

Abstract
Objective. To assess the reproducibility and the utility of the 6-minute walk test (6MWT) in systemic sclerosis (SSc).
Methods. All patients with SSc who underwent at least two 6MWT within a minimum 3-month interval plus simultaneous routine clinical, biological, and functional evaluations were consecutively enrolled in this observational study over 6 years. Following American Thoracic Society guidelines, each 6MWT was repeated twice to assess the 6-minute walk distance (6MWD) reproducibility, with the highest value being reported for subsequent analysis.
Results. Among 56 (38 female) included patients aged 46 ± SD 12.7 years, with 17 ± 10 modified Rodnan skin score (mRSS) and 1 ± 0.8 Scleroderma Health Assessment Questionnaire (SHAQ) at first referral, 277 6MWT evaluations (5 ± 3.9 6MWT per patient) were performed over 23 ± 22.5 months followup. Meanwhile, 8 deaths (87.5% SSc-related) occurred. The mean 6MWD absolute value was 457 ± 117 m with a 4 ± 2.2 mean Borg dyspnea score. The 6MWD intraclass correlation coefficient was 0.996 (95% CI 0.995–0.999, p < 0.0001). In multivariate linear regression analysis, these factors were independently associated with a lower 6MWD: sex (R2 = 0.47, p < 0.0001), mRSS (R2 = 0.47, p = 0.008), tendon friction rub (R2 = 0.47, p = 0.003), SHAQ (R2 = 0.47, p = 0.02), muscle disability score (R2 = 0.47, p = 0.03), DLCO% (R2 = 0.47, p = 0.0008), and left ventricular ejection fraction (R2 = 0.47, p = 0.006). The 6MWD at first referral was an independent predictor for the overall mortality (HR 0.99, 95% CI 0.988–0.999) and the SSc-related mortality (HR 0.99, 95% CI 0.988–0.999).
Conclusion. We show strong reproducibility for the 6MWD and confirm the 6MWT utility to assess the overall prognosis of patients with SSc.
The 6-minute walk test (6MWT) is a simple, submaximal aerobic exercise test, currently used in idiopathic pulmonary fibrosis, all types of pulmonary arterial hypertension (PAH), or in chronic heart failure, to assess disease severity and the patient’s prognosis1,2,3. It is indicated as a single measurement of functional status for patients with heart failure, chronic obstructive pulmonary disease (COPD), and PAH, and as a predictor of morbidity and mortality in patients with heart failure, COPD, or PAH. The 6MWT is indicated for pre- and posttreatment comparisons, especially for patients with PAH3. According to the American Thoracic Society (ATS) practical guidelines4, the 6MWT is “easy to administer, better tolerated and more reflective of activities of daily living than the other walk tests.” This safe, noninvasive test requires no exercise equipment nor advance training for technicians5,6. Therefore, the 6MWT has become an important outcome measure in many clinical trials for idiopathic PAH7,8 and has been used progressively for pulmonary hypertension [due to lung diseases or PAH associated with connective tissue disease, including systemic sclerosis (SSc)]9. In 2008, the expert panel on outcome measures in PAH and interstitial lung disease (ILD) related to SSc for the Expert Panel on Outcome Measures in PAH related to Systemic Sclerosis (EPOSS)-Outcome Measures in Rheumatology (OMERACT) group, using a Delphi consensus study with cluster analysis, recommended use of the 6MWT in SSc clinical trials10. After a systematic literature review, the EPOSS-OMERACT group found insufficient data to completely validate the 6MWT reproducibility and sensitivity to change over time11. Ten years later, very few studies have yet analyzed the correlations between the 6MWT results and patients’ clinical characteristics12,13,14, and its reproducibility has only been assessed once in SSc patients with ILD15. In addition, Sanges, et al recently reported that the 6-minute walk distance (6MWD) was not an accurate surrogate marker for SSc-PAH hemodynamics when analyzing 2 independent cohorts of French (2006–2009) and US (1998–2006) patients16.
We therefore designed the present prospective study to investigate the reproducibility and the utility of the 6MWT in an unselected population of patients with SSc, when performed during routine patient followup evaluation in a tertiary referral center for SSc.
MATERIALS AND METHODS
Population
All patients with limited or diffuse SSc, as defined according to the American College of Rheumatology criteria17 and the LeRoy and Medsger criteria18, and referred to Hôpital Saint-Louis SSc tertiary center from November 2002 to November 2008, were consecutively enrolled in this observational study if they underwent at least 2 successive 6MWT within a minimum 3-month interval and if data from simultaneous clinical and biological evaluation during their routine followup were available. This observational study was conducted between 2002 and 2008 on the 6MWT according to routine clinical care in an expert center for SSc and following treatment protocols. Considering the French legislation at that time, there was no requirement for ethics or institutional review board committee approval. All patients gave written informed consent for data collection and analysis.
Within a maximum of 1 week before or after the 6MWT, the following clinical and biological data were collected at first referral and at each testing evaluation: (1) age, sex, disease duration (since onset of first non-Raynaud phenomenon), body mass index, SSc subtype according to Leroy and Medsger18, World Health Organization performance status (PS), Scleroderma Health Assessment Questionnaire (SHAQ) ranging from 0 (normal) to 3 (maximum)19, presence of arthralgia or tendon friction rubs20, muscle disease score (MDS) ranging from 0 (normal) to 75 (maximum disability)21; (2) extension of skin fibrosis as measured by the Rodnan modified skin score (mRSS)22; and (3) cardiac and pulmonary evaluation, including systolic and diastolic arterial blood pressure, heart rate, respiratory rate, functional class according to New York Heart Association (NYHA) at rest, presence of pulmonary rales, results from pulmonary function tests [forced vital capacity (FVC), DLCO], according to the ATS and European Respiratory Society (ERS) consensus standards23, presence of SSc-related ILD or pleural effusion on chest radiograph or on high-resolution computed tomography (HRCT), results from echocardiography including left ventricular ejection fraction (LVEF), tricuspid regurgitation peak velocity (TRV; m/s), and pulmonary arterial systolic pressure (PASP; mmHg) measurement. When PASP at rest on Doppler echocardiography was > 35 mmHg or TRV > 2.7 m/s, right heart catheterization was performed. PAH was confirmed as a mean pulmonary arterial pressure ≥ 25 mmHg and was considered an SSc-associated precapillary PAH when associated with a pulmonary artery wedge pressure ≤ 15 mmHg. Laboratory variables included hemoglobin level, serum creatinine, C-reactive protein, creatinine kinase, antinuclear (ANA), anticentromere (ACA), and antitopoisomerase I antibodies status. Patient survival status was evaluated during and at the end of the whole cohort followup.
6MWT
Following the ATS guidelines4, each 6MWT was performed indoors along 30-m straight, flat, hard surface corridor. Patients had not exercised vigorously within 2 h before the beginning of the test. It was undertaken without additional oxygen and administered by the same tester (KG) not involved in the patient’s daily care, at the same location throughout the study. The instructions to patients were: “Walk as far as possible for 6 min. You will walk back and forth in this hallway. Six minutes is a long time to walk, so you will be exerting yourself. You will probably get out of breath or become exhausted. You are permitted to slow down, to stop, and to rest as necessary. You may lean against the wall while resting, but resume walking as soon as you are able to.” The 6MWT was terminated before 6 min elapsed if blood oxygen saturation went < 80%, or exhaustion, chest pain, intolerable leg cramps, or diaphoresis occurred. Following clear instructions, the walking distance achieved between 0 and 6 min (6MWD in m) was recorded as absolute value. The Borg dyspnea score was recorded at the end of each 6MWT24. To lower the variations induced by age, height, weight, sex, we used the Enright’s reference equation5 to calculate the 6MWD relative value (%) for each individual adult patient performing the test for the first time. This equation is a ratio given by the value of the 6MWD measured in patients over the theoretical reference-predicted distance of the 6MWD for healthy adults. The predicted distance is defined as follows for men: 6MWD = [7.57 × height (cm)] − (5.02 × age) − [1.76 × weight (kg)] − 309 m; and for women: 6MWD = [2.11 × height (cm)] − (5.78 × age) − [2.29 × weight (kg)] + 667 m. The 6MWD was considered abnormal if it was < 80% of the normal range predicted by the Enright’s equation.
Two successive 6MWT were performed at each evaluation: the first, called 6MWT1 and designed by ATS as a “practice test,” was followed by 6MWT2, performed at least 1 h later and on the same day. All included patients repeated the test twice at each evaluation during consecutive clinical followup visits. All 6MWD1 and 6MWD2 values were computed to assess the intratest 6MWT variability and reproducibility. The highest 6MWD recorded was considered as the patient’s final result for a single evaluation.
Statistical analysis
Categorical variables were summarized as numbers and percentages, and numerical variables as mean ± SD. We used the Bland-Altman plots method25 to evaluate the agreement between each 6MWD1 and 6MWD2 measurement, then calculated the intraclass correlation coefficient (ICC) between both measures to determine the 6MWD reproducibility. Patient referral characteristics between those with normal and abnormal 6MWD (< 80% predicted) were compared using chi-square and Student t test. Results from the repeated evaluations during routine clinical followup were computed to assess the 6MWT sensitivity to change and its predictive value. Correlations between the 6MWD absolute values and patients’ clinical and paraclinical characteristics at first referral and during followup were assessed by univariate linear regression. Then, all variables identified with a p value < 0.05 in the univariate analysis were computed for the multivariate model (stepwise ascending procedure). Correlation between 6MWD absolute value and survival was assessed using a Cox proportional hazards model, expressed as HR and 95% CI and adjusted for age and sex. All tests were 2-sided with a significance level of p < 0.05. Statistical analysis was performed using SAS software version 9.3 (SAS Institute).
RESULTS
Patient characteristics and 6MWT results at first referral
Over the 6-year study period, 56 consecutive patients with SSc (68% female) were prospectively included after 33.6 ± SD 44 months of disease duration. At first referral, their mean age was 45.6 ± 13 years, performance status was 0 (19.6%), 1 (62.5%), or 2 (17.9%), with a SHAQ value at 1.02 ± 0.77. There were 39 patients (70%) who had diffuse cutaneous SSc. Mean mRSS was 17 ± 10 (range 0–43); all patients tested positive for ANA, 33 (59%) with antitopoisomerase I, and 5 (9%) with ACA. Other disease characteristics and drugs exposure at first referral are in Table 1. Blood pressure, heart rate, and LVEF on echocardiography were within the normal range at first referral 6MWT, with a mean PASP 32 ± 9 mmHg, while the other organ involvement measures showed the presence of the following: dyspnea NYHA grade 2 (38.9%) or 3 (8.3%), tendon friction rubs (9.1%), arthralgia (46.3%), and a 7.8 ± 9 MDS score. Pulmonary function tests showed 84 ± 26% of predicted FVC and 58 ± 17% of predicted DLCO with ILD present on chest radiograph or on HRCT in 31 patients (67%). Three patients (5.4%) had SSc-related PAH confirmed on right heart catheterization, of whom 1 (0.8%) was under oxygen therapy at first referral. Overall, the mean 6MWD absolute value was 457 ± 117 m (6MWD relative value 74.7 ± 20%), with a 4 ± 2.2 mean Borg scale at the end of the 6MWD for all 56 patients with SSc, of whom 25 (44.6%) completed an abnormal 6MWD (< 80% predicted) with 373 ± 106 m mean 6MWD absolute value (6MWD relative value 57.6 ± 15%).
Baseline clinical characteristics of the 56 patients with SSc at time of first referral evaluation and 6MWT. Values are mean ± SD or n (%).
When compared to SSc patients with normal 6MWT, those with abnormal 6MWD (< 80% predicted) at first referral were significantly younger (41 ± 12 yrs vs 49 ± 12, p = 0.01), had more severely impaired functional status (PS 2: 32% vs 6.5%, p = 0.01; SHAQ: 1.3 ± 0.7 vs 0.8 ± 0.7, p = 0.005), higher MDS score (10.7 vs 5.4, p = 0.001), more frequent arthralgia (74 vs 23%, p = 0.001) and tendon friction rubs (20 vs 0%, p = 0.02), more severely altered lung function (FVC% theoretical values: 77 ± 24 vs 91 ± 26, p = 0.05; DLCO% theoretical values: 53 ± 17 vs 62 ± 16; p = 0.05; and lower LVEF%: 65 ± 8 vs 72 ± 8, p = 0.003).
Patient outcomes and repeated 6MWT during followup
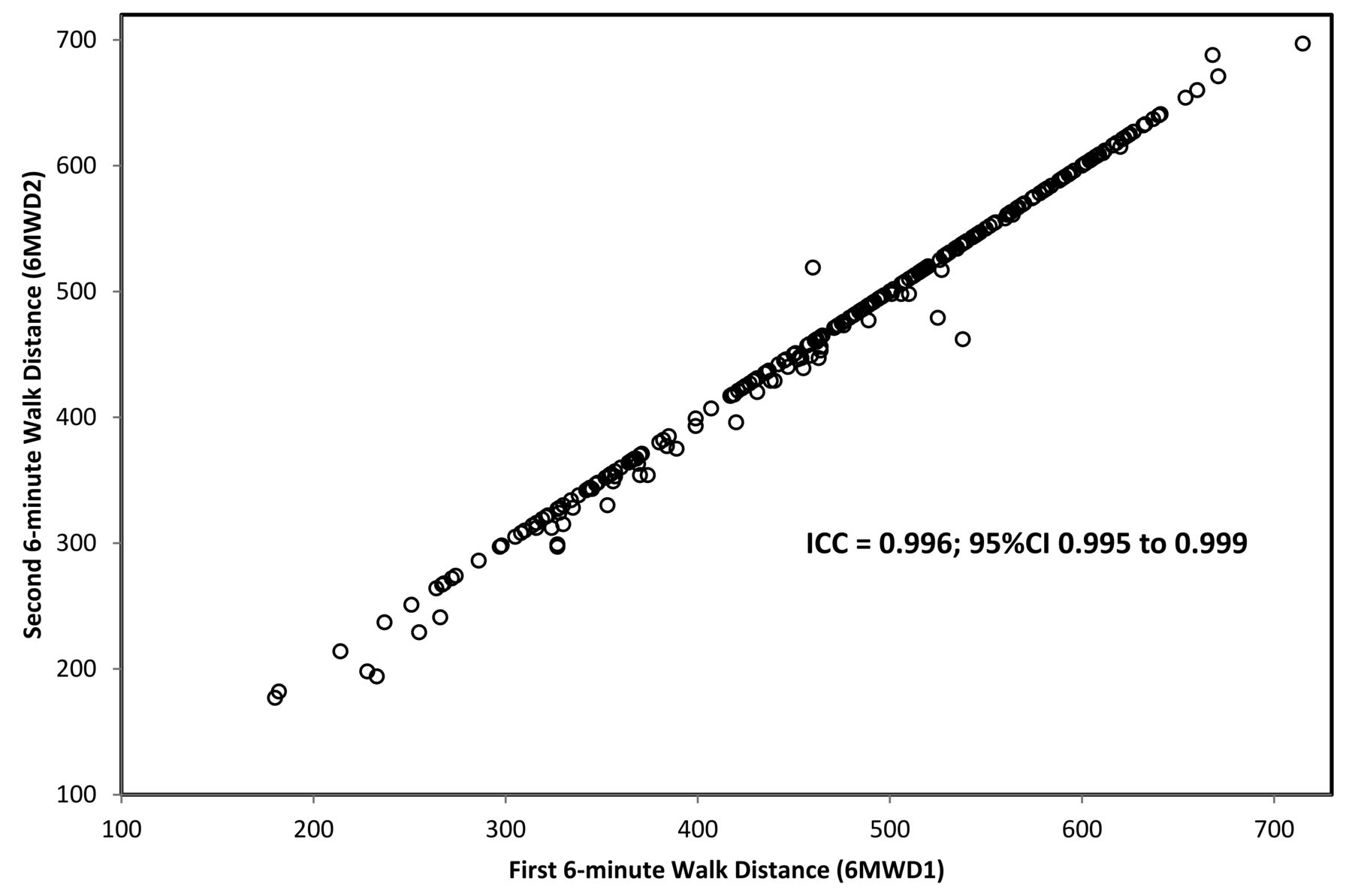
Within 23.3 ± 22.5 months mean followup for the whole cohort, 5.0 ± 3.9 evaluations per patient were performed. The 6MWD was repeated twice at each evaluation and the mean post-6MWT Borg dyspnea index was 3.9 ± 2 (n = 277). Out of 544 single 6MWD measures collected, the mean absolute 6MWD1 and 6MWD2 values were 468 ± 115 m and 475 ± 112 m, respectively. Bland-Altman plot showed good agreement for repeated 6MWD in SSc (Figure 1). The 6MWD ICC was 0.996 (95% CI of 0.995 to 0.999, p < 0.0001), demonstrating a strong reproducibility (Figure 2).
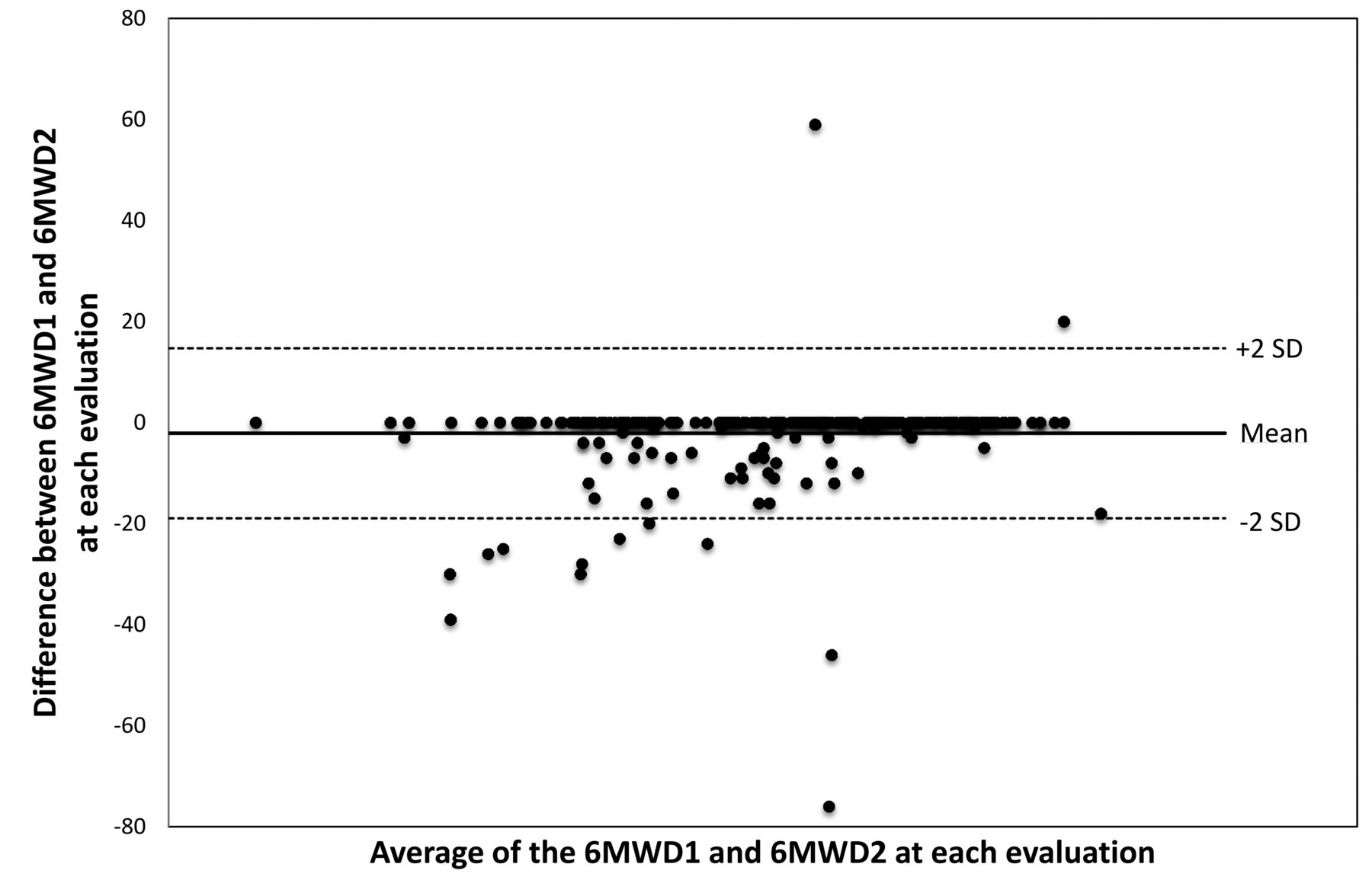
Bland-Altman plot of the 6-minute walk distance (6MWD) in 56 patients with systemic sclerosis.
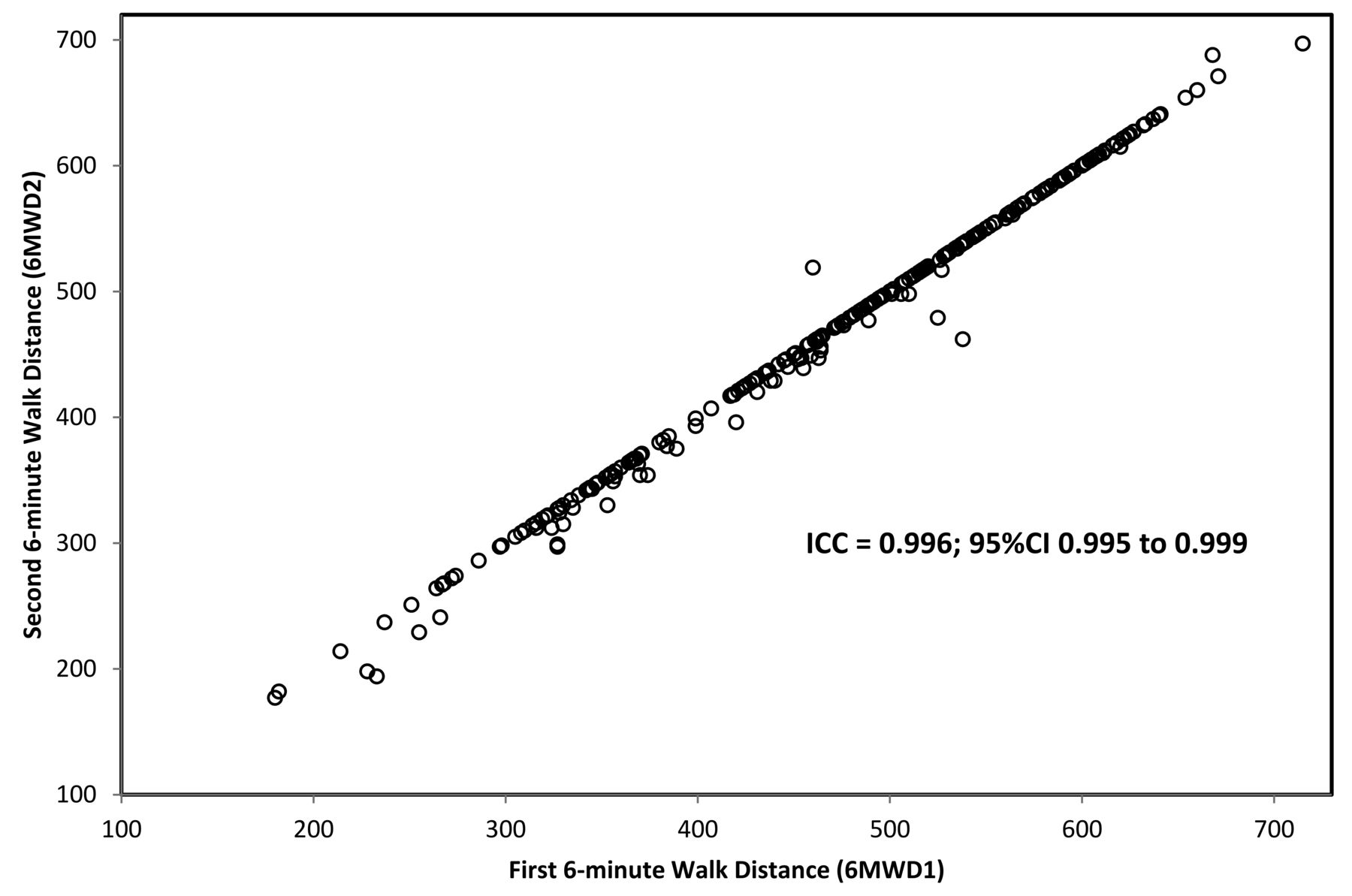
Intertest reproducibility of the 6-minute walk distance (6MWD) in 56 patients with systemic sclerosis. Two 6MWD were performed at first referral and at each followup evaluation, with the total 6-min distance walked being recorded (m). ICC: intraclass correlation coefficient.
Correlations of the 6MWT with SSc patient characteristics at baseline and during followup
As detailed in Table 2, univariate analysis using linear regression showed that the 6MWD absolute value at any evaluation point from first referral up to last followup among all 56 patients with SSc significantly correlated with several clinical, functional, and biological variables. In multivariate analysis, these were independent predictors of the 6MWD and accounted for 47% of the 6MWT variance: sex (R2 = 0.47, p < 0.0001), SHAQ (R2 = 0.47, p = 0.02), mRSS (R2 = 0.47, p = 0.008), presence of tendon friction rub (R2 = 0.47, p = 0.003), MDS score (R2 = 0.47, p = 0.03), DLCO% (R2 = 0.47, p = 0.0008), and LVEF% (R2 = 0.47, p = 0.006).
Correlation between 6MWD (absolute value, m) and SSc patient characteristics (univariate linear regression).
Mortality
At the end of followup, 8 deaths (14.3%) had occurred: 7 related to SSc (2 from disease progression, 5 from ILD worsening) and 1 from esophagus cancer and liver cirrhosis. Six deaths (10.7%) were observed among patients with abnormal 6MWD (< 80% predicted) at first referral and 2 (3.6 %) among those with normal 6MWD initially (p = 0.03). The 6MWD absolute value at first referral was an independent predictor for both the overall mortality (adjusted HR 0.99, 95% CI 0.988–0.999; p = 0.024) and SSc-related mortality (adjusted HR 0.99, 95% CI 0.988–0.999; p = 0.039), a 1% improved survival for 1 additional m carried out.
DISCUSSION
SSc is a rare heterogeneous autoimmune disease characterized by excessive and progressive fibrosis due to collagen deposition in the skin and internal organs (lung, gastrointestinal, cardiovascular, and renal). Early detection and followup management of PAH and ILD are recommended26,27, because they remain the leading causes of death in SSc28,29,30. Therefore, noninvasive clinical tools are essential for accurate and repeated screening of frequently coexisting cardiac and lung involvement in patients with SSc.
According to the 2002 ATS guidelines, the 6MWT is a common, practical, and simple test to evaluate the overall response of integrated organ systems in patients with various types of pulmonary or cardiac diseases. A single 6MWT allows the assessment of the functional exercise capacity in daily practice, while repeated testing evaluates pre- and posttreatment followup. In patients with moderate to severe heart or lung disease and in idiopathic PAH or pulmonary fibrosis, the 6MWT is an independent predictor of mortality4,31,32. This test has been accepted by the US Food and Drug Administration as a primary outcome measure in the development and approval of PAH drugs4. However, the value obtained in idiopathic PAH could not be generalized to SSc-PAH33, and few studies have assessed the 6MWT value in SSc. In a metaanalysis of 43 retained papers that included 3185 SSc patients tested from 1996 to 2016, no data were available in those without ILD and PAH, nor on the evolution of the 6MWD over time33. In addition, the 6MWD data were missing in up to 30% of the included SSc-ILD–PAH patients, without explanation. Two other studies raised doubts about the 6MWT specificity and relevance, because of multiple organ involvement in SSc12,15.
As recommended by the EPOSS-OMERACT experts10, this prospective observational study specifically evaluated the 6MWT in an unselected SSc population during routine clinical followup. We performed the 6MWT as originally described by Guyatt, et al34. Following the ATS guidelines, a practice test was performed to report the highest 6MWD as an absolute value4. The 6MWD results are very sensitive to variations in methodology (e.g., use of encouragement, provision of oxygen, changes in track layout and length)31. Shorter height, older age, higher body weight, female sex, pulmonary and cardiovascular diseases, and musculoskeletal disorders may all reduce the 6MWD. SSc cardiac and pulmonary involvement, as studied by Garin, et al in 75 patients with and without ILD or PAH35, but also musculoskeletal disease with arthralgia, tendon friction rubs, myositis, or pain may account for reduced 6MWD. Here, we used the validated version of SHAQ after prior adequate translation19, a reliable score used in daily practice and clinical trials to evaluate SSc disability19,36,37 and one of the best prognostic factors of survival at 2 years in diffuse SSc38. The significant correlation observed between the 6MWD and the SHAQ at any evaluation point during followup reinforces the significance of each test in this setting. Cardiac involvement is common in SSc, although it is subclinical for a long time. Once it is clinically apparent, cardiac involvement carries a very poor prognosis30,39,40,41,42. While the overall longterm prognosis of patients with SSc has improved in recent years, the proportion of deaths due to heart disease has not changed significantly, and monitoring of myocardial involvement is essential in SSc management43,44. Although all patients had normal LVEF at first referral, we found a strong significant correlation between 6MWD and LVEF, and also an independent statistical significant association with increased mortality (HR = 0.99, 95% CI 0.988–0.999; p = 0.02) at almost 2 years followup. Villalba, et al had showed that a 6MWD < 400 m was associated with transthoracic echocardiography PASP > 30 mmHg in SSc patients with lung involvement45. Sanges, et al reported correlations between 6MWD and baseline transthoracic echocardiography variables and hemodynamics in SSc-PAH without extensive ILD16. Three different studies using multivariate analysis had shown that the 6MWT was associated with measures of myocardial involvement, ILD, musculoskeletal disorders, and inflammation13,14,15. Our present prospective study of an unselected cohort of 56 patients with SSc shows relevant correlation between abnormal 6MWD (< 80% predicted) at first referral with the presence of heart, lung, skin, and musculoskeletal involvement within a relatively short followup of almost 2 years. Therefore, a low 6MWD effectively correlates with SSc disease severity, although it is nonspecific for the presence of PAH or ILD per se, because of multiorgan involvement. Importantly, the 6MWT is an independent predictor of survival.
Our study had several limitations. The cohort reflects patients usually followed in tertiary centers where most, but not all patients, had diffuse SSc. Patients unable to walk and perform the test at first referral were not included in the study. Irrespective of the diffuse or limited SSc subtype, it cannot be applied to patients with very advanced disease who are unable to perform the 6MWT because of muscle weakness, foot calcinosis, or joint pain, highlighting the major limitation of this test. This supports the validity that the 6MWT does not cover the whole range of SSc. Although bias is minimized by our statistical approach, unknown latent factors could also affect 6MWD variations not specific to SSc, such as variability in pulmonary function testing or transthoracic echocardiography, or variable responses to exercise testing. Different psychological responses to exercise (unrelated to disease) could lead to either a training effect or decompensation. However, the 6MWD reproducibility was strong in the tested population and this latter factor was not a confounding factor in results analysis.
This unselected SSc prospective cohort study first shows strong reproducibility for the 6MWD and that a “practice test” is no longer needed in SSc daily practice evaluation. It confirms 6MWT utility as a valid tool to assess functional capacity, with a significant prognostic value at first evaluation but also during followup in SSc patients with various degrees of organ involvement. In SSc, as in other clinical settings, the 6MWT is a sensitive test to indirectly evaluate SSc myocardial and pulmonary involvement and is an independent predictor of overall survival.
- Accepted for publication April 6, 2018.








{kind=link}
{kind=link}