

Abstract
Objective. To assess the occurrence and extent of interstitial lung disease (ILD) in patients with juvenile mixed connective tissue disease (JMCTD), compare pulmonary function in patients and matched controls, study associations between ILD and disease-related variables, and examine progression of pulmonary manifestations over time.
Methods. A cohort of 52 patients with JMCTD were examined in a cross-sectional study after a mean 16.2 (SD 10.3) years of disease duration with high-resolution computed tomography (HRCT) and pulmonary function tests (PFT) comprising spirometry, DLCO, and total lung capacity (TLC). Matched controls were examined with PFT. Previous HRCT and PFT were available in 37 and 38 patients (mean 8.8 and 10.3 yrs before study inclusion), respectively.
Results. Compared to controls, patients with JMCTD had lower forced vital capacity (FVC), DLCO, and TLC (p < 0.01). The most frequent abnormal PFT was DLCO in 67% of patients versus 17% of controls (p < 0.001). Fourteen patients (27%) had ILD on HRCT. Most had ILD in < 10% of their lungs. ILD was associated with low values for FVC and TLC, but not with DLCO. HRCT findings did not progress significantly over time, but FVC declined (p < 0.01).
Conclusion. Compared to controls, patients with JMCTD had impaired pulmonary function. ILD was present in 27% of patients after a mean 16 years of disease duration, mostly as mild disease, and did not progress. ILD seems to be less common in juvenile-onset than in adult-onset MCTD, and ILD in JMCTD seems mostly mild and stable over time.
- MIXED CONNECTIVE TISSUE DISEASE
- INTERSTITIAL LUNG DISEASE
- PULMONARY FIBROSIS
- PEDIATRIC RHEUMATOLOGY
- AUTOANTIBODIES
- OUTCOME RESEARCH
Mixed connective tissue disease (MCTD) is a rare autoimmune disease characterized by serum autoantibodies directed against RNP (anti-RNP), and with clinical findings that include Raynaud phenomenon and puffy hands, as well as features of systemic sclerosis (SSc), systemic lupus erythematosus (SLE), and/or polymyositis.
According to the diagnostic criteria for MCTD described by Kasukawa and colleagues, pulmonary manifestations comprise pulmonary fibrosis, restrictive lung disease (vital capacity < 80% of predicted), and/or reduced DLCO < 70% of predicted1. In adult MCTD, the prevalence of pulmonary manifestations, particularly interstitial lung disease (ILD), has been found to range from 35% to 78%, and to represent a major cause of morbidity and mortality2,3,4,5,6,7. The prognosis in MCTD seems to vary from mild disease, as initially described by Sharp, et al8, to a disease with severe complications, such as pulmonary fibrosis and pulmonary arterial hypertension4,9.
Disease onset during childhood or adolescence (< 18 yrs of age) has been reported to occur in 7–23% of all MCTD cases10,11. Data on lung involvement in juvenile (J-) MCTD are scarce. Aaløkken, et al12 found evidence of ILD in 25% of 24 patients with JMCTD, mostly as very mild disease. Further, Mier, et al13 described ILD in 3 of 10 patients in a subpopulation believed to be at risk. The prevalence and extent of ILD observed in JMCTD was lower than that reported in most studies on adult MCTD2,3,4,5,6,7. Progression of lung disease in adult-onset MCTD has been shown to be modest3,6. Nevertheless, studies focusing on the longterm outcome of pulmonary manifestations in patients with JMCTD are lacking.
Small retrospective studies on JMCTD have described reduced DLCO in 15−42% of patients and restrictive lung disease in 24−64%13,14,15. However, no research team has compared pulmonary function with controls from a general population. Whether there is a relationship between pulmonary function, ILD, and other disease-related variables in JMCTD is not known.
Herein, we aimed to do the following: (1) examine and assess the occurrence and extent of ILD in JMCTD in a representative nationwide cohort; (2) compare pulmonary function in patients with JMCTD with age- and sex-matched controls from a general population; (3) examine ILD progression and changes in pulmonary function over time; and (4) evaluate possible associations between pulmonary findings and disease-related variables.
MATERIALS AND METHODS
Patients and controls
The current cross-sectional study was performed at Oslo University Hospital (OUH) from March 2013 to June 2015.
Inclusion criteria were the fulfillment of the criteria for the diagnosis of MCTD set by Kasukawa and colleagues1 or Alarcón-Segovia and Villareal16, symptom onset < 18 years of age, and a clinical diagnosis of MCTD confirmed by a rheumatologist or pediatrician. Patients were identified through multiple acquisition routes and a nationwide approach; identification and inclusion have been described in detail previously17. Sixty-two patients were initially identified; of these patients 3 had died, 3 did not wish to participate, 1 did not respond to our enquiries, and 3 had developed clinical SLE and were excluded. Thus, 52 patients with JMCTD comprised our study population. Controls matched for age and sex were selected randomly from the Norwegian population register. Controls with a history of autoimmune disease necessitating immunosuppressive medication, heart disease, and/or lung disease (other than mild asthma) were excluded. Informed consent was obtained from all participants and from the parents of patients and controls < 16 years old, according to the Declaration of Helsinki. The study protocol was approved by the Regional Ethics Committee for Medical Research (2012/1721).
Clinical data
Patients and controls underwent a thorough clinical examination undertaken by the main investigators (SOH or VL). Clinical variables during the entire disease course and upon examination were obtained from medical records and patient interviews. Through examination of medical records and available data from a former study done by our research team12, previous high-resolution computed tomography (HRCT) images (Time 1) were available in 37 patients from at least 2 years before the cross-sectional examination (Time 2), and previous pulmonary function tests (PFT) were available in 38 patients. The mean time span between the first and second HRCT was 8.3 years (SD 2.7), and 10.3 years (SD 1.0) for the PFT. Smoking habits and level of physical activity were obtained from questionnaires.
Acquisition and analyses of CT images
HRCT was undertaken in patients only and obtained in the supine position during deep inspiration and breath-hold. Images were reconstructed in sections of thickness measuring 1–1.25 mm with 10-mm intervals, and at sections of thickness measuring 2.5 mm reformatted in the axial, coronal, and sagittal planes. The images were reviewed by 2 experienced chest radiologists blinded to clinical information on a picture archiving and communication system (PACS). The presence, extent, and distribution of ILD were evaluated according to the CT criteria of ILD recommended by the Nomenclature Committee of the Fleischner Society18. These criteria comprised reticular pattern (i.e., the coarseness of fibrosis), ground-glass opacities, traction bronchiectasis, interlobular septal thickening, and airspace consolidations. The reticular pattern was classified into 3 grades: 1 (fine intralobular fibrosis without evident cysts); 2 (mostly microcystic reticular pattern involving air spaces ≤ 4 mm in diameter); and 3 (a predominantly macrocystic reticular pattern with air spaces > 4 mm in diameter). HRCT findings were reviewed in 4 zones divided in a craniocaudal manner by the aortic arch, carina, and inferior pulmonary veins. The extent of fibrosis was expressed as a percentage of the total lung volume (TLV). Area measurements were done precisely by drawing a freehand region of interest on the PACS screen.
PFT
All patients and controls performed PFT according to a standardized protocol and guidelines set by the American Thoracic Society/European Respiratory Society (ATS/ERS)19,20 and included spirometry, and determination of static lung volumes and gas diffusing capacity. All measurements were made using an automated Vmax V6200 system (VIASYS Respiratory Care). Recorded variables were forced vital capacity (FVC), forced expiratory volume in 1 s (FEV1), total lung capacity (TLC), DLCO, and DLCO divided by alveolar volume. The values were recorded in absolute terms and as the percentage of the predicted value. Predicted values were derived from reference equations for each sex, with age and height as predictor variables. Low values for FVC, FEV1, DLCO, and TLC were defined as < 80% of predicted; a low value for FEV1/FVC was defined as < 0.70. These cutoff points correspond to the lower 5th percentiles in reference material and are in accordance with ERS recommendations21.
The 6-min walk test (6MWT)
The 6MWT was carried out on a straight indoor line measuring 35 m, according to ATS guidelines22. All participants scored their level of exhaustion on a modified Borg scale23 using values from 0 (no dyspnea) to 10 (maximal exhaustion).
Statistical analyses
Differences between patients and controls, and between patients at Time 1 and Time 2, were tested with the paired sample t test for continuous, normally distributed variables, Wilcoxon rank-sum test for non-normally distributed variables, and McNemar test for categorical variables. To test differences between patients with and without ILD, we used the independent sample t test for continuous normally distributed variables, Mann–Whitney U test for non-normally distributed variables, and the chi-square test or Fisher’s exact test for differences in categorical variables. Correlations between extent of ILD, DLCO, and FVC were determined by the Spearman correlation coefficient. To identify factors associated with ILD, we undertook univariable logistic regression analyses on disease-related variables from the time of diagnosis. Statistical analyses were undertaken with SPSS v22.0 (IBM).
RESULTS
The patients were mean 28.0 (SD 10.3) years old upon examination (median 27.4, range 11.8–53.8 yrs) and had a median duration of disease of 15.7 (range 0.6–41.2) years from symptom onset (Table 1). The controls were mean 29.0 (SD 10.2) years.
Characteristics in patients with JMCTD and controls from the general population. Values are mean (SD) or median (range) unless otherwise specified.
Compared with controls, patients were shorter (166.0 vs 170.1 cm, p = 0.016), and had a lower body weight (63.0 vs 68.1 kg, p = 0.033). Patients and controls reported a similar amount of physical activity and smoking habits. Two patients reported dyspnea upon exertion, one of whom had coronary artery disease. None of the controls reported pulmonary symptoms.
Pulmonary function in patients and controls
PFT values were impaired in 69% of the JMCTD patients and 25% of controls (p < 0.001; Table 2). The most commonly impaired PFT was DLCO (low in 67% of patients and 17% of controls, p < 0.001). FVC was impaired in 21% of patients and zero controls (p < 0.001). TLC was impaired in 12% of patients and zero controls (p = 0.009). Patients walked a mean 65 m less on the 6MWT than controls (p = 0.002). PFT and the 6MWT remained significantly lower in patients than in their matched controls even after excluding patients with ILD on HRCT (data not shown).
Pulmonary function after mean 16.2 years of disease duration in patients with JMCTD and controls. Values are mean (SD) or median (range) unless otherwise specified.
HRCT findings in patients
Fourteen patients (27%) had ILD on HRCT (reticular pattern, ground-glass attenuation, interlobular septal thickening, airspace consolidations, and/or traction bronchiectasis; Table 3). The most common abnormality was a reticular pattern, which was present in 13 patients (25%).
HRCT findings in 52 patients with JMCTD after mean 16.2 years of disease duration.
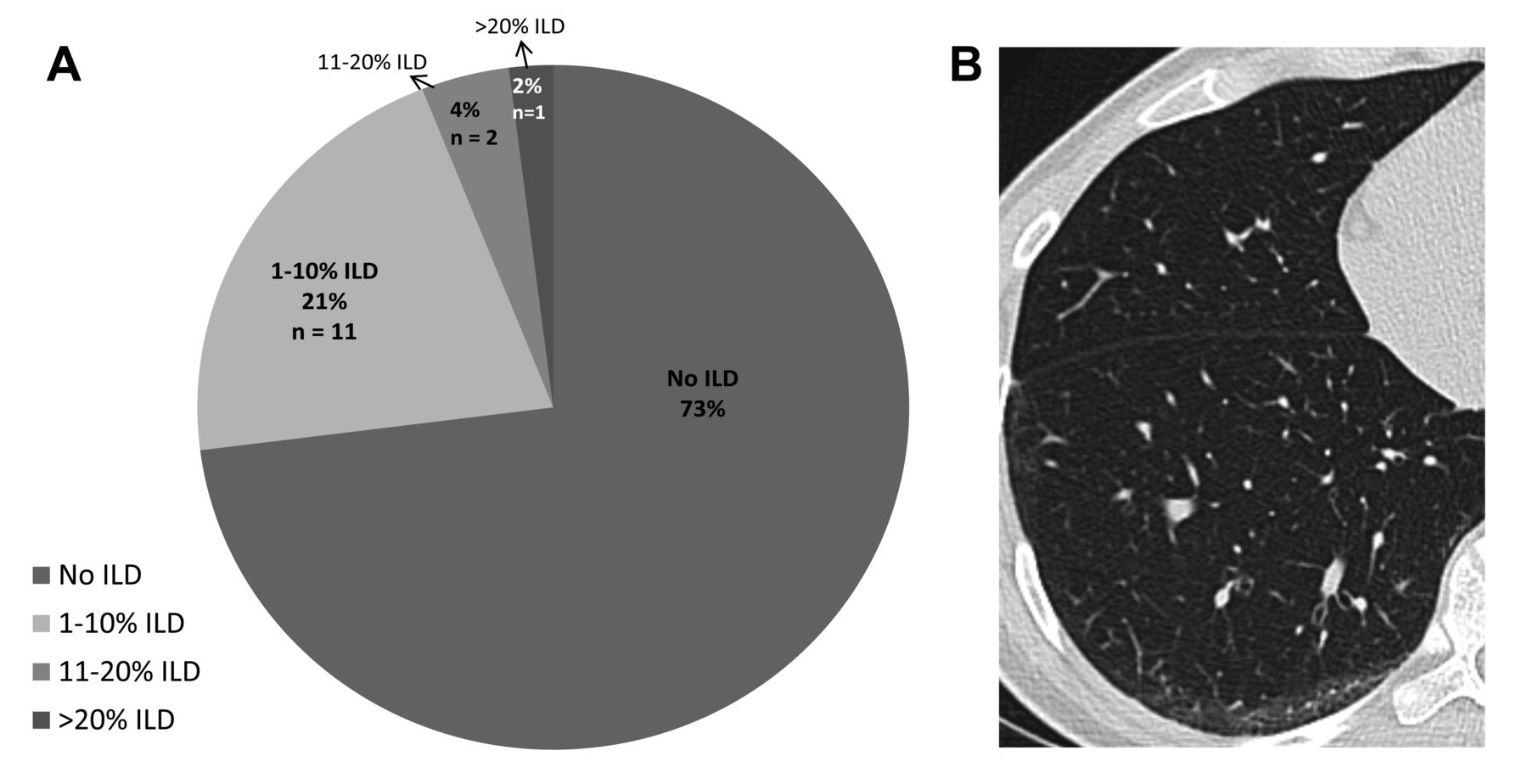
The extent of ILD was a median of 4% (range 1–75%) of the lung volume. Most (11/14) cases showed involvement of ≤ 10% of TLV (Figure 1). The remaining 3 patients had 12%, 18%, and 75% of the lung parenchyma affected, respectively. Of the 14 patients with ILD, only the patient with 75% involvement of the lung reported pulmonary symptoms (dyspnea upon exertion).

HRCT abnormalities in JMCTD. A. ILD extent in percent of total lung parenchyma. B. HRCT image of a typical patient with JMCTD, with a fine reticular pattern grade 1 and 2, and 7% of total lung volume involved. HRCT: high-resolution computed tomography; JMCTD: juvenile mixed connective tissue disease; ILD: interstitial lung disease.
A reticular pattern was most often found in the basal lung zone (11/14 patients, 79%). Seven of 14 cases (50%) had findings between the inferior pulmonary veins and the level of the carina, 6/14 (40%) between the level of the carina and aortic arch, and 3/14 (20%) above the aortic arch (data not shown).
Associations between ILD and patient characteristics, disease variables and PFT
A higher proportion of patients with ILD had low FVC (43% vs 14%, p = 0.023) and low TLC (36% vs 3%, p = 0.002) compared with those without ILD (Table 4). Patients without ILD had more often been treated with corticosteroids (90% vs 64%, p = 0.033) and antimalarial agents (92% vs 57%, p = 0.003) than those with ILD. The use of corticosteroids (but not antimalarial agents) correlated with SLE-like disease at the time of examination (r = 0.41, p = 0.003). The extent of ILD correlated negatively with FVC% predicted (r = −0.64, p = 0.01) and DLCO% predicted (r = −0.81, p < 0.01) at Time 2, but not with other disease-related variables at the diagnosis or after a mean of 16 years (data not shown).
Patient and disease characteristics in 52 patients with JMCTD with and without ILD at examination after 16.2 years disease duration. Values are n (%) or median (range) unless otherwise specified.
Progression of HRCT findings and changes in PFT values
Changes in HRCT and PFT values in 37 and 38 patients, respectively, over a median of 8.8 and 10.3 years are shown in Table 5. Values of FVC and FEV1 declined significantly, but the DLCO was stable from Time 1 to Time 2. There was no significant increase in ILD findings with regard to the extent, presence, or grade of the reticular pattern between Time 1 and Time 2.
Progression of HRCT findings (n = 37) and changes in PFT (n = 38) in patients with JMCTD. Values are mean (SD) or median (range) unless otherwise specified.
DISCUSSION
In this longterm outcome study of 52 patients with JMCTD, we found ILD in 27% after mean disease duration of 16.2 years. Most cases had < 10% of lung parenchyma involved. Compared with controls, patients had lower values for FVC, DLCO, and TLC. ILD was associated with low values for FVC and TLC. No significant progression in ILD was observed over time. To our knowledge, this is the first systematic case-control study on pulmonary manifestations, and the first to assess the presence and progression of ILD in an unselected cohort of patients with JMCTD.
The prevalence of ILD in adult MCTD has been reported to be 35–78%2,3,4,5,6,7. Recently, Reiseter, et al observed ILD in 41% of 119 patients after a mean duration of disease of 16.5 years3. In our cohort of JMCTD cases, a lower prevalence of 27% of cases with ILD was noted, even though our patients had a comparable long duration of disease. Two studies on JMCTD have also reported the ILD prevalence to be in the lower range. Mier, et al13 found pulmonary fibrosis on CT in 30% of 10 patients believed to be at risk of ILD. Aaløkken and colleagues reported a prevalence of ILD of 25% in 24 patients with JMCTD after a median duration of disease of 10.5 years12. In juvenile SSc and dermatomyositis, the prevalence of ILD has been reported to be 21% and 14%, whereas in juvenile SLE, ILD rarely occurs24,25,26. Thus, a prevalence of ILD of 27% in our study is in accordance with that reported in JMCTD, but lower than that reported in most studies of patients with adult MCTD. However, compared to other pediatric connective tissue diseases, ILD is a frequent finding in JMCTD.
Most of our patients had mild fibrosis, and only 6% had lung involvement of > 10%. These findings are in accordance with those reported by Aaløkken and colleagues in patients with JMCTD12. With respect to adult MCTD, however, Reiseter, et al found a much higher proportion (17%) of cases with involvement of > 10% of TLV3. Further, in a large cross-sectional study with 126 adult patients, Gunnarsson, et al reported that 19% of cases had severe fibrosis2. According to our results, not only the prevalence but also the severity of ILD in JMCTD seems to be lower than that in adult MCTD.
Impaired lung function was found in 69% of our patients, and values of FVC, FEV1, DLCO, and TLC were reduced significantly compared with those in controls. The most commonly impaired PFT was DLCO, which was noted in 65% of cases. However, on a group level, the reduction was only moderate. Patients with ILD and impaired PFT were mainly asymptomatic; only 1 patient reported symptoms of ILD. The 6MWT was clearly reduced compared with that of controls, but within the expected normal range27, supporting the notion that lung function impairment in JMCTD is common but mostly mild. We did not use mild asthma and smoking as exclusion criteria, which could explain the somewhat unexpected finding that 25% of controls had abnormal PFT.
Low values of FVC and TLC were associated significantly with ILD. In contrast, low DLCO was not associated with ILD, even though it was the most commonly impaired PFT in JMCTD. Abnormal DLCO has also been described to occur commonly in other types of connective tissue disease in children. In a cohort of 60 juvenile patients with SLE, Lilleby, et al found low DLCO in 35% and none of them had findings of ILD on HRCT26. Further, in juvenile dermatomyositis, Sanner, et al described low DLCO in half of 59 patients without association with ILD25. Thus, in JMCTD, low DLCO cannot be explained by restrictive lung disease alone, but may be due to other causes, such as pulmonary vascular disease28 or structural changes in alveolar membranes29. In addition, in SSc, fibrosis has been shown to be better predicted by FVC than by DLCO30,31,32,33.
Our data showed no significant progression of ILD over a mean observation period of 8 years. In adult MCTD, Kawano-Dourado, et al6 found limited ILD progression over 10 years, with an increase in lower-lobe ILD score from 7.5 to 11.2%. Reiseter, et al3 found modest progression of ILD in 19% of cases over 6.4 years, with an increase in median extension of ILD from 5% to 7%. The presence and extent of ILD are prognostic factors for increased mortality in MCTD2,3. Our data imply that ILD in JMCTD is mostly stable over longterm disease duration, but we cannot exclude that mild ILD in these patients should be of concern, because lung function declined over time.
Patients without ILD after mean disease duration of 16 years had more often been treated with prednisolone and antimalarial agents than patients with ILD. Although we cannot make conclusions based on these associations, because of the relatively small sample size and low number of patients with ILD, these are relationships that could be assessed in more depth in larger studies. We found no associations between ILD and disease activity measurements or smoking status. Reiseter and colleagues showed male sex, presence of anti-Ro52 antibodies, and a high level of anti-RNP antibodies to be predictors for ILD progression in adult MCTD3, but none of these factors was associated with ILD in our cohort.
Our present study had 2 main limitations. The first was the small cohort of patients; in particular the results regarding the subgroup of patients with ILD should be interpreted with caution, because these analyses are more exploratory in their characteristics. However, compared with other relevant studies, our cohort was the largest cross-sectional study carried out on JMCTD. Second, ideally, we should have had data on all 52 patients also at Time 1, and we cannot exclude that the study was underpowered with regard to assessing ILD progression.
The main strength of our study was that it was the first, to our knowledge, to compare JMCTD patients with a control group. It was also the largest study to assess HRCT and PFT systematically in all patients, and the cohort is considered representative of patients with JMCTD living in Norway, as described in more detail previously17. Progression of pulmonary manifestations in patients with JMCTD has not previously been reported, and we had a long followup of 16.2 years from the diagnosis. All HRCT, from Time 1 and Time 2, were examined by the same experienced radiologist using a standardized method.
Our longterm study showed that compared to matched controls, patients with JMCTD had impaired pulmonary function. ILD was found in 27% of patients, mostly as mild disease. The presence and extent of ILD did not progress. These findings suggest that ILD is stable in JMCTD, and that the progression and severity of ILD is less prevalent than that reported in adult-onset MCTD. Our results may imply that asymptomatic JMCTD patients with mild ILD can be followed with regular PFT alone, but repeated HRCT should be considered in cases of unexplained pulmonary symptoms or reduction in PFT.
Acknowledgment
The authors acknowledge Helga Sørhøy for practical assistance in examining the patients, Torhild Garen for help with preparation of questionnaires, and Øyvind Molberg and Inge-Margrethe Gilboe for administrative support.
Footnotes
This study was funded by The Norwegian Rheumatism Association and made possible by the Norwegian ExtraFoundation for Health and Rehabilitation.
- Accepted for publication May 10, 2018.








{kind=link}