Padua6, UK18, Netherlands7, and China19), but not in the Toronto9 or the Hopkins20 cohorts. Absence of renal involvement was also associated with a higher probability of achieving LDAS in the APLC cohort21 but not in the Netherlands cohort7. Similarly, absence of hematologic involvement was reported in the Hopkins20, Padua6, and China19 cohorts. Absence of other disease manifestations associated with a higher probability of remission, although not in our cohort, have been central nervous system involvement in the Toronto9 and UK18 cohorts, pulmonary involvement in the Toronto cohort9, cardiopulmonary in the UK18, vasculitis in the Padua cohort6, and immunological involvement in the Hopkins cohort20.
A lower SLEDAI score at baseline was associated with a higher probability of remission or LDAS/remission in our cohort; in a similar way, a lower SLEDAI at baseline and at followup was associated with prolonged remission in the Toronto9 and Netherlands7 cohorts. In the Netherlands cohort, a lower SLEDAI-2K at baseline was found in those patients who achieved prolonged remission and in those who achieved LDAS for at least 50% of the followup7. These findings contrast with those of a Spanish cohort, in which disease activity at baseline was found to be similar among those patients who achieved and those who did not achieve remission; however, that cohort included only 100 patients and its results should be viewed cautiously22.
Regarding treatment, a lower dose of glucocorticoids at baseline or during the followup was associated with prolonged remission in the Toronto9 and the Netherlands7 cohorts. In the Netherlands cohort, a lower use of immunosuppressive drugs was found in those patients who achieved LDAS for at least 50% of the followup7. Given that we examined the use of drugs before the baseline visit and very early in the disease course, our results cannot be compared. Rather, our data support the early but judicious use of immunosuppressive drugs if optimal outcomes are to be achieved in patients with SLE. Of note, these drugs can also increase the risk of damage accrual23.
Our study has some limitations. First, the relatively small number of patients who achieved remission while not receiving therapy precluded examination of the factors predictive of this state. Second, because of the relatively short followup and its variable duration, the effects of some predictors could have been underestimated. Third, because there are no uniform definitions of remission and LDAS, it is possible that had we used different definitions, our results could also have been different; however, similar definitions have been used in other studies, and they are considered reliable4,5,6,22. We must point out that manifestations that are either frequent (mucocutaneous), or that do not respond rapidly to treatment (renal), could lead to a delay in achieving remission; because our analyses were based on the examination of intervals rather than area under the curve, this is an important issue to consider.
Despite these limitations, our data from a very large multiethnic, multinational Latin American SLE cohort emphasize the advantage of not having mucocutaneous, renal, or hematologic involvement, of early use of immunosuppressive drugs, and of experiencing lower disease activity early in the course of the disease on a higher likelihood of achieving remission or LDAS. Our data also show the benefit of age on achieving LDAS. These data have practical applicability to treatment of patients with SLE.
ONLINE SUPPLEMENT
Supplementary material accompanies the online version of this article.
Acknowledgment
We are grateful to Daniel Villalba and Leonardo Grasso for assistance with the ARTHROS software. The GLADEL group acknowledges PANLAR (Pan American League of Associations for Rheumatology) for its support of the SLE study group.
- Accepted for publication December 18, 2018.








{kind=link}
{kind=link}
{kind=link}