

Abstract
Objective. To assess the prevalence and association of renal dysfunction in patients with spondyloarthritis (SpA).
Methods. The ASAS-COMOSPA (Assessment of Spondyloarthritis international Society-COMOrbidities in SPondyloArthritis) was an international study (22 participating countries from 4 continents) investigating comorbidities in SpA. Renal function was assessed based on estimated glomerular filtration rate (eGFR) calculated using the Modification of Diet in Renal Disease equation. SpA characteristics and risk factors for renal impairment were collected. Nonsteroidal antiinflammatory drug (NSAID) use was assessed based on current intake (last 3 mos).
Results. Of the 3984 patients recruited, 2098 (52.6%) were analyzed after excluding outliers and patients with no available eGFR measurement [male sex: 63.5%; age: 45.3 yrs; disease duration: 8.6 years; HLA-B27+: 73.1%; Bath Ankylosing Spondylitis Activity Index (BASDAI): 3.6/10]. Overall, 153 patients (5.2%, mean age: 53.6 yrs) exhibited an eGFR < 60 ml/min/1.73 m2. In univariate analysis, renal impairment was associated with age (p < 0.001), HLA-B27 positivity (p = 0.003), several cardiovascular (CV) risk factors (history of hypertension, p < 0.001; systolic blood pressure, p = 0.009; diabetes, p = 0.005; and Framingham risk score, p < 0.001), disease activity scores [BASDAI, p = 0.001; Ankylosing Spondylitis Disease Activity Score-C-reactive protein (ASDAS-CRP), p < 0.001], functional variables (Bath Ankylosing Spondylitis Functional Index, p < 0.001), inflammatory biomarkers (erythrocyte and CRP, both p < 0.001), and NSAID intake since onset of disease (percentage of days, p = 0.008). However, there was no association with disease duration, disease severity, or ASAS-NSAID score. In multivariate analysis, age (45–59 yrs: OR 1.9, > 60 yrs: OR 6.2), HLA-B27 positivity (OR 0.51), and CRP (OR 1.3) remained significantly associated with eGFR < 60 ml/min/1.73 m2.
Conclusion. Renal impairment was associated with age, HLA-B27 positivity, and inflammation, though not with CV risk factors, disease severity, or NSAID intake in patients with SpA.
- SPONDYLOARTHRITIS
- RENAL IMPAIRMENT
- CARDIOVASCULAR RISK FACTORS
- ANKYLOSING SPONDYLITIS
- CHRONIC KIDNEY DISEASE
- NSAID
Spondyloarthritis (SpA) is a chronic inflammatory disease primarily involving the spine and sacroiliac joint. The condition manifests as back pain and progressive stiffness of the spine. The peripheral joints and entheses (capsules, ligaments, and tendons) can also be involved1, in addition to several other organ systems, and several epidemiological studies have found higher incidences of extraarticular manifestations1.
Renal involvement in SpA, although uncommon, may include secondary renal amyloidosis (AA type), nonsteroidal antiinflammatory drug (NSAID) nephropathy, glomerulonephritis1, and, more rarely, nephrolithiasis2. The few data that exist concerning the prevalence of renal impairment in SpA mostly originate from small or retrospective studies1,2,3,4,5,6,7,8. Amyloidosis is more prevalent in aggressive and active SpA and older patients with longstanding disease4. A Finnish hospital-based study of ankylosing spondylitis (AS) patients with a mean followup time of 25 years reported an overall mortality rate 1.5-times higher than expected, attributed to the high incidence of deaths from AS, primarily due to AA amyloidosis4.
NSAID are the cornerstones of AS treatment, yet are known to cause adverse renal events, such as acute tubular necrosis and interstitial nephritis, as well as hypertension (HTN). In cases of NSAID failure, anti-tumor necrosis factor-α (TNF-α) treatment is required. Several case reports suggest that TNF inhibitors could improve AA amyloidosis9.
Several studies have shown that patients with SpA are at higher risk for cardiovascular (CV) disease and vascular mortality10. This could be because of a TNF-α-mediated inflammatory process, as well as SpA treatment, with NSAID potentially causing or exacerbating HTN while increasing the thrombogenic risk. Further, patients with SpA are even more likely than the general population to experience renal impairment influenced by CV risk factors.
The objective of our study was to assess the prevalence of renal impairment in patients with SpA according to the large international ASAS-COMOSPA (Assessment of Spondyloarthritis international Society-COMOrbidities in SPondylo-Arthritis) cohort, and to identify the risk factors of renal impairment.
MATERIALS AND METHODS
The ASAS-COMOSPA was an international, cross-sectional study of consecutive SpA patients followed up in routine care11. Rheumatologists from 22 participating countries across 4 continents included 3984 adult patients fulfilling ASAS criteria for the diagnosis of peripheral or axial SpA.
Clinical variables were recorded (age, sex, disease duration, HLA-B27 positivity, history of joint replacement, and extraarticular manifestations). Biological values recorded were C-reactive protein (CRP; mg/dl), erythrocyte sedimentation rate (ESR; mm in the first hour), CV risk factors [HTN, diabetes, smoking, high-density lipoprotein (HDL) and low-density lipoprotein (LDL) cholesterol, obesity based on body mass index (BMI), and Framingham risk score calculation12], and SpA activity scores [Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), and Ankylosing Spondylitis Disease Activity Score (ASDAS)]. Functional scores recorded were Bath Ankylosing Spondylitis Functional Index (BASFI) and EQ-5D13. BASDAI has been considered as a continuous variable and a categorical variable with < or ≥ 4/10 as a threshold for inactive or active disease. NSAID use was based on current intake (last 3 mos), percentage of days intake since onset, and calculation of the ASAS-NSAID score14. Proteinuria, hematuria, and leukocyturia were not collected in this cohort. SpA severity was assessed by history of hip replacement and presence of bamboo spine.
Estimated glomerular filtration rate (eGFR) in ml/min/1.73 m2 was calculated using the simplified Modification of Diet in Renal Disease (MDRD) equation. Values of eGFR < 60 ml/min/1.73 m2 defined renal impairment15.
The study was conducted according to guidelines for good clinical practice in all countries. Written informed consent was obtained from all subjects before enrollment. All local ethics committees (North East-Newcastle/North Tyneside 2 Research Ethics committee 12/Ne/0417, the 14th/12/2012) approved the ASAS-COMOSPA study protocol.
Statistical analysis
Statistical analysis was performed using Stata software, Version 12 (StataCorp). The tests were 2-sided, with a Type I error set at α = 0.05. Means and SD or medians and interquartile ranges were calculated for continuous variables, and number of patients and associated percentages for categorical variables. Comparisons between independent groups (eGFR < or ≥ 60 ml/min/1.73 m2) were performed using the chi-squared or Fisher’s exact test for categorical variables, and Student t test or the Mann-Whitney U test were applied for quantitative variables (normality verified by the Shapiro-Wilk test, with homoscedasticity tested by the F distribution). Multivariate analyses (logistic regression model with eGFR < or ≥ 60 ml/min/1.73 m2 as dependent variable) were conducted to establish risk factors in the following procedure: first, stepwise (backward and forward) on the factors considered significant in univariate analysis (entry in the model for p < 0.1)16,17, and second, according to clinically relevant variables18,19 (SpA duration, HLA-B27 positivity). The interactions between factors were also tested. The results were expressed as OR with 95% CI. Multivariate analyses were performed using random-effects models to take into account center effect. A sensitivity analysis was performed to compare characteristics (age, sex, Framingham CV risk, BMI, BASDAI) of patients excluded because of missing data or outliers and complete cases.
RESULTS
Of the 3984 patients with SpA included in the study, 2098 (52.6%) had available data enabling eGFR calculation using the MDRD equation. The characteristics of patients excluded because of missing data or outliers did not differ from those of the study population, except for age (45.3 ± 13.7 in the study population vs 41.8 ± 14 yrs in the excluded population).
The demographic characteristics of the study population are presented in Table 1.
Comparative analysis of demographic, SpA-related characteristics, CV risk factors, and disease activity variables according to eGFR in patients with SpA. Values are n (%) unless otherwise specified.
In the study population, mean age was 45.3 ± 13.7 years, the majority were male (n = 1332, 63.5%), mean SpA duration was 8.6 ± 9 years, and HLA-B27 was positive in 73.1% (n = 1126). Sacroiliitis manifested on radiograph in 1315 patients (62.8%) and on magnetic resonance imaging in 558 (26.6%). Extraarticular manifestations of SpA (psoriasis, uveitis, or inflammatory bowel disease) were present in 488 patients (23.3%) and bamboo spine in 166 (8%). History of hip replacement was reported in 81 patients (4%).
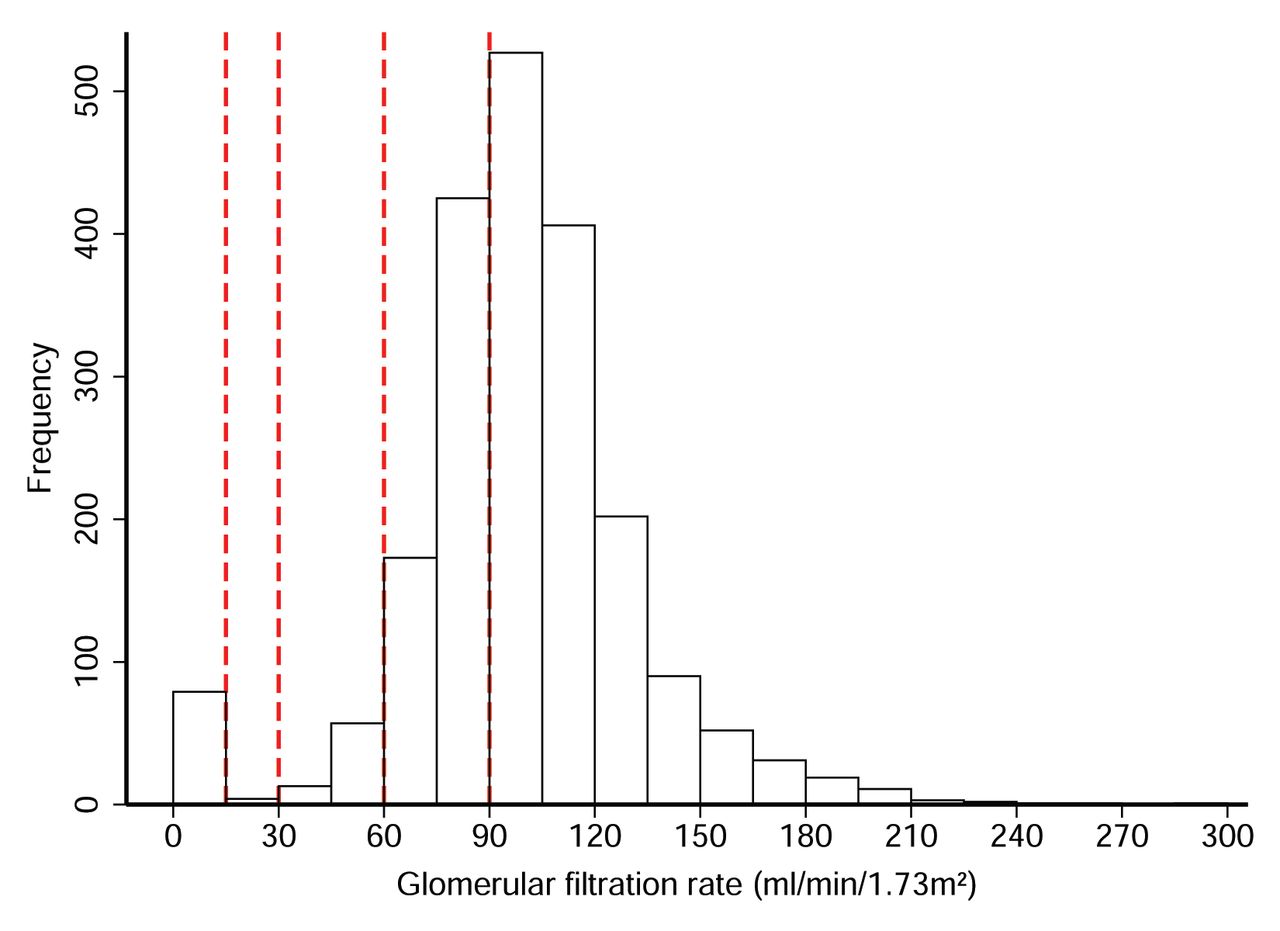
A total of 153 patients (5.2%) presented an eGFR < 60 ml/min/1.73 m2, with a mean age of 53.6 ± 14.6 years. The distribution of GFR is presented in Figure 1.
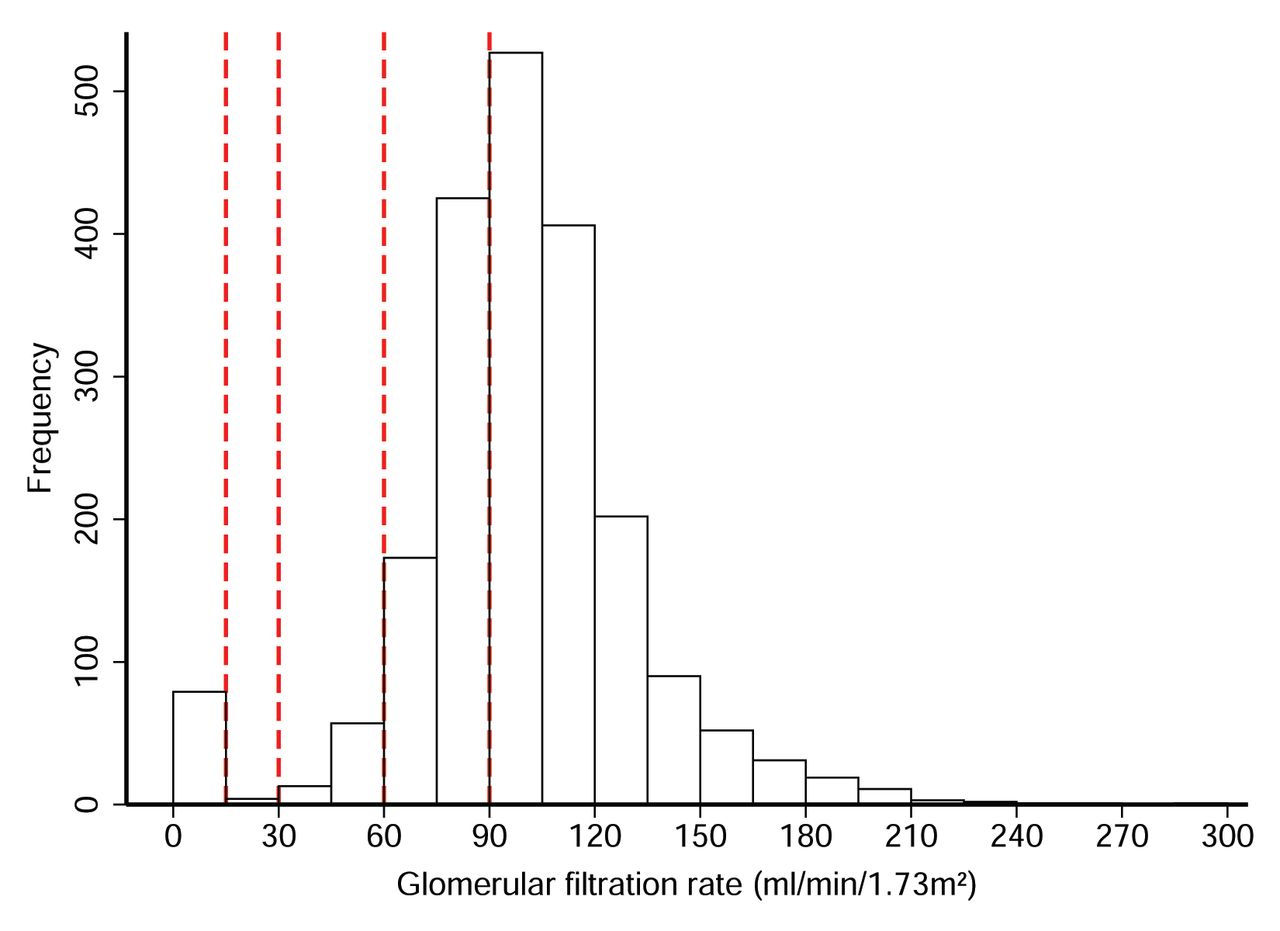
Distribution of the GFR. GFR is expressed in ml/min/1.73 m2 as calculated with the MDRD equation. The red lines separated the different categories of eGFR: 15 ml/min/1.73 m2, 30 ml/min/1.73 m2, 60 ml/min/1.73 m2, and 90 ml/min/1.73 m2. GFR: glomerular filtration rate; eGFR: estimated GFR; MDRD: Modification of Diet in Renal Disease.
Only 3 patients had amyloidosis, and all had an eGFR > 60 ml/min/1.73 m2.
Association between renal impairment and demographic characteristics of SpA
Renal impairment was strongly associated with age (53.6 ± 14.6 vs 44.6 ± 13.3 yrs, p < 0.001) and HLA-B27 positivity (59.6% vs 74%, p = 0.003), but not with sex or disease duration. Patients with renal impairment were older at the time of the SpA diagnosis (43.7 ± 14.8 vs 36.1 ± 12.9 yrs, p < 0.001).
Association between renal impairment and CV risk factors
HTN was more frequently reported in patients with an eGFR < 60 ml/min/1.73 m2 (50.3% vs 34.8%, p <0.001) and with diabetes mellitus (18.3% vs 10.8%, p = 0.005). Systolic blood pressure was higher in patients with renal impairment (127.6 ± 16.8 mmHg vs 123.9 ± 15.5 mmHg, p = 0.009), while diastolic blood pressure was similar in all. The Framingham risk score was higher in cases of renal impairment (12.8 ± 10.2 vs 7.9 ± 7.9, p < 0.001).
In addition, there was no significant difference in the prevalence of previous or current smoking, HDL cholesterol level, LDL cholesterol level, or BMI between patients with or without renal impairment.
Association between renal impairment and SpA activity
Patients with renal impairment had higher SpA activity scores: BASDAI (4.1 ± 2.4 vs 3.5 ± 2.4, p = 0.001), ASDAS-ESR (2.8 ± 1.1 vs 2.3 ± 1.1, p < 0.001), ASDAS-CRP (2.4 ± 1.1 vs 1.9 ± 1.1, p < 0.001), and physician’s global assessment (PGA; 3.7 ± 2.1 vs 3.1 ± 2, p < 0.001)
The acute-phase reactant levels were also higher in those with an eGFR < 60 ml/min/1.73 m2: ESR [22 (6–24) vs 12 (5–23) mm at the 1st hour, p < 0.001] and CRP [0.2 (0.05–1.2) vs 0.1 (0.03–0.3) mg/dl, p < 0.001].
Association between renal and functional impairment
Patients with renal impairment exhibited worse functional variables: BASFI (4.4 ± 2.6 vs 2.9 ± 2.7, p < 0.001), and EQ-5D (0.39 ± 0.31 vs 0.59 ± 0.31, p < 0.001).
Association between renal impairment and SpA severity
No significant association was reported between history of hip replacement or presence of bamboo spine and renal dysfunction.
Association between renal impairment and SpA treatment
There was no relationship between reduced renal function and the type of current disease-modifying antirheumatic drug given (anti-TNF or methotrexate). There were 257 patients (12.3%) receiving daily corticosteroid therapy, with a cumulative dose of 8034 mg, without any association with renal impairment.
There were 1429 patients (68.3%) who had taken NSAID at least once in the 3 previous months, with no differences between the groups. Patients with renal impairment received less NSAID since onset of the disease than patients with eGFR > 60 ml/min/1.73 m2 (51% vs 58.4% of days NSAID intake, p = 0.008). NSAID score was similar between patients with and without renal impairment (7.5 vs 12.6, p = 0.18)
Multivariate analysis
Two logistic regression models, one with BASDAI as a continuous variable (model A) and one with BASDAI as a categorical variable (< or ≥ 4/10, Model B) were constructed from the variables significantly associated with eGFR < 60 ml/min/1.73 m2. Other variables, which were not significant on univariate analysis although they could have been confounding or clinically relevant, were included in the model: sex and TNF-α blocker treatment. In both models, the intraclass correlation coefficient was relatively high (0.40).
In model A, these factors remained significantly associated with eGFR < 60 ml/min/1.73 m2: age (between 45–59 yrs: OR 2, 95% CI 1.1–3.6; > 60 yrs: OR 6.5, 95% CI 2.9.7–14.6), HLA-B27 positivity (OR 0.54, 95% CI 0.3–0.97), CRP (OR 1.3, 95% CI 1.1–1.5), and BASDAI (OR 1.2, 95% CI 1.05–1.27).
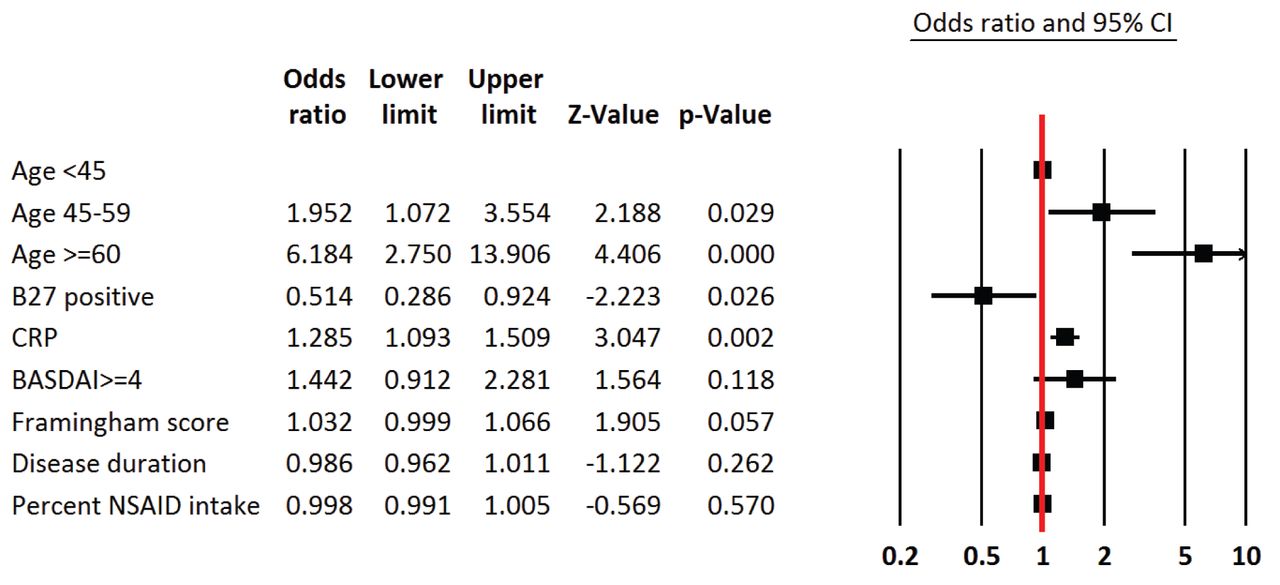
In model B, these factors remained significantly associated with eGFR < 60 ml/min/1.73 m2: age (between 45–59 yrs: OR 1.9, 95% CI 1.1–3.6; > 60 yrs: OR 6.2, 95% CI 2.7–13.9), HLA-B27 positivity (OR 0.51, 95% CI 0.29–0.92), and CRP (OR 1.3, 95% CI 1.1–1.5).
Forest plot of the variables associated with renal impairment after multivariate analysis with BASDAI as a categorical variable (Model B) is presented in Figure 2.

Forest plot of the variables associated with renal impairment (eGFR < 60 ml/min/m2). Black squares correspond to the OR while the horizontal bars represent the 95% CI. eGFR: estimated glomerular filtration rate; CRP: C-reactive protein; BASDAI: Bath Ankylosing Spondylitis Activity Index; NSAID: nonsteroidal antiinflammatory drug.
DISCUSSION
In the international ASAS-COMOSPA study, 5.2% of patients with SpA exhibited renal impairment, as defined by an MDRD-based eGFR < 60 ml/min/1.73 m2. ASAS-COMOSPA was the first and largest observational study to assess comorbidities, particularly renal impairment, in a worldwide population of patients with SpA11. The prevalence of renal impairment in our study was in line with that reported in the literature: El Maghraoui stated that renal abnormalities [including glomerulonephritis, particularly associated with deposition of immunoglobulin A (IgA) and containing immune complexes, renal amyloid deposition, microscopic hematuria, microalbuminuria, and decreased renal function and creatinine clearance] are observed in 10% to 35% of patients with AS3. In the largest SpA study so far, though retrospective in design, 8% of the 681 patients with SpA exhibited proteinuria and/or hematuria1. In a retrospective insurance–based Canadian study with 2 comparative cohorts (patients with SpA and the general population), the prevalence of any “renal complications” was estimated at 3.4% in men and 2.1% in women with SpA5. In the large population-based study conducted by Haroon, et al, chronic kidney disease was reported in 1.7% of the patients with SpA and in 0.7% of the matched controls10. In a Brazilian retrospective study including 1472 patients with various subtypes of SpA (AS, psoriatic arthritis, undifferentiated arthritis, reactive arthritis), 17 patients (1.2%) had renal involvement (IgA nephropathy or chronic hematuria) without data on their GFR20. The discrepancies with the results observed in our study could be explained by its design, with the inclusion of consecutive patients, a possible overestimation of renal dysfunction prevalence in the retrospective studies, and the definition of renal impairment used.
In our study, renal impairment was associated with age, HLA-B27 positivity, and CRP. In patients with SpA, the risk of renal dysfunction exists even at a young age, and is higher than in the whole age-adjusted population. In the retrospective insurance-based cohort reported by Levy, et al, comparing 8616 patients with axial SpA to 50,699 healthy sex- and aged-matched subjects from the general population, the magnitude of the risk of renal complications (acute or chronic kidney disease, amyloidosis, hypertensive kidney disease) was highest among younger individuals and decreased with age (prevalence ratio of any renal diagnosis: 2.4 in AS men aged 20 to 39 yrs vs 2 in those aged 40 to 59 yrs)5.
In both of our multivariate analysis models, HLA-B27 positivity seemed to be negatively associated with renal impairment (Appendix 1). To our knowledge, this association has never been reported before and links between the HLA-B27 gene and renal damage are poorly studied. In the studies of Lee, et al and Azevedo, et al, frequency of proteinuria and hematuria was similar in HLA-B27–positive or –negative patients1,21.
Disease activity scores (BASDAI, ASDAS-ESR, ASDAS-CRP, PGA) and acute-phase reactants were strongly associated with renal impairment in univariate analysis, but only CRP level remained significantly associated with renal impairment. However, the low absolute values found for CRP limit the significance. The main hypothesis held that chronic inflammation promoted atherosclerosis. Inflammatory mediators such as CRP or interleukin 6 have already been reported to be predictive of CV morbidity and mortality, especially in patients receiving dialysis22. Renal impairment was revealed to be a strong independent CV risk factor in the general population23. Several studies have shown that patients with SpA are at high risk of CV disease24,25,26,27,28,29, with ischemic heart disease and myocardial infarction occurring at a higher rate in these individuals30,31. In our study, renal impairment was associated with CV risk factors only in univariate analysis.
In our study, renal impairment was not associated with SpA severity (as assessed by hip replacement or presence of a bamboo spine) or with disease duration. It has been previously reported that longstanding disease with chronic inflammation could lead to the deposit of serum amyloid A protein, in turn leading to amyloidosis (AA type) as an important cause of death (12%) in longterm followup4. In our study, only a few patients (n = 3) were reported to have amyloidosis. This could be explained by the type of recruitment, large and prospective, with all levels of severity of SpA.
Our study naturally has several limits including, first, the large quantity of missing data for the estimation of GFR. However, comparison of patients excluded because of missing data or outliers with those of the study population revealed no significant differences except for age. Second, the data on hematuria and leukocyturia, which are also markers of kidney damage, were not collected, nor were variables pertaining to the definition of chronic kidney disease according to the National Kidney Foundation15. Proteinuria, typically the most common presentation of amyloidosis, was also not recorded. The multicentric design of the study, based on the cooperation of numerous different countries, posed a difficulty when attempting to sample urine in standardized conditions.
Renal impairment is not rare in SpA and is associated with age, HLA-B27 positivity, and inflammation, though not with SpA severity or CV risk factors. Systematic estimation of GFR is necessary for patients with SpA, notably those treated by nephrotoxic therapies such as NSAID.
APPENDIX 1.
Multivariate analysis of the variables associated with renal impairment (eGFR < 60 ml/min/1.73 m2).
- Accepted for publication November 21, 2017.








{kind=link}
{kind=link}