

Abstract
Objective. Whether systemic sclerosis (SSc) confers increased risk of venous thromboembolism (VTE) is uncertain. We evaluated the prevalence, risk factors, and effect of VTE on SSc survival.
Methods. A cohort study was conducted of subjects with SSc who fulfilled the American College of Rheumatology/European League Against Rheumatism classification criteria between 1970 and 2017. Deep vein thrombosis was defined as thrombus on extremity ultrasound. Pulmonary embolism was defined as thrombus on thorax computed tomography angiogram. Risk factors for VTE and time to all-cause mortality were evaluated.
Results. Of the 1181 subjects, 40 (3.4%) experienced VTE events. The cumulative incidence of VTE was 2.7 (95% CI 1.9–3.7) per 1000 patient-years. Pulmonary arterial hypertension (PAH; OR 3.77, 95% CI 1.83–8.17), peripheral arterial disease (OR 5.31, 95% CI 1.99–12.92), Scl-70 (OR 2.45, 95% CI 1.07–5.30), and anticardiolipin antibodies (OR 5.70, 95% CI 1.16–21.17) were predictors of VTE. There were 440 deaths. There was no difference in survival between those with and without VTE (HR 1.16, 95% CI 0.70–1.91). Interstitial lung disease (HR 1.54, 95% CI 1.27–1.88) and PAH (HR 1.35, 95% CI 1.10–1.65) were predictors of mortality.
Conclusion. The risk of VTE in SSc is comparable to the general population. The presence of PAH, peripheral arterial disease, Scl-70, and anticardiolipin antibodies are risk factors for VTE. VTE does not independently predict SSc survival.
Venous thromboembolism (VTE) is a vascular phenomenon that includes deep vein thrombosis (DVT) and pulmonary embolism (PE). It is recognized that active systemic inflammation can augment coagulability and lead to thrombosis1. Systemic sclerosis (SSc) is characterized by vascular lesions, inflammation, and fibrosis2. Vasculopathy is associated with reperfusion injury and endothelial dysfunction, which may influence the onset of local thrombotic complications3,4,5. Whether there is an increased risk of VTE in SSc is being debated.
A metaanalysis evaluating the risk of VTE in inflammatory rheumatic disease concluded that inflammatory rheumatologic diseases were associated with a 3-fold higher risk of VTE compared to the general population1. However, the SSc-specific data were attributable to only 4 studies. One cohort study reported that people with immune-mediated disease may be at increased risk of subsequent VTE. However, that study included a range of immune-mediated diseases and was limited to inpatients or daytime specialist care6. Another retrospective cohort study of individuals admitted to hospital because of an autoimmune disorder found that autoimmune disorders were associated with increased risk of PE during the first year after admission. The standardized incidence ratio for SSc was 1.61 (95% CI 1.45–1.79). This study was potentially biased to the more severely ill, who required inpatient day hospital care7. The remaining 2 studies relied on administrative data. One population-based cohort study reported patients with SSc had a 10.5-fold increased risk of DVT and a 7.0-fold increased risk of PE compared with the general population8. Another population-based cohort study reported a relative risk of DVT of 5.0 (95% CI 2.7–9.4) and relative risk of PE of 4.0 (95% CI 2.1–7.6)9. However, both studies relied on International Classification of Diseases codes for case-finding and may have included other prothrombotic diseases such as systemic lupus erythematosus or overlap syndromes. Thus, it remains uncertain whether SSc confers an increased risk of VTE. Improved understanding of the relationship and effect of VTE on SSc may have implications for screening and anticoagulation treatment.
The aim of our study was to evaluate the epidemiology of VTE in SSc. We evaluated the cumulative incidence of VTE and compared our findings to that of the general population to ascertain whether SSc is associated with an increased risk of VTE. We evaluated risk factors for the development of VTE in SSc, and the effect of VTE on SSc survival.
MATERIALS AND METHODS
Subjects
The Toronto Scleroderma Program, a health network comprising 3 academic hospitals, is the largest single center longitudinal cohort in Canada10. Subjects who fulfilled the American College of Rheumatology/European League Against Rheumatism classification criteria for SSc were included11. Subjects with localized scleroderma, overlap syndromes, undifferentiated connective tissue disease, and an inherited thrombophilia were excluded. The study period was 1970–2017.
Outcomes
DVT was defined as the presence of thrombus of the upper extremity, femoral, or popliteal veins, or distal (calf) thrombosis with proximal extension on Doppler ultrasound. PE was defined as the presence of thrombus on thorax computed tomography (CT) angiogram. Ultrasound and CT scan were performed based on clinical suspicion. D-dimers and Well’s score were not used to stratify risk. Comparing those with and without VTE, we evaluated differences in disease duration, subtype, SSc manifestations, and comorbidities.
Differences in baseline characteristics between those with and without VTE included male sex, subtype of SSc (limited or diffuse, ascertained at baseline but revised if limited evolved into diffuse), SSc manifestations [calcinosis, Raynaud phenomenon, digital ulceration, symptomatic esophageal dysmotility on history, telangiectasia, abnormal nailfold capillaries on visual inspection, interstitial lung disease (ILD; forced vital capacity < 70%), and bibasilar reticular abnormalities with minimal ground glass on high resolution CT thorax]10, pulmonary arterial hypertension [PAH; mean pulmonary artery pressure (mPAP) > 25 mmHg and pulmonary capillary wedge pressure (PCWP) < 15 mmHg by right heart catheterization]12, renal crisis (acute renal failure, new onset hypertension, normal or mild proteinuria on urinalysis, microangiopathic hemolytic anemia), and serology (Scl-70 centromere antibodies).
Analysis
Descriptive statistics and relative risk (RR) with 95% CI were used to summarize the data. The prevalence of VTE in our cohort was compared to the general population using the Poisson distribution. We also evaluated prevalence by age, race, and sex. Logistic regression models were fit to evaluate risk factors for VTE. We evaluated model discrimination using the c statistic, and model calibration using the Hosmer-Lemeshow statistic. Patients who were alive on January 1, 2017, were right censored. All-cause mortality was the outcome for the survival models. The survival status of subjects who were lost to followup was systematically tracked through the hospital electronic record, family physician, referring physician, and online obituary databases. This approach has been shown to be a valid and reliable method of obtaining robust mortality data13, and has been successfully implemented in other studies10,14,15. Differences in survival were evaluated using Kaplan-Meier and Cox proportional hazards models. Analyses were conducted using RStudio (version 0.97.248).
Ethics
Institutional research ethics board approval was obtained prior to the conduct of this study (UHN REB 15-9209-AE, MSH REB 15-0256-C), and the study was conducted in compliance with the Helsinki Agreement.
RESULTS
Subjects
There were 1181 subjects [971 (82%) females, 210 (18%) males] who fulfilled eligibility criteria. In our cohort, there were 2 subjects with inherited thrombophilia (protein C deficiency, protein S deficiency), who were excluded from our study.
Frequency
There were 40 patients (3.4%) with unique VTE events. There were 20 DVT (1.7%) and 26 PE (2.2%) events. Of these, 6 (0.5%) had both a DVT and PE. The prevalence of VTE was 2.7 (95% CI 1.9–3.7) per 1000 patient years. Compared to a general population prevalence of VTE of 2 cases per 1000 persons16, the prevalence of VTE in SSc did not differ significantly from the general population (p = 0.07). We note that although 0.5% had both DVT and PE, subjects were not double-counted in the estimation of prevalence.
In subgroup analyses, the prevalence of VTE in SSc appears to increase with age, similar to the general population. There appears to be no differences in the incidence of VTE between males and females. The prevalence of VTE appears to be higher among African Americans compared to whites and Asians (Table 1).
Estimated prevalence of VTE by ethnicity, age, and sex.
Risk factors for VTE
Comparisons of SSc characteristics and comorbidities between those with and without VTE are summarized in Table 2.
Comparison of SSc subjects with and without VTE. Values are n (%) unless otherwise specified.
In unadjusted bivariate comparisons, the presence of these conditions was more prevalent in subjects who developed VTE: ILD (RR 1.67, 95% CI 1.26–2.20), PAH (RR 2.18, 1.75–2.71), Scl-70 antibody (RR 1.69, 95% CI 1.00–2.84), anticardiolipin antibodies (aCL; RR 6.11, 95% CI 1.83–20.4), coronary artery disease (RR 2.62, 95% CI 1.43–4.80), diabetes mellitus (RR 2.81, 95% CI 1.29–6.10), and peripheral arterial disease (RR 5.57, 95% CI 2.79–11.08). The subjects who had the presence of a lupus anticoagulant or aCL did not have antiphospholipid antibody syndrome. Independent predictors of VTE in SSc were PAH (OR 3.77, 95% CI 1.83–8.17), peripheral arterial disease (OR 5.31, 95% CI 1.99–12.92), Scl-70 (OR 2.45, 95% CI 1.07–5.30), and aCL (OR 5.70, 95% CI 1.16–21.17; Table 3). Subjects with ILD more frequently experienced DVT (RR 2.85, 95% CI 1.08–7.54) but not PE (RR 1.82, 95% CI 0.89–3.70). There was no significant difference in the occurrence of DVT (RR 0.95, 95% CI 0.46–1.97) or PE (RR 0.98, 95% CI 0.74–1.30) between SSc subtypes.
Summary of logistic regression model evaluating baseline predictors of survival.
Survival
There were 440 deaths. The probability of short-term (1-, 2-, 3-, 4-, 5-yr) and longterm (10-, 15-, 20-yr) survival, and median survival times between SSc subjects with and without VTE, are summarized in Table 4.
Survival probabilities and median survival time. Values are % (95% CI), except where indicated.
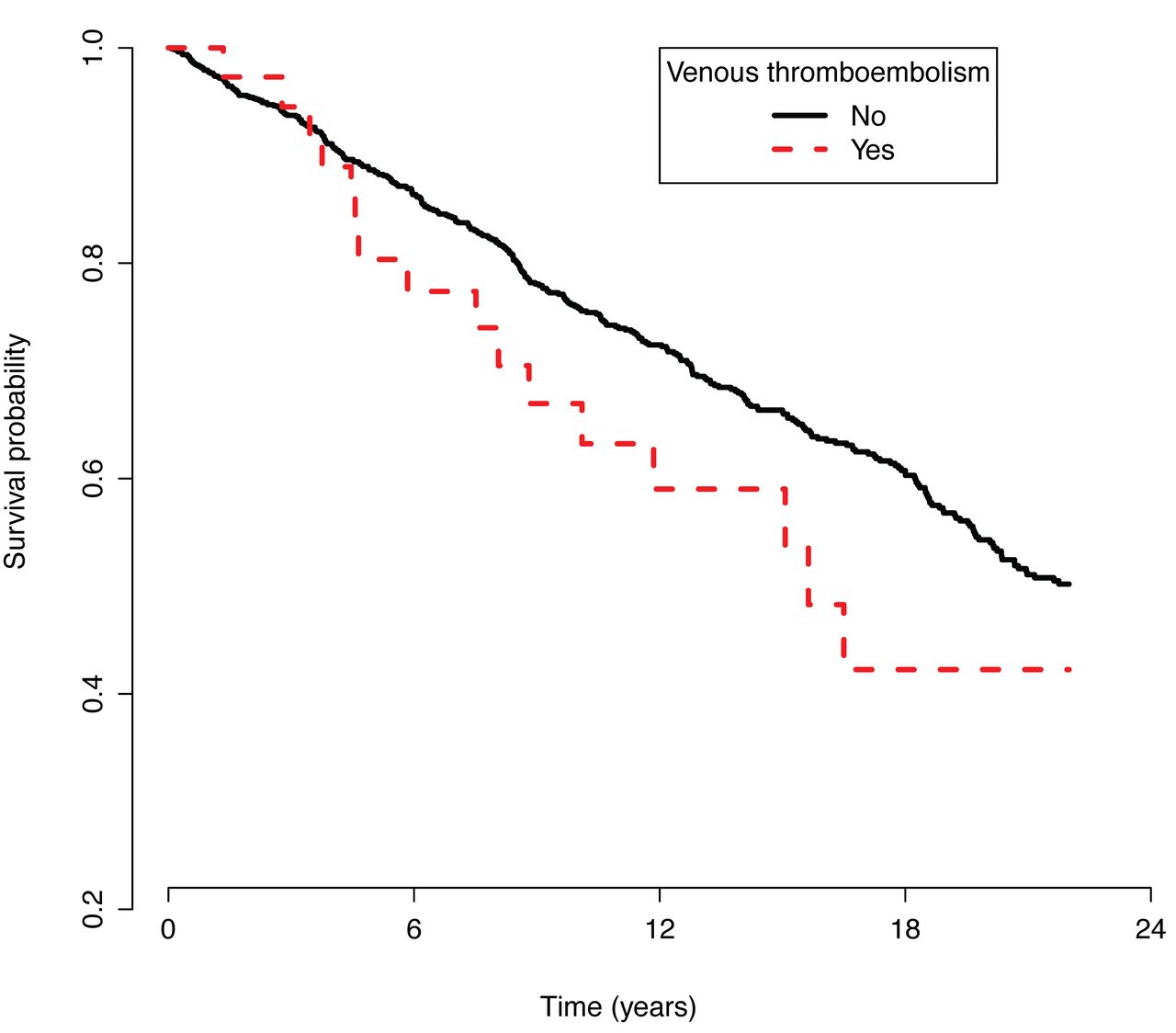
There were no significant differences in short-term survival between groups (log-rank test, p = 0.54). The Kaplan-Meier curves in Figure 1 suggest worsening longterm survival for the VTE group. There was no significant difference in the unadjusted survival between the 2 groups (HR 1.16, 95% CI 0.70–1.91). This was further attenuated (HR 1.02, 95% CI 0.62–1.67) after adjustment for the presence of ILD, PAH, Scl-70 antibody, aCL, coronary artery disease, diabetes mellitus, and peripheral arterial disease. Only the presence of ILD (HR 1.54, 95% CI 1.27–1.88) or PAH (HR 1.35, 95% CI 1.10–1.65) were independent predictors of mortality.
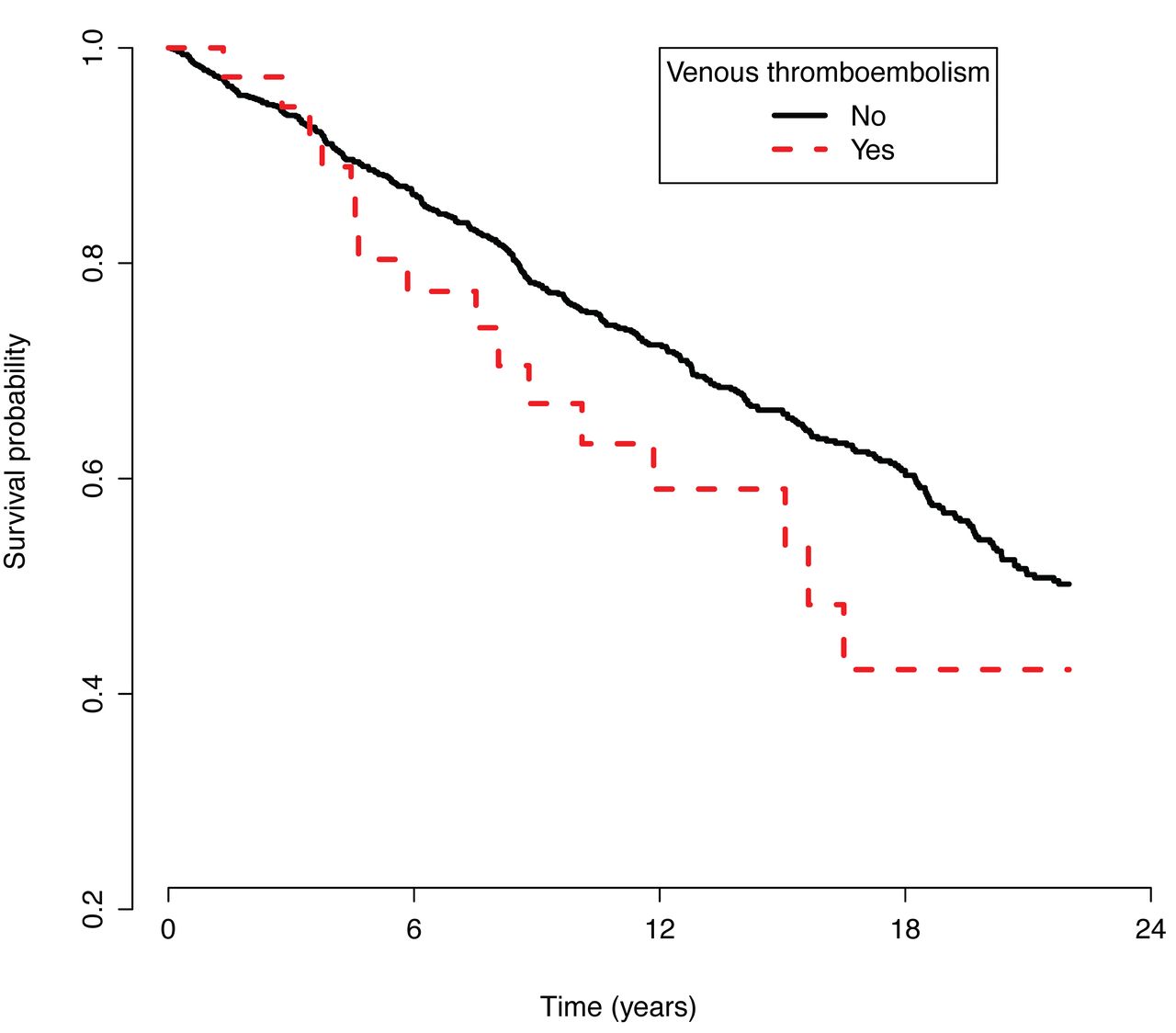
Kaplan-Meier survival curves of subjects with systemic sclerosis, with and without venous thromboembolism (log-rank test, p = 0.54).
DISCUSSION
Vascular abnormalities in SSc including microvascular changes, endothelial dysfunction, impaired angiogenesis, thrombotic arteriopathy, platelet activation, and increased aggregability provide a plausible biologic rationale for the development of VTE in SSc5,17. It has been suggested that SSc is an underrecognized risk factor for VTE, but the evidence to support this is limited1. The cumulative incidence of VTE in SSc of 2.7 per 1000 patient-years in our study is comparable to the VTE cumulative incidence of 3.13% (95% CI 1.73–4.52%) reported in a 2014 metaanalysis1. However, we found the cumulative incidence is not significantly higher than observed in the general population16. This suggests that unlike other rheumatologic disease such as rheumatoid arthritis and systemic lupus erythematosus, SSc is not an independent risk factor for VTE.
Classic risk factors of VTE including immobility, surgery, obesity, and malignancy have been well documented16. In SSc, it has been hypothesized that the diffuse cutaneous subtype may be more predisposed to VTE, because diffuse SSc is associated with elevated plasma D-dimer levels, conferring a possible prothrombotic state3. We found no significant differences in the incidence of DVT or PE between the subtypes, suggesting both subtypes are at equal risk of VTE. We found that the presence of PAH, peripheral arterial disease, Scl-70, and aCL were independent risk factors for VTE in SSc. That is, these risk factors (and the other baseline characteristics we evaluated) occurred prior to the occurrence of VTE. This may have implications in the evaluation of patients with SSc-PAH presenting with worsening dyspnea, because our data suggest that PAH is a risk factor for VTE in SSc.
We found that SSc-ILD subjects more frequently experienced DVT. This is consistent with the observation that individuals with idiopathic pulmonary fibrosis have higher incidence rates of DVT18. The development of DVT in subjects with SSc-ILD may be attributable to immobility. Although infrequent, aCL can occur in the setting of SSc and are associated with thrombosis19. Together, these observations suggest that SSc does not independently confer a venous hypercoagulable state. Rather, when VTE occurs in SSc, one should consider other attributable causes.
Finally, we found no difference in short-term survival between SSc subjects with and without VTE. This may address the fact that there is treatment for VTE and it is effective. However, the survival curves suggested worsening longterm survival for SSc subjects with VTE. ILD and PAH remained independent predictors of mortality.
To our knowledge, this is the first study with primary data collection to evaluate the epidemiology of VTE in SSc in the outpatient setting using a large, well-characterized SSc cohort. We evaluated the effect of VTE on survival using robust mortality data with a long followup duration10,13. A potential limitation is that VTE may have occurred in subjects that were lost to followup and not detected in our study. This may result in our underestimation of the prevalence. Another potential limitation to our work is that we report only symptomatic VTE, because investigations for VTE were based on symptoms and/or signs. We did not systematically screen all asymptomatic subjects or ascertain risk prior to investigation. Although this may result in our underestimation of the rate of VTE in SSc, this reflects real-world practice. The population-based estimates of VTE, with which we compare our findings, used the same screening approach16.
The discordance between our findings and the previously published works may have occurred for a few reasons. It is worth noting that the other Canadian administrative data study involved a distinct population from ours (province of British Columbia vs Ontario). None of the subjects with VTE in our study were taking oral contraceptive or hormone replacement therapy, nor did they have a previous history of DVT or surgery prior to the VTE event. We were not able to adjust for immobility, but this may be colinear with advanced ILD or PAH. In our study, there was no significant difference in the occurrence of cancer between those with and without VTE events.
VTE is an infrequent but important occurrence in SSc. Improving our understanding about the burden and causes of VTE in SSc has the potential to prevent and reduce morbidity and mortality from VTE16.
Footnotes
Dr. Johnson is supported by a Canadian Institutes of Health Research Clinician Scientist Award, the Oscar and Eleanor Markovitz Fund for Scleroderma Research, and the Freda Fejer Fund of the Arthritis Research Foundation. Dr. Wijeysundera is supported in part by a New Investigator Award from the Canadian Institutes of Health Research and a Merit Award from the Department of Anesthesia at the University of Toronto.
- Accepted for publication December 14, 2017.








{kind=link}