

Abstract
Objective. Exclusion of psoriatic skin/nail lesions is important in differentiating early seronegative rheumatoid arthritis (ERA) from early polyarticular psoriatic arthritis (EPsA) and such manifestations may go unnoticed in atypical or minimally expressed cases. The aim of this study is to assess the usefulness of integrated rheumatological-dermatological evaluation in highlighting dermatological lesions missed on rheumatological examination and to investigate the role of ultrasonography (US) and dermoscopy in improving the recognition of subclinical psoriatic findings.
Methods. Patients with a new diagnosis of seropositive or seronegative ERA and EPsA with prevalent hands involvement were recruited. All were reassessed for the presence of psoriatic lesions during an integrated rheumatological-dermatological clinical evaluation and underwent hands US and proximal nailfold dermoscopy.
Results. Seventy-three consecutive subjects were included in the study: 25 with seropositive ERA, 23 with seronegative ERA, and 25 with EPsA. One-fourth of the subjects initially diagnosed as seronegative ERA presented cutaneous or nail psoriasis on integrated rheumatological-dermatological evaluation, thereby being reclassified as EPsA. The presence of at least 1 extrasynovial feature on hand US and dotted vessels on proximal nailfold dermoscopy was significantly associated with EPsA, with a sensitivity of 68.0% and 96.0% and a specificity of 88.1% and 83.3% for US and dermoscopy, respectively. When used together, specificity for PsA diagnosis raised to 90.5%.
Conclusion. Integrated rheumatological-dermatological clinical evaluation may be helpful in identifying patients with EPsA misclassified as seronegative ERA. Additionally, US and dermoscopy may be used as supportive tools in identifying subclinical psoriatic features, which may come in handy in distinguishing EPsA from ERA.
- INTEGRATED RHEUMATOLOGY-DERMATOLOGY ASSESSMENT
- DERMOSCOPY
- IMAGING
- PSORIATIC ARTHRITIS
- RHEUMATOID ARTHRITIS
- SERONEGATIVE RHEUMATOID ARTHRITIS
Diagnosis of early seronegative rheumatoid arthritis (RA) may be challenging, with consequent possible diagnostic mistakes and inappropriate therapies. This is likely due to the absence of specific markers for seronegative RA (e.g., biological and imaging diagnostic markers), as well as the greater difficulty in classification of RA in early phases1. The main differential diagnosis of seronegative forms of early RA (ERA) is early polyarticular psoriatic arthritis (PsA), whose recognition is also troublesome, especially when dealing with minimal or atypical cutaneous or nail lesions, because they may be difficult to recognize. In this regard, we highlighted the usefulness of both proximal nailfold dermoscopy and musculoskeletal ultrasonography (US) as possible supportive tools in highlighting peculiar subclinical features and assisting the diagnosis of early PsA (EPsA)2,3. In particular, dermoscopy revealed diffuse reddish background (with or without sparse dotted vessels) of proximal nailfold, while US displayed extrasynovial and synovio-entheseal complex (SEC) involvement (i.e., peritendinitis, enthesitis, and soft tissue edema)2,3.
In our study, we carried out an integrated rheumatological-dermatological clinical assessment along with dermoscopic and US examinations of patients with arthritis with prevalent involvement of the hands diagnosed as having seronegative ERA by expert rheumatologists, comparing their findings with those of patients with seropositive ERA and EPsA with hand small joint involvement. The aim was to investigate the usefulness of a shared diagnostic approach, including an integrated clinical assessment in conjunction with dermoscopic and US evaluations, in the differential diagnosis between seronegative ERA and EPsA with rheumatoid-like joint involvement.
MATERIALS AND METHODS
Consecutive patients with a new diagnosis of ERA (< 12 mos from symptoms onset) or EPsA (< 24 mos from symptoms onset) referred by expert rheumatologists to the outpatient Early Arthritis Clinic of the University Hospital of Udine (Italy) were screened for this cross-sectional case-control analysis4,5. The study duration was 1 year, from November 2015 to November 2016. Inclusion criteria were (1) fulfillment of the American College of Rheumatology (ACR)/European League Against Rheumatism (EULAR) 2010 classification criteria for ERA cases and a score ≥ 2 of ClASsification for Psoriatic ARthritis criteria (CASPAR) for patients with EPsA1,5,6; and (2) clinical presentation with arthritis of hand small joints (excluding the rare cases of RA with distal interphalangeal joint involvement) for both EPsA and ERA groups. Subjects were not included if they had used systemic steroid therapy or conventional/biological disease-modifying antirheumatic drugs (DMARD) during the previous 3 months or concomitantly had hand osteoarthritis, chondrocalcinosis, or other rheumatological diseases involving the hands. Additionally, ERA subjects with a family history of psoriasis in first- or second-degree relatives or current/past evidence of skin/nail psoriasis were also excluded.
All the patients underwent hand US, dermoscopic examination of proximal nailfold vascular pattern, and integrated dermatological-rheumatological clinical assessment within 7 days from the initial referral. Traditional hand and feet radiographs were also concomitantly done in all the subjects. The study was carried out according to a protocol for the characterization of early arthritis approved by the local Ethical Committee (protocol EAC001-number 66/2015/OS-CEUR), in conformity with the Declaration of Helsinki and the guidelines for good clinical practice. Informed consent was obtained from all the participants.
US protocol
Longitudinal and transverse US examinations of both hands [metacarpophalangeal (MCP) joints, proximal interphalangeal (PIP) joints, flexor and extensor finger tendons, dorsal and volar soft tissue] were performed by the same rheumatologist (AZ), blinded to clinical and laboratory data, using a MyLabClassC (Esaote) equipped with a 6–18 MHz linear transducer with specific attention not to apply transducer pressure on the anatomical structures under examination. US greyscale imaging variables were optimized for maximal image resolution and power Doppler settings were standardized at the following values: 750 Hz for pulse repetition frequency, 3 for wall filter, 4 for persistence, and color gain between 50–55%. According to our previous study, only the more specific US features for PsA were evaluated, i.e., peritendon inflammation of the extensor digitorum tendon (PTI) at MCP joint, central slip enthesitis (CSE) at PIP joint, and soft tissue edema around flexor tendon (STE-FT)3,7,8. STE-FT was defined as a diffuse enlargement of soft tissue round the flexor tendon, with an increased power Doppler signal, from finger pad to MCP joint, and it was evaluated by volar scan3,9,10. Further, erosions, defined as discontinuity of bone surface that is visible in 2 perpendicular planes, were evaluated at MCP and PIP joints11.
Dermoscopic examination protocol
Dermoscopic assessment of vascular morphology of proximal nailfold of a target finger (i.e., that one with the best visibility of the vascular pattern) was performed by the same dermatologist having a demonstrated experience in the field of dermoscopy (EE) using a polarized, manual dermoscope (DermLite DL3 X10, 3 Gen). A fluid interface (US gel) was placed between the instrument and the skin to enhance vessel visibility; minimal pressure was applied to preserve vessels morphology and ensure their better visualization. Dermoscopic evaluation was done prior to the dermatological clinical assessment and the examiner was unaware of dermatological and rheumatological clinical data as well as US findings. According to our previous dermoscopic analysis2, reddish background with or without dotted vessels was considered as “psoriatic pattern,” while “fish school-like” vessels and irregular/ramified, blurry, purple vessels were considered “non-psoriatic pattern”; detection of a single row of uniform capillary loops just above the cuticle was considered “normal pattern” (Supplementary Figure 1, available with the online version of this article).
Integrated dermatological-rheumatological clinical assessment
Dermatological and rheumatological clinical evaluations [always performed by the same dermatologist (EE) and rheumatologist (AZ), respectively] were done during a single medical examination after US and dermoscopic examination (Figure 1). Rheumatological assessment was carried out by articular examination recording tenderness and swelling of the joints, while dermatological assessment consisted of inspecting all the skin surface and nail plate of all fingers to detect skin/nail psoriatic lesions. In all cases, skin lesions diagnosed as “psoriatic” underwent dermoscopic examination (using a polarized device) to confirm the clinical diagnosis by detecting specific validated dermoscopic findings, i.e., diffusely distributed dotted vessels and white scaling12,13,14,15.

Flow chart of the study protocol. RA: rheumatoid arthritis; PsA: psoriatic arthritis; ACR: American College of Rheumatology; EULAR: European League Against Rheumatism; CASPAR: ClASsification for Psoriatic ARthritis criteria.
Statistical analysis
All analyses were performed using Microsoft Excel 2010 (Microsoft Corp.). Data are expressed as mean or absolute values or percentages. The study has an analytical design, and then it was not powered. Comparative evaluation of the prevalence of dermoscopic and US findings in the 3 groups was carried out using Fisher’s exact test, with statistical significance set at p < 0.05, without corrections for multiple comparisons. Further, for each PsA feature, sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were calculated by considering patients with early RA (both seropositive and seronegative) as the control group.
RESULTS
A total of 73 consecutive subjects were included in the study: 23 (3 men and 20 women, mean age: 54.2 ± 14.7 yrs) with seronegative ERA, 25 (12 men and 13 women, mean age: 54.0 ± 16.5 yrs) with seropositive ERA, and 25 (14 men and 11 women, mean age: 52.4 ± 9.3 yrs) with EPsA. Nineteen out of 25 (76.0%) seropositive RA patients were positive for both rheumatoid factor (RF) and anticitrullinated protein antibodies (ACPA), while 22 out of 25 patients with PsA (88.0%) had current psoriasis and 23 of them (92.0%) had a CASPAR score ≥ 3. Clinical features of the 3 groups are showed in Table 1. Standard radiographs did not allow us to differentiate EPsA from both seronegative and seropositive ERA in any case (not significant evidence of juxtaarticular new bone formation).
Clinical findings at the first rheumatological evaluation.
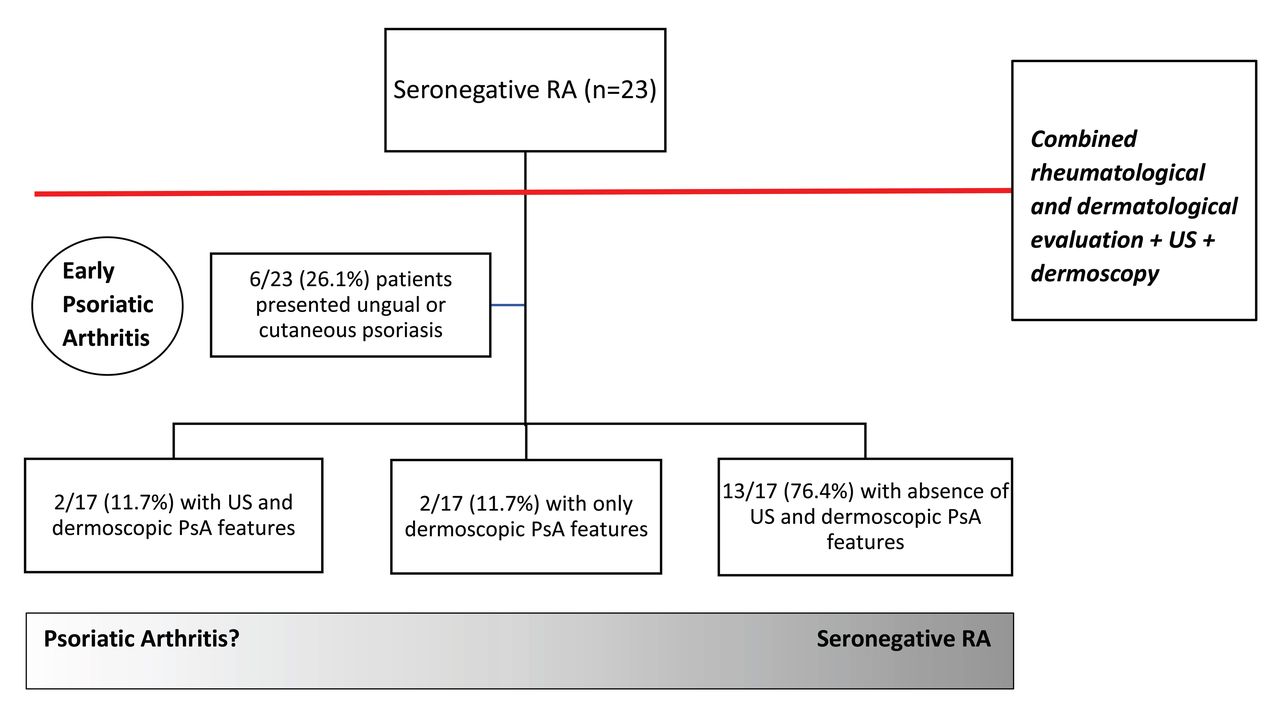
Six out of 23 patients (26.1%) in the cohort of seronegative ERA presented cutaneous or nail psoriasis (previously unrecognized) on dermatological evaluation during the jointed rheumatological-dermatological visit (Figure 2). In detail, 4 out of 6 subjects had very limited and mild skin psoriatic lesions (Psoriasis Area and Severity Index < 3 in all cases — localization: elbows 4/4 and heels 1/4), which were confirmed by dermoscopy, while the remaining 2 patients presented only nail psoriatic changes, i.e., nongeometric pitting, psoriatic onycholysis, oil drop patches, and punctate leukonychia. All such patients also presented the same dermoscopic vascular periungual pattern detected in all EPsA subjects (Supplementary Figure 2, available with the online version of this article), and 4 out of 6 also had PsA-specific features on US examination of the hands (Supplementary Figure 3, available with the online version of this article). Of note, none of these 6 patients had radiologic evidence of juxtaarticular new bone formation. Consequently, the initial (at the first referral) diagnosis of seronegative ERA was finally changed into EPsA in these 6 patients after the integrated rheumatology-dermatology evaluation.
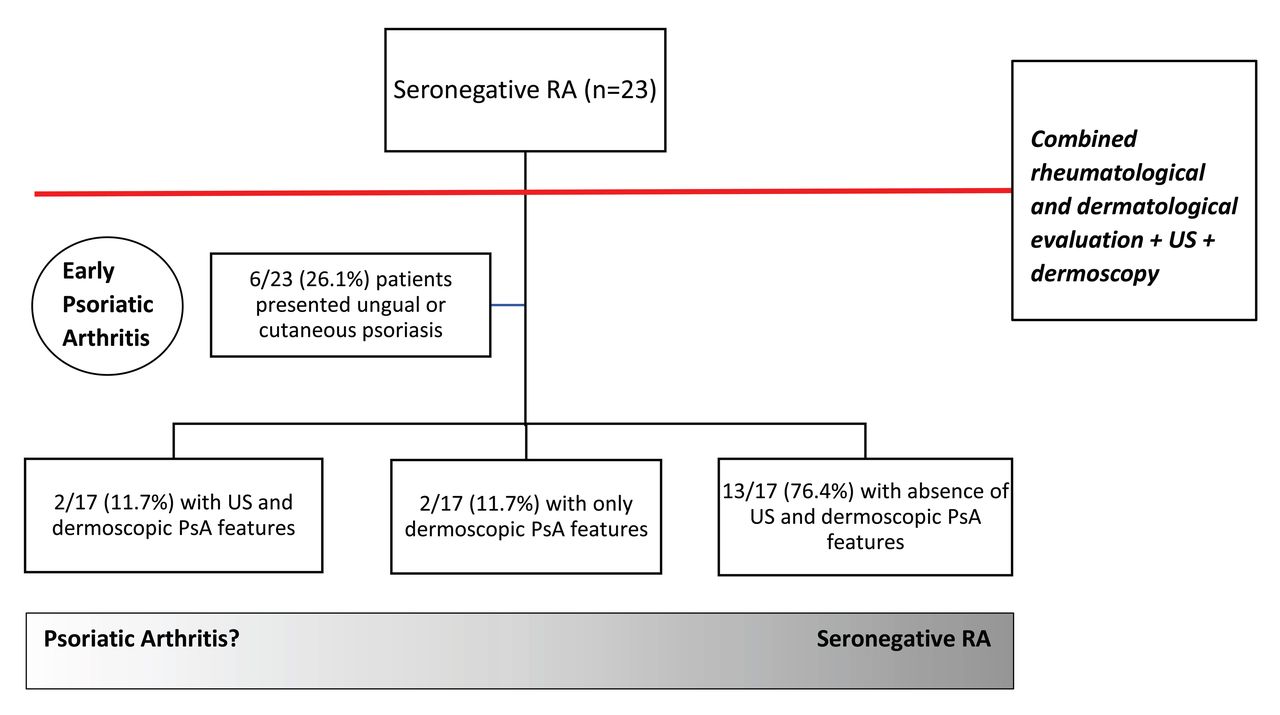
Diagnostic algorithm of seronegative RA. RA: rheumatoid arthritis; PsA: psoriatic arthritis; US: ultrasonography.
In the comparative analysis of the 3 cohorts (EPsA, seropositive ERA, and seronegative ERA without the 6 patients with the new diagnosis of psoriasis), 96.0% (24/25) of patients with EPsA presented sparse or diffuse dotted vessels over a reddish/pinkish background (“psoriatic pattern”) on dermoscopic assessment of proximal nailfold, while such a pattern was observed only in 4 out of 17 (23.5%) seronegative ERA patients and in 3 out of 25 (12.0%) seropositive ERA patients (p < 0.001 for PsA vs seronegative or seropositive RA); all the other patients with ERA presented a non-psoriatic pattern (Table 2).
US and dermoscopic features of the 3 groups. Values are n (%) unless otherwise specified.
For US features, 17 out of 25 patients with EPsA (68.0%) displayed at least 1 psoriatic-specific finding, while this was detected in 2 out of 17 (11.7%) seronegative ERA subjects (p < 0.001) and in 3 out of 25 (12.0%) seropositive ERA patients (p < 0.001; Table 2). Considering each US psoriatic finding in EPsA cohort, STE-FT, PTI, and CSE were found in 10/25 (40.0%), 9/25 (36.0%), and 5/25 (20.0%) subjects, respectively. Erosions were more frequently found in seropositive ERA (8/25; 32.0%) compared to seronegative ERA (2/17; 11.7%) and EPsA patients (3/25; 12.0%), though there was no statistical significant difference (Table 2).
Of note, the 2 seronegative ERA cases having US features specific for EPsA also had the same dermoscopic vascular periungual pattern observed in all EPsA subjects (i.e., sparse or diffuse dotted vessels over a reddish/pinkish background), despite the absence of psoriatic manifestations on clinical assessment (Figure 2 and Figure 3).
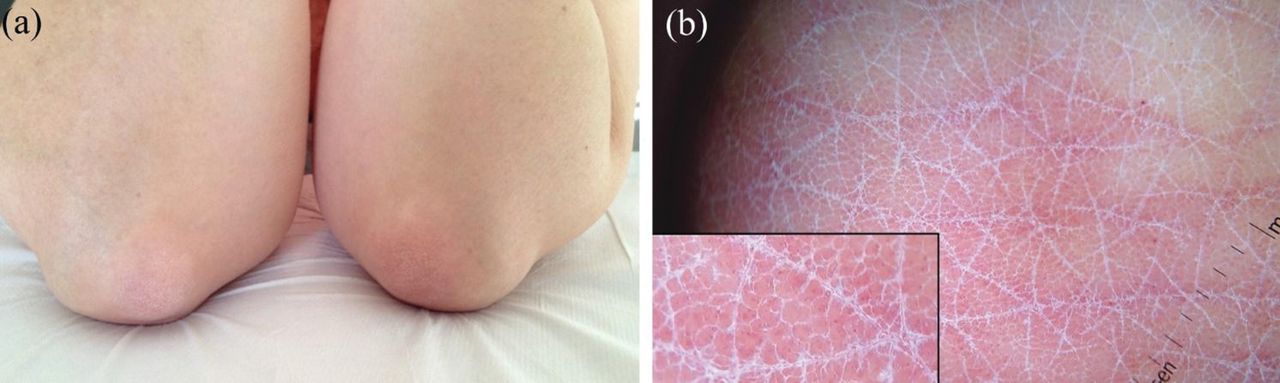
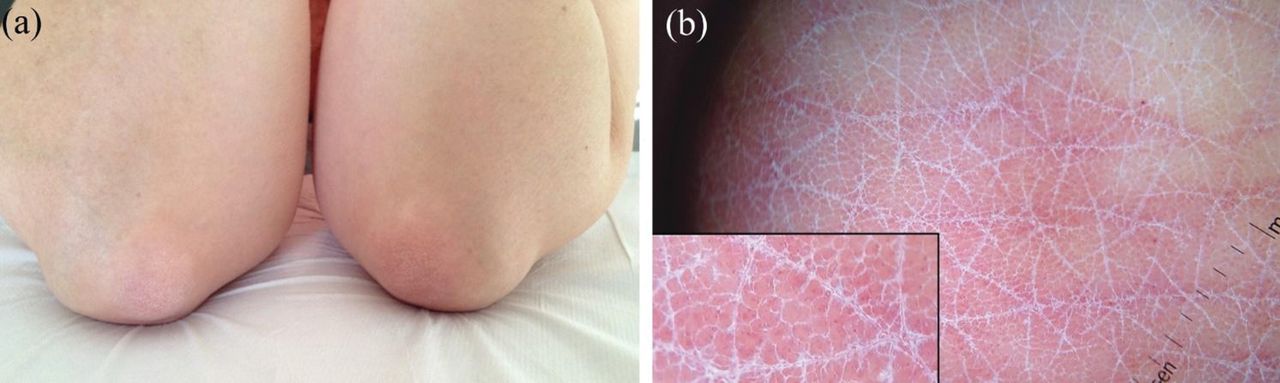
(a) Clinical picture of one of the 6 patients initially diagnosed as having seronegative RA who turned out to have minimal skin psoriatic lesions (on the elbows in this case) on combined rheumatological-dermatological assessment. (b) Dermoscopic examination of the lesions reveals the typical psoriatic pattern: regularly distributed dotted vessels and diffuse white scaling, thus confirming the clinical diagnosis. RA: rheumatoid arthritis.
Considering the accuracy for EPsA of the 2 imaging techniques, dermoscopic detection of dotted vessels had a sensitivity of 96.0% and a specificity of 83.3%, while its PPV and NPV were 77.4% and 97.2%, respectively (Table 3). On the other hand, the detection of at least 1 US feature among PTI pattern at MCP joint, CSE pattern at PIP joint, and STE-FT of the digit turned out to have a sensitivity of 68.0% and a specificity of 88.1% for EPsA, while its PPV and NPV were 77.3% and 82.2%, respectively (Table 3). When integrated, dermoscopy and US displayed a specificity of 90.5% (Table 3).
Sensitivity, specificity, PPV, and NPV of different US and dermoscopic features for early PsA versus early seronegative and seropositive RA.
DISCUSSION
The differential diagnosis between seronegative ERA and EPsA can be difficult in patients with symmetrical polyarthritis of the MCP and PIP joints of the hands because standard radiographs are often unhelpful in early phases and no specific biomarkers are currently available, hence the need of new diagnostic approaches. Our study highlights the role of imaging techniques, i.e., proximal nailfold dermoscopy and US of small joints of the hand, as well as integrated rheumatological-dermatological clinical assessment in facilitating the correct diagnosis of such types of arthritis. This reinforces the view that a strict collaboration between the rheumatologist and the dermatologist is a relevant step toward diagnosis, with potential reduction of misclassifications. This finding could have important implications for management and outcome because an early and correct diagnosis is crucial for choosing the best treatment and getting the greater likelihood to achieve remission, especially when using new therapeutic options such as ustekinumab, secukinumab, and apremilast, which are effective in PsA but not in RA.
Based on our results, about one-fourth of patients diagnosed as having early seronegative RA on rheumatological examination turned out to have minimal cutaneous/nail psoriasis after an integrated rheumatology-dermatology clinical evaluation. This is quite relevant because the detection of dermatological psoriatic disease, along with the absence of RF and ACPA, rules out RA (based on the 2010 ACR/EULAR criteria) and satisfies CASPAR criteria for PsA. Of note, psoriatic lesions in our patients went unnoticed on the first rheumatological assessment because they were very limited, so only the expertise of a dermatologist led to their identification.
Importantly, all the seronegative RA cases reclassified as PsA after integrated rheumatological-dermatological clinical evaluation also showed psoriatic findings on dermoscopic examination of proximal nailfold and 66% of them also displayed PsA features on US assessment, thus emphasizing the usefulness of such tools in assisting the clinical differential diagnosis of early arthritis. This is further supported by the high specificity (90.5%) for EPsA that we observed in the concomitant use of dermoscopy and US.
Regarding US, we found that PsA displayed a more common US extrasynovial and SEC involvement compared to RA, with soft tissue edema (i.e., diffuse enlargement of soft tissue around the flexor tendon or peritendon inflammation of the extensor digitorum tendon) being the most important differentiating finding between the 2 conditions, thus supporting the results observed in our previous work as well as in other studies3,9,10,16,17 (Supplementary Figure 3, available with the online version of this article). On the other hand, we observed that most patients with PsA, clinically active for hands arthritis, presented sparse or diffuse dotted vessels over a reddish/pinkish background on dermoscopic examination of proximal nailfold, while this pattern was seen in only 12% of seropositive RA patients. Such results are slightly different from the ones found in our previous study, in which dotted vessels (having sparse distribution) were seen in 53.3% of cases, while in the remaining patients only a reddish background was evident. These differences are likely due to technical variations in the dermoscopic assessment because, unlike the previous analysis, in this study we used a fluid interface (US gel), which is known to enhance the vessels visibility on dermoscopy. Additionally, we cannot exclude that the different results could also occur because the PsA cohort examined in the previous study did not have cutaneous/nail psoriasis (PsA sine psoriasis), with consequent less expression of skin vascular alterations.
Both soft tissue edema and proximal nailfold vascular changes may be the consequence of a remodeling of blood and lymphatic vasculature in extrasynovial structures due to the endothelial cells’ dysfunction and the consequent increased expression of vascular endothelial growth factor and other vascular mediators, which might be responsible for dilation/proliferation as well as morphological/functional alterations of cutaneous vessels18,19.
In our opinion, the use of imaging techniques could play a more extensive role in the diagnostic investigation of early arthritis because specificity of the CASPAR classification criteria is not absolute, and some patients diagnosed as having seronegative ERA might indeed present EPsA without visible skin/nail lesions. In this regard, excluding subjects with skin/nail psoriatic clinical manifestations, we still found that about 12% of seronegative RA patients showed psoriatic features on both US and dermoscopy, thereby raising questions about the precise classification of these subjects and the need of a medium-term followup to better characterize this subgroup of chronic polyarthritis.
Our study emphasizes that an integrated rheumatological-dermatological clinical evaluation may be helpful in identifying patients with misclassified EPsA as seronegative RA. In particular, US and dermoscopy may be useful tools to distinguish EPsA from ERA, because the former presents both US extrasynovial SEC involvement and a peculiar dermoscopic vascular pattern of the proximal nailfold (dotted vessels). When combined, US and dermoscopy findings demonstrate a high specificity for EPsA. In this way, the diagnostic investigation of early arthritis may be improved, if confirmed in a larger series.
ONLINE SUPPLEMENT
Supplementary material accompanies the online version of this article.
- Accepted for publication November 21, 2017.








{kind=link}
{kind=link}
{kind=link}