

Abstract
Objective. To assess clinical outcomes including imaging findings on computed tomography (CT), pulmonary function testing (PFT), and glucocorticoid (GC) use in patients with the antisynthetase syndrome (AS) and interstitial lung disease (ILD) treated with rituximab (RTX).
Methods. We retrospectively identified all patients at 2 institutions with AS-ILD who were treated with RTX. Baseline demographics, PFT, and chest CT were assessed before and after RTX. Two radiologists independently evaluated CT using a standardized scoring system.
Results. Twenty-five subjects at the Brigham and Women’s Hospital (n = 13) and University of Pittsburgh Medical Center (n = 12) were included. Antisynthetase antibodies were identified in all patients (16 Jo1, 6 PL-12, 3 PL-7). In 21 cases (84%), the principal indication for RTX use was recurrent or progressive ILD, owing to failure of other agents. Comparing pre- and post-RTX pulmonary variables at 12 months, CT score and forced vital capacity were stable or improved in 88% and 79% of subjects, respectively. Total lung capacity (%) increased from 56 ± 13 to 64 ± 13 and GC dose decreased from 18 ± 9 to 12 ± 12 mg/day. Although DLCO (%) declined slightly at 1 year, it increased from 42 ± 17 to 70 ± 20 at 3 years. The most common imaging patterns on CT were nonspecific interstitial pneumonia (NSIP; n = 13) and usual interstitial pneumonia/fibrotic NSIP (n = 5), of which 5 had concurrent elements of cryptogenic organizing pneumonia.
Conclusion. Stability or improvement in pulmonary function or severity of ILD on CT was seen in most patients. Use of RTX was well tolerated in the majority of patients. RTX may play a therapeutic role in patients with AS-ILD, and further clinical investigation is warranted.
The antisynthetase syndrome (AS) is rare and characterized by myositis associated with antisynthetase antibodies, including, but not limited to, anti-Jo1, –PL-7 (threonyl), –PL-12 (alanyl), –OJ (isoleucyl), and –EJ (glycyl), as well as additional clinical features including polyarthritis, fever, Raynaud phenomenon, mechanic’s hands, and interstitial lung disease (ILD)1,2. ILD is the most serious complication of AS (AS-ILD), occurring in 70–89% of patients, with an increase in morbidity and mortality in affected individuals3,4,5,6,7,8. Some variability in ILD incidence, phenotype, and mortality has been noted based on antibody subtype7,8,9. It is imperative to establish effective treatment options for this serious complication. To date, many therapies have been reported for ILD, with glucocorticoids (GC) remaining as the first line of treatment3,5,10. Because of the lack of prospective trials, specific use of additional immunosuppressive agents is empiric.
Rituximab (RTX) is a chimeric monoclonal antibody against CD20+ B cells, which results in B cell depletion11,12. Evidence for the effectiveness of B cell depletion exists in a number of immune-mediated conditions, including rheumatoid arthritis, antineutrophil cytoplasmic antibody-associated vasculitis, and immune thrombocytopenic purpura13,14,15,16,17,18. RTX has also been specifically studied in myositis19,20,21,22,23,24 and scleroderma-ILD25,26. Of note, a retrospective analysis of 50 patients with severe ILD of varying etiologies, excluding idiopathic pulmonary fibrosis (IPF), demonstrated an improvement in pulmonary function tests (PFT) at 6 and 12 months post-RTX27. The only randomized trial of RTX therapy in AS was nested within a double-blind, placebo-phase trial of RTX in 200 refractory adult and juvenile dermatomyositis and adult polymyositis cases by Oddis, et al, in which 17% of subjects possessed antisynthetase autoantibodies (primarily anti-Jo1)19. In the Oddis, et al prospective trial, 83% of subjects met the predetermined definition of improvement after RTX, but no subgroup analysis was performed and lung function and computed tomography (CT) changes were not assessed as an outcome in the antisynthetase-positive subjects. There are limited data regarding the use of RTX in AS-ILD, mostly derived from retrospective case series/case reports, in which improvements in pulmonary function and high-resolution CT (HRCT) scans were noted20,21,28–36. Adverse events mainly included infectious complications, such as P. jirovecii pneumonia, which were occasionally fatal, as well as rash, arrhythmia, and serum sickness21,30,31,33,34,37.
Our objective was to assess clinical outcomes, including pulmonary function, severity of ILD on HRCT, and concurrent GC dosing in a cohort of patients with AS-ILD treated with RTX at 2 institutions.
MATERIALS AND METHODS
Study design and population
We retrospectively identified all patients at the Brigham and Women’s Hospital (BWH), Boston, Massachusetts, USA, and the University of Pittsburgh Medical Center (UPMC), Pittsburgh, Pennsylvania, USA, with antisynthetase autoantibodies who presented with ILD and were treated with RTX since 2007 (BWH) and 2005 (UPMC). Inclusion criteria comprised the presence of antisynthetase autoantibodies, a diagnosis of ILD, treatment with RTX, and ≥ 1 PFT and/or CT scan at baseline and again 1–3 years after treatment with RTX. Exclusion criteria included lack of adequate followup or lung transplantation prior to 1 year after administration of RTX. Demographic characteristics, antisynthetase autoantibodies, clinical symptoms, laboratory abnormalities, concomitant GC (i.e., prednisone dose), and other immunosuppressive use, PFT, and HRCT chest imaging findings were extracted from the electronic medical record through April 2016. At BWH, RTX was routinely dosed every 6 months after the initial administration of RTX, whereas at UPMC, RTX was given initially with variable intervals of subsequent administration in the AS-ILD subjects.
Antisynthetase antibody detection
The majority of antisynthetase antibodies were detected using the Myositis Profile available through the Oklahoma Medical Research Foundation Clinical Immunology Laboratory (n = 21), which included testing for 12 myositis-specific and myositis-associated antibodies using RNA immunoprecipitation. Testing on the other 4 subjects was performed through a variety of other laboratories. Anti-SSA was measured using standard chemiluminescent immunoassay–certified laboratories at both institutions.
Pulmonary function testing
Serial PFT completed primarily for clinical indications were reviewed. For consistency, only prebronchodilator values were used for the analyses because bronchodilator therapy was not routinely given. Reference values for spirometry were derived from the Third National Health and Nutrition Examination Survey in the United States38, whereas lung volumes were standardized using predicted equations based on Crapo, et al39, and DLCO-predicted equations were based on Cotes, et al40.
HRCT analysis
Chest CT scans were done at the 2 study sites using standard institutional CT protocols (including axial HRCT images) as clinically indicated. Two radiologists (RM and FC, with 8 and 2 years’ experience, respectively, as thoracic radiologists) independently evaluated axial 3–5 mm chest CT scans and 1 mm HRCT scans, recording their subjective assessment of the ILD pattern as usual interstitial pneumonia (UIP), nonspecific interstitial pneumonia (NSIP), or cryptogenic organizing pneumonia (COP). Coexistence of ≥ 1 CT pattern was possible and was also recorded. This was followed by a more detailed quantitative assessment and calculation of a CT severity score (Supplementary Table 1, available from the authors on request). The thin-section CT findings were graded on a scale of 1–6 as shown in Supplementary Table 1. Presence of each of the 6 different types of imaging patterns was assessed independently in 3 (upper, middle, and lower) zones of each lung. The upper zone was defined as the area above the level of the carina, the middle zone as the area between the level of the carina and the level of inferior pulmonary vein, and the lower zone as the area below the level of inferior pulmonary vein. The extent of each abnormality was determined by visually estimating the percentage (to the nearest 5%) of the affected lung parenchyma in each zone. The abnormality score for each zone was calculated by multiplying the percentage area by the point value (the score of 1–6)41,42. The score for each zone was calculated by multiplying the percentage of the area to the nearest 5% by the grading scale score. The 6 zone scores were averaged to determine the total score for each patient. The scores of the 2 observers were averaged.
Statistical analysis
Chest CT scan scores, PFT, and prednisone dose were assessed before and after RTX. Average values were calculated at baseline for all subjects with followup values at any timepoint (1, 2, or 3 yrs), and average values at subsequent timepoints were calculated only for subjects with baseline values for comparison. An improvement in CT severity scores was defined as a > 10% decrease, while improvement in PFT was defined as a > 10% increase in forced vital capacity (FVC). Failure is defined by a > 10% increase in CT score or a > 10% decline in FVC. Stability was defined as between these values — a < 10% decrease but < 10% increase in CT score and a < 10% increase but < 10% decrease in FVC43. Paired univariate analyses were conducted with Wilcoxon signed-rank tests where appropriate. Subgroup analyses were based on antisynthetase autoantibodies, ILD pattern, baseline mean HRCT score (194), PFT variables indicating severe disease [FVC < 50%, total lung capacity (TLC) < 50%, and DLCO < 35%; some of which have been associated with increased ILD mortality44,45], use of RTX as initial or rescue therapy, and the presence of concurrent immunosuppression at the time of starting RTX. A p value of < 0.05 was considered statistically significant. All analyses were performed using Statistical Analysis Software version 9.3 (SAS Institute). This project was granted IRB approval by the Partners Human Research Committee at BWH (protocol no. 2014P000110) and UPMC (IRB0409097).
RESULTS
At BWH, 16 consecutive patients treated with RTX for AS-ILD since 2007 were identified. One proceeded to lung transplant 2 months after RTX and was excluded, while 2 additional patients were excluded because of lack of PFT or HRCT followup. There were no deaths recorded in the medical record. At UPMC, 21 consecutive patients with AS-ILD treated with RTX since 2005 were identified. Eight were excluded because of lack of followup PFT and/or HRCT data, 1 of whom died from respiratory failure 5 months after receiving RTX; 1 additional subject proceeded to lung transplant 10 months after RTX and was also excluded. Two UPMC subjects included in our study also died: 1 from respiratory failure secondary to progression of underlying ILD 2 years after receiving RTX (Supplementary Table 2, UPMC Subject 4, available from the authors on request), and 1 from anoxic brain injury about 10 years after receiving RTX (Supplementary Table 2, UPMC Subject 6). Available baseline and followup HRCT and PFT for each BWH and UPMC subject are detailed in Table 1.
Available baseline and followup CT and PFT for each BWH and UPMC subject.
Of the 25 subjects included in our cohort, the mean age was 49 years, and 20 (80%) were female (Table 2). Eight patients (32%) had a smoking history and 2 (8%) were current smokers. Antisynthetase antibodies were identified in all patients (16 Jo1, 6 PL-12, 3 PL-7). Four subjects were anti-SSA–positive, 15 were negative, and for 6 the information was unavailable. The most common clinical features noted at any time in the clinical course included myositis (n = 19) and Raynaud phenomenon (n = 14), followed by mechanic’s hands/rashes/arthritis (n = 12 each), and fever (n = 6). Baseline HRCT (n = 21) revealed the following patterns: 9 NSIP, 4 UIP/fibrotic NSIP, 4 NSIP/COP, 1 COP, 1 fibrotic NSIP/COP, 1 COP/bronchiolitis obliterans, and 1 acute interstitial pneumonitis (AIP)/diffuse alveolar damage (Figure 1). Abnormalities of the esophagus identified on HRCT included a patulous esophagus (n = 7) and hiatal hernia (n = 1). The Spearman rank correlation coefficient for quantitative CT scoring interobserver agreement between the 2 radiologists was 0.95.
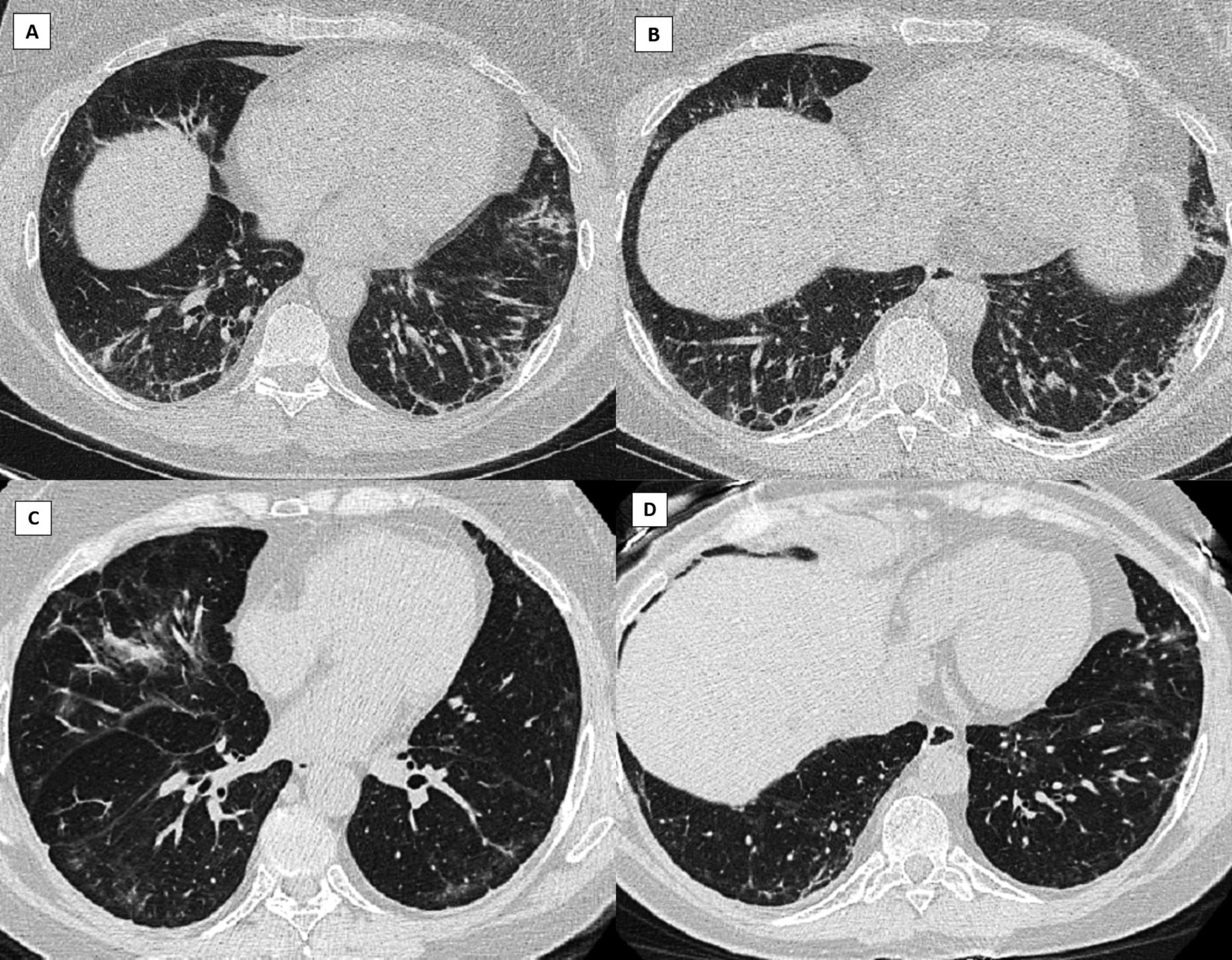
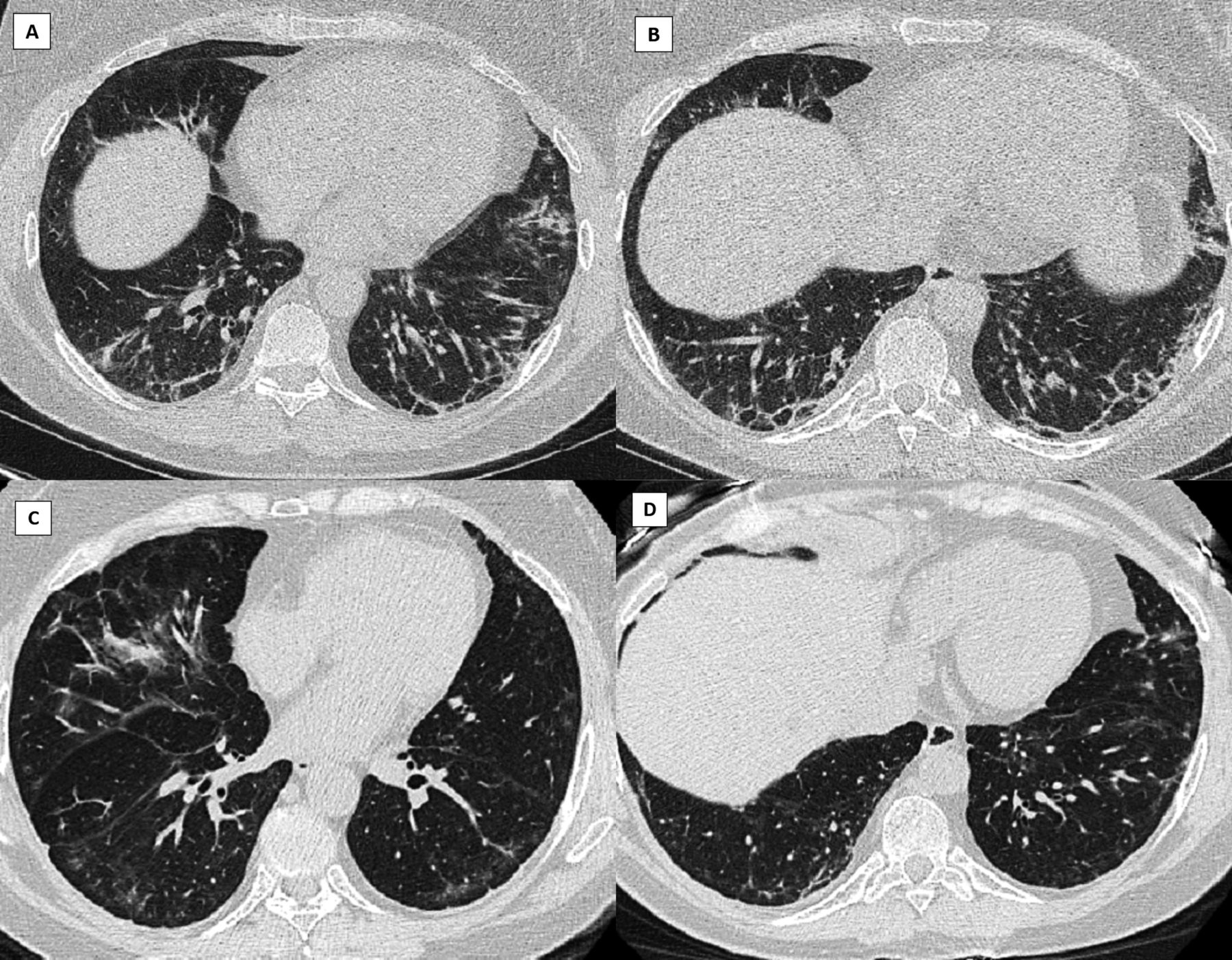
CT scan before and after treatment with RTX for BWH Subject 2. Pre-RTX (CT score 125.1): axial HRCT images in lung windows (A and B) demonstrate subpleural reticulation, coarse linear bands, ground-glass abnormality, and patchy consolidation within the lower lobes, lingula, and right middle lobe in a predominantly peripheral, subpleural distribution. Affected areas of lung demonstrate traction bronchiectasis and architectural distortion. No honeycombing was present, and lung volumes were mildly reduced. Pattern of interstitial pneumonitis has overlapping features of both NSIP and COP. More than 3 years post-RTX (CT score 113.7): axial HRCT images (C and D) in lung windows demonstrate definite improvement in bilateral subpleural reticulation, consolidation, and architectural distortion. Residual ground-glass opacity is present with subpleural sparing, and imaging features are consistent with a milder NSIP pattern. CT: computed tomography; RTX: rituximab; BWH: Brigham and Women’s Hospital; HRCT: high-resolution CT; NSIP: nonspecific interstitial pneumonia; COP: cryptogenic organizing pneumonia.
Baseline demographics of AS subjects. Values are n (%) or mean ± SD.
The diagnosis of AS followed the diagnosis of ILD in 18 patients (72%) by a mean of 2.5 years. The mean time to initiation of RTX after ILD identification was 4.4 years. In 21 cases (84%), the principal indication for RTX use was recurrent or progressive ILD owing to failure of other immunosuppressive agents. In 4 subjects (16%), RTX was used as the first GC-sparing agent. Medications used prior to switching to RTX are detailed in Table 1. Twenty-three subjects were taking prednisone at the time of starting RTX (92%) and 12 (48%) were taking additional concurrent immunosuppressive agents at the time of starting RTX: mycophenolate mofetil (MMF; n = 7), tacrolimus and MMF (n = 1), azathioprine (n = 1), cyclophosphamide (n = 1), intravenous immunoglobulin (n = 1), and methotrexate (n = 1). Three patients had documented adverse events after the initial RTX dosing: 1 anaphylaxis and 2 serious gastrointestinal complications requiring surgery; they all later resumed RTX. Infectious complications while taking RTX included pneumonia (n = 1), influenza (n = 1), bronchitis (n = 1), Clostridium difficile colitis/urinary tract infection (n = 1), diverticulitis (n = 1), varicella zoster (n = 2), cellulitis (n = 1), and sinus infection (n = 1).
We compared the baseline and 1-year post RTX findings in the 21 subjects with either PFT and/or HRCT imaging at 1 year of followup and then analyzed subjects with up to 3-year PFT (n = 7) and/or HRCT (n = 4) followup (Table 3, Figure 2; and Supplementary Table 2, available from the authors on request). The average CT scan score at 1 year (n = 8) was stable or improved in 88% of subjects while the FVC (n = 19) was similarly stable or improved in 79%. The average TLC in all subjects (n = 7) increased from 56 ± 13 to 64 ± 13 at 1 year, with a statistically significant average individual TLC increase of 8.3% (p = 0.016). Similar trends were seen at 24 months. Based on very limited 36-month followup data for only 7 subjects, there was a statistically significant average individual increase in FVC at 3 years of 21% (p = 0.016). Although the average DLCO in all subjects declined slightly from 42 ± 17 to 36 ± 16 at the 1-year timepoint, there was an increase at 2 years to an average of 53 ± 26. The GC dose was stable or decreased in 88% of subjects at 1 year with an average drop of 6 mg and a statistically significant average individual decrease of 6.2 mg (p = 0.041). When comparing subjects who received repeat RTX dosing (n = 17) with those who received a 1-time dose (n = 8), those with repeat RTX dosing showed improvement in all variables, including a significant average increase in FVC and TLC of 9.3% (p = 0.0077) and 8.5% (p = 0.031), respectively (Table 4), despite starting with a lower average FVC, TLC, and DLCO, although a comparison of baseline values between the 2 groups did not reach statistical significance. Those who received a single dose of RTX had a decline in most variables including a worsening CT score, decrease in FVC, and decrease in DLCO, although the numbers were too small to reach statistical significance. Overall, 100% of subjects (5/5) who had repeat RTX dosing had treatment success (defined as stabilization or improvement) regarding CT score, and 93% (13/14) had treatment success regarding FVC. In the single RTX group, those numbers declined to 67% (2/3) for CT score and 40% (2/5) for FVC (Table 4).

Graph of (A) CT score, and (B) FVC by subject over 3 years of followup. (A) Line graph of CT scores demonstrating stability or improvement (decrease in CT score) in > 75% of subjects over the 3 years of followup. (B) Line graph of FVC demonstrating stability or improvement in > 79% of subjects over the 3 years of followup. CT: computed tomography; FVC%: forced vital capacity, % predicted; BWH: Brigham and Women’s Hospital; UPMC: University of Pittsburgh Medical Center.
Comparison of pre- and post-RTX CT scan score, PFT measurements, and prednisone dose for all subjects with followup at 1–3 years (n = 25). Values are mean ± SD or n (%) unless otherwise specified.
Comparison of pre- and post-RTX CT scan score and PFT measurements comparing averages at baseline and 1 year with the average individual change (p value) in subjects with repeat RTX dosing versus subjects with a 1-time RTX dose. Values are mean ± SD or n (%) unless otherwise specified.
Although limited in their interpretability given the insufficient numbers, we did perform subgroup analyses by autoantibody status (Jo1, PL-12, PL-7), radiographic pattern (NSIP, NSIP, and COP, or fibrotic ILD), severity of lung disease (CT fibrosis score > or < 194, FVC < or > 50%, TLC < or > 50%, DLCO < or > 35%), use of RTX as rescue therapy or initial therapy, and absence or presence of concurrent immunosuppression at the time of initiating RTX (Supplementary Table 3, available from the authors on request). Improvement with RTX was more apparent in individuals who had an NSIP pattern on CT scan, or had less severe lung disease based on the FVC or DLCO. Those in whom RTX was started owing to failure of other immunosuppressive agents and those who were taking concurrent immunosuppression also had a more notable response. However, small subject numbers limited the generalizability of the above findings and prohibited paired statistical analyses in many subgroups.
DISCUSSION
In our study of 25 AS-ILD subjects treated with RTX at 2 academic referral centers, we observed stability or improvement in CT imaging and/or physiologic testing (FVC, TLC, and DLCO) in most patients at 1 and 3 years of followup. Further, there was a significant steroid-sparing effect and RTX was generally well tolerated. Subgroup analyses demonstrated a benefit to repeat RTX dosing over a single RTX cycle, but in general, it seemed that the greatest benefit to RTX was seen at the 3-year followup, although the low number of patients with data at this endpoint limits the generalizability of the conclusions.
Previous studies addressing RTX for treatment of AS-ILD have also shown a favorable response20,21,28–34,36, although investigations are mostly limited to case reports and retrospective studies. In small case series of patients with AS-ILD following treatment with RTX, objective improvement in PFT (FVC, TLC, and DLCO) has been noted20,21,28,30,33,34,35,36, as has improvement or resolution of ground-glass opacities and stability, or improvement of fibrosis on HRCT20,28,30,33,35. In 1 similar retrospective study by Andersson, et al, ILD extent was found to be reduced or stabilized in 21/23 patients and FVC increased by an average of 24% in 24 patients followed longitudinally for up to 60 months33. In another small study by Marie, et al35 of 7 AS subjects with refractory ILD treated with RTX at Day 0, Day 14, and Month 6, there was a statistically significant improvement in the median FVC/DLCO and an improvement (n = 5) or stability (n = 2) in HRCT at 1 year of followup, as well as a decrease or resolution of respiratory symptoms in all subjects. Further, these subjects had a significant decrease in the concurrent median daily prednisone dose from 20 mg/day to 9 mg/day35. However, unlike our study, this was a single-center study that did not assess individual change and had insufficient power to analyze subgroups. There has been 1 prospective trial by Allenbach, et al, in which 10 antisynthetase-positive subjects who had failed conventional treatment received RTX at Day 0, Day 15, and Month 631. That study demonstrated an improvement or stabilization of ILD as measured by FVC and DLCO in 9/10 subjects and either a > 50% decrease in steroid dose or discontinuation of ≥ 1 other immunomodulatory/immunosuppressive drug in 6/10 patients. Only 1 subject had a reduction in interstitial infiltrates on CT scan, and improvement in ILD (5/10 subjects) was defined as a 10% increase in FVC or 15% increase in DLCO, while stabilization (4/10 subjects) was defined as a < 10% decrease in FVC or < 15% decrease in DLCO at Month 12.
Although our study and previous case series and retrospective studies have reported favorable responses in AS-ILD treated with RTX, the mechanism of its therapeutic effect is uncertain. It is unclear whether the B cell–deleting mechanism attributed to RTX represents the mechanism of action leading to its effectiveness in AS-ILD. Studies in other immune-mediated diseases suggest that RTX may lead to normalization of autoreactive T cells46,47, and the repopulation of the B cells following RTX may be antigenically naive, transitional B cells, suggesting a possible “resetting” of the immune system that contributes to a therapeutic effect48. A retrospective study of 50 systemic autoimmune rheumatic disease–related ILD patients with myositis improved their PFT following B cell depletion27, suggesting a key pathogenic role of T cells in myositis-ILD. Future mechanistic studies should address the pathogenic potential of specific antibodies in AS and whether B cell depletion after RTX is responsible for its favorable effect in AS-ILD. In addition, the future elucidation of antisynthetase autoantibody-specific differences or whether the presence of other biomarkers is useful in predicting a response to B cell depletion should be investigated to guide treatment algorithms in AS-ILD.
In our study, all patients in the BWH cohort received repeat RTX dosing on average every 6 months, whereas most patients in the UPMC cohort received only a 1-time dose (n = 8), with only 4 receiving repeat dosing at variable intervals. A better objective response in FVC and TLC was noted in patients with repeat RTX dosing, with a trend toward improved HRCT scores. However, the sample size is too small to draw any significant conclusions and there may be inherent bias because the reason for redosing in the UPMC cohort could not be ascertained. This raises the question of whether those subjects who were redosed were the patients who responded favorably, while those who were not redosed did not respond to initial RTX dosing. In general, there is no standard of care regarding the frequency of RTX dosing in myositis given the paucity of data and the variability of third-party payer approval. One retrospective study demonstrated that in 11 AS patients with severe, progressive ILD refractory to other immunotherapy, RTX appeared to stabilize and/or improve ILD in 7 patients during the first 6 months only28, suggesting that frequent dosing versus 1-time RTX dosing was more effective. This observation, our findings, especially the significant improvement at 3 years, and the pathophysiologic mechanisms discussed above suggest that optimal RTX dosing may require additional dosing rather than an initial cycle of RTX, and that RTX may take a long time to have an effect.
Our study has a few important limitations. First, the small sample size limits the discovery of statistically significant findings, particularly regarding the interpretability of subgroup analyses. Second, the retrospective chart review design is limited in that not all subjects have data at all timepoints, and there are very few subjects with 3-year followup, potentially introducing a source of bias. However, all subjects had ≥ 1 HRCT or PFT done > 1 year from the time of initial RTX dosing. To address this limitation, the difference in the mean of paired observations was presented to allow for paired analyses. Third, there was variability in the dosing of RTX at the 2 independent centers, which complicates composite data analyses. Fourth, there is limited generalizability given that our study was conducted in 2 clinical centers. Fifth, there is an inherent difficulty in assessing radiographic outcomes in ILD associated with AS, because there is no validated specific scoring system for autoimmune ILD. Although numerous HRCT severity scoring systems exist for evaluation of patients with IPF, no specific scoring system has yet been proposed for patients with ILD in the setting of AS. Given the presence of multiple radiologic patterns (UIP, NSIP, and COP) in this subset of patients, we adapted a CT scoring system proposed by Fujimoto, et al41 and Ichikado, et al42, which has previously been used for quantitative assessment of HRCT abnormalities in a variety of clinical scenarios ranging from AIP, acute respiratory distress syndrome, and IPF6. The exclusion of the UPMC subject who proceeded to transplant after 10 months might have biased the data analysis in favor of RTX, given that this subject received a lung transplant after declining over the 10 months after RTX. Additional prospective, randomized, multicenter trials should address these limitations.
RTX may play a therapeutic role in patients with AS-ILD. Our study has added a significant body of data to the existing information on RTX in AS-ILD, and suggests that further clinical investigation is warranted into the effectiveness of RTX as a treatment for AS-ILD, pathophysiologic mechanisms of action, ideal dosing interval, and length of treatment4.
Footnotes
Supported by the US National Institutes of Health (grant number 1 K23 HL119558 to TJD).
- Accepted for publication November 15, 2017.








{kind=link}
{kind=link}