

Abstract
Objective. To identify the effects of glucocorticoids (GC) on various types of fractures in patients with rheumatoid arthritis (RA).
Methods. We used the Korean National Healthcare Claims database from 2010 to establish a retrospective cohort of patients with RA ≥ 19 years old. We then followed those patients through December 2013. The incidence rates of total and major fractures were calculated. We evaluated the effects of GC dose and duration on fractures using multivariable logistic regression analyses. We also examined the influence of GC on fractures in RA patients without a history of osteoporosis.
Results. A total of 11,599 fractures was observed in 9964 out of 138,240 patients with RA. During followup, 68.2% of patients used oral GC for > 3 months. Adjusted analysis showed the risk of vertebral fractures was increased by the following characteristics: duration of GC ≥ 6 months (OR 1.76, p < 0.01); mean dose of GC ≥ 2.5 mg (OR range = 1.37–1.71, p < 0.01); and highest daily dose of GC ≥ 10 mg (OR range = 1.23–1.75, p < 0.03). However, neither the duration nor the dose of oral GC increased the risk of hip and nonvertebral/nonhip fractures in patients with RA. Consistent results were observed in RA patients without osteoporosis.
Conclusion. Longer duration and higher dose of oral GC in patients with RA increased the risk of vertebral fractures. However, the dose and duration of GC did not influence the risk of hip and nonvertebral/nonhip fractures.
Patients with rheumatoid arthritis (RA) experience fractures more frequently than those in the general population1,2,3,4,5. This increased risk of fracture is explained by several characteristics of RA and patients with RA. Some researchers have proposed that the inflammatory characteristics of RA, and therefore the elevated expression of proinflammatory cytokines, is associated with osteoporosis and fractures6,7. Others have suggested that common characteristics of patients with RA, including advanced age, female sex, RA medications, decreased physical activity, and combined vitamin D deficiency increase their risk of fracture5.
Among various risk factors for fractures in patients with RA, perhaps the most important factor is the use of glucocorticoids (GC)8,9,10,11,12,13. Low-dose GC are widely used to suppress signs and symptoms of inflammation and retard the development and progression of bone erosion14. By suppressing the expression of proinflammatory cytokines, such as tumor necrosis factor-α, interleukin 1 (IL-1), and IL-6, GC may benefit bone health6,7. On the other hand, GC therapy is the leading cause of secondary osteoporosis15,16,17. GC decrease bone density by decreasing the number of osteoblasts, partially through increasing osteocyte apoptosis, and increasing the number of osteoclasts15. As seen in previous studies, the relative risk of fracture in GC users was 1.5–2.0, according to anatomical site8. However, prior studies have not investigated how the duration of GC use, mean daily dose of GC, or highest daily dose influence the risk of fractures. Therefore, there is some controversy within the research community regarding the effect of GC usage on fractures regarding treatment specifics8,18,19.
The influence of GC on fractures may also differ by involved anatomic site. Prior studies have found that GC therapy has a more profound and rapid effect on trabecular bone mass than it does on cortical bone mass20,21. Bone composition differs according to anatomic site; therefore, the effect of GC on each bone would be expected to vary. However, this site-dependent effect of GC has never been clearly shown and also remains controversial8,19.
Therefore, we sought to identify the specific effects of GC treatment on various fracture types using the Korean healthcare claims database, which includes the entire Korean RA population.
MATERIALS AND METHODS
Data source and study population
We analyzed data from the nationwide claims database of the Health Insurance Review and Assessment Service (HIRA) of Korea, which covers about 98% of the entire Korean population22. The HIRA claims database includes valuable resources for healthcare service research, including patient diagnosis, treatment, procedures, surgical history, and prescriptions.
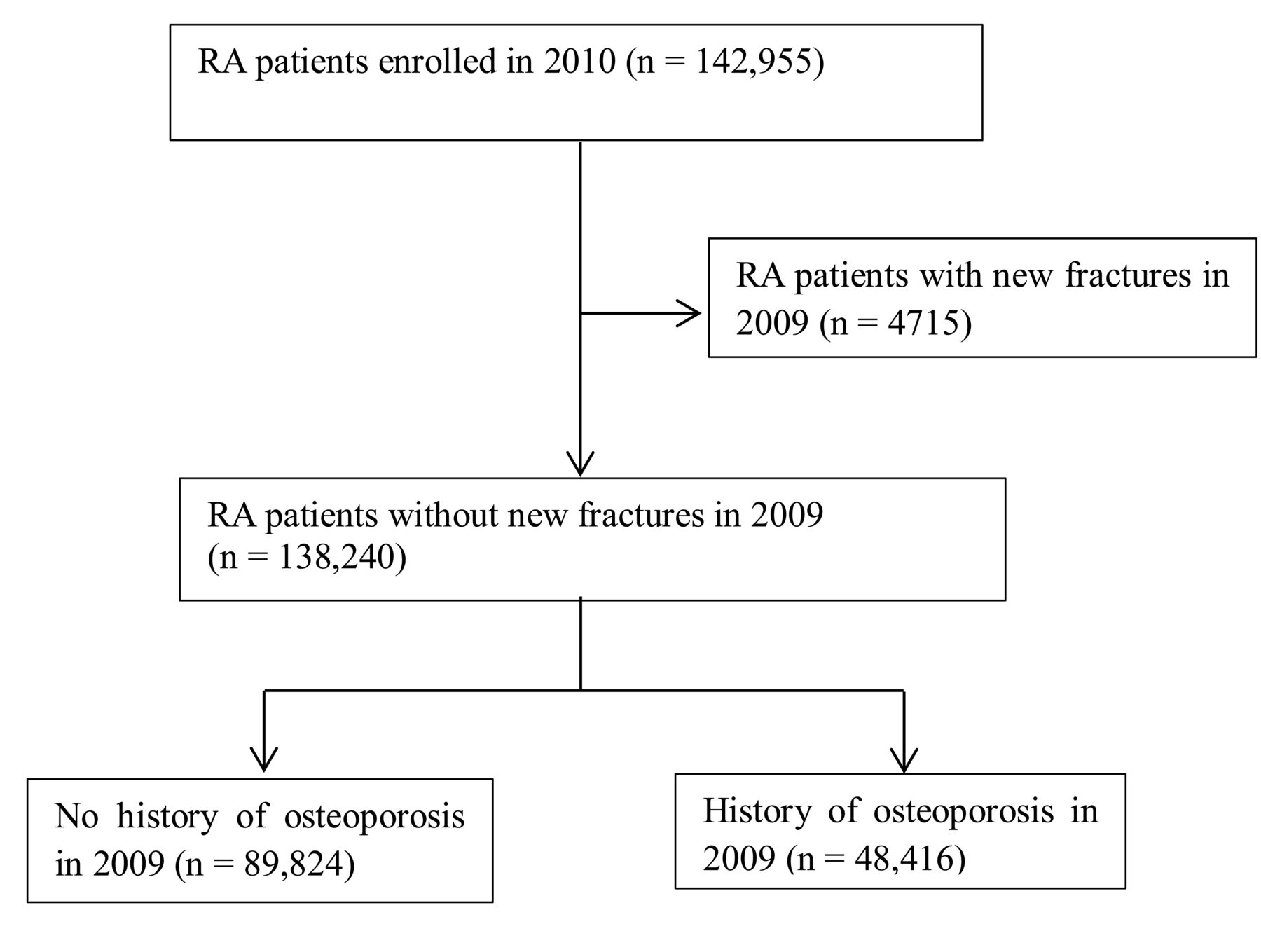
Patients with RA from 2010 were identified using the RA diagnostic code and the prescription of any disease-modifying antirheumatic drugs within 1 year, according to our previously validated definition23. Among them, we excluded patients with RA who experienced any fractures in 2009 (Figure 1). We also identified patients without a history of osteoporosis to assess the effect of oral GC on patients with a relatively lower risk of fractures. Patients without a history of osteoporosis were defined as those without a diagnostic code for osteoporosis in 2009 or those who were not prescribed any osteoporosis treatments in 2009. Because of the low cost and high prevalence of bone mineral density (BMD) performance in Korea, diagnostic codes for osteoporosis in patients with RA are more accurate than in other populations.

Patient selection flow. RA: rheumatoid arthritis.
This study was approved by the HIRA Research Ethics Committee of South Korea (NSCR-2014-3).
Fracture incidence in patients with RA
We established a retrospective cohort using the claims database of HIRA from January 2010 to December 2010. We included patients with RA aged ≥ 19 years, and followed those included through December 2013. The date of the first claim was defined using the RA diagnostic code as the RA index date. The observational period was defined as that between the RA index date and either the incidence of fracture or the last visit up to December 2013.
Fractures were identified on the basis of select International Classification of Diseases, 10th ed (ICD-10) codes, which were adapted from a previous study that estimated the incidence of fracture in Korea using the same claims database, and hospitalization or outpatient clinic visits according to fracture site24. Vertebral fractures were defined by the following diagnostic codes, accompanied by hospital admission or > 3 outpatient visits within 6 months of fracture: M48.4 (fatigue fracture of vertebra), M48.5 (collapsed vertebra, not elsewhere classified), S22.0 (fracture of thoracic vertebra), S22.1 (multiple fracture of thoracic spine), and S32.0 (fracture of lumbar vertebra). Hip fractures were defined by the diagnostic codes S72.0 (fracture of neck) and S72.1 (pertrochanteric fracture). These patients must have also had 1 hospital admission or emergency room visit and the following related procedures: open reduction of fractured extremity (femur), closed pinning (femur), external fixation (pelvis, femur), closed reduction of fractured extremity (femur), bone traction, skin traction (hip), and hemiarthroplasty (hip). Fractures of the clavicle, humerus, wrist, and ankle were also identified by their diagnostic codes and by > 1 hospital admission, or 3 outpatient clinic visits for the same diagnostic codes within 6 months of fracture development. We identified fracture at 6 different sites, including the spine, clavicle, humerus, wrist, hip, and ankle.
Oral GC and other risk factors for fracture in patients with RA
Information regarding oral GC use was collected in detail. We included all kinds of oral GC such as deflazacort, dexamethasone, hydrocortisone, methylprednisolone, prednisolone, and triamcinolone. In addition, GC dose was calculated as a prednisolone-equivalent dose. The patterns of GC use were collected from prescription information in the database, and we used the concept of medication possession rate (no. dispensed medication doses ÷ no. days in a unit of time). Only patients who had ever taken GC during the observational period were included and categorized as GC users in this analysis. Although this definition is usually acceptable in the studies based on the claims database, we could not confirm that patients took the whole GC amount prescribed between each prescription. Hence, we did not calculate the GC exposure days as a continuous variable, but rather categorized the duration of GC exposure as 0, < 3 months, between 3–6 months, and > 6 months during 3 years of followup. The duration of GC use was the period of prescribed oral GC from the RA index date to the development of a fracture or the last visit until December 31, 2013. The mean dose of oral GC was calculated as the cumulative dose of oral GC during the observational period, divided by GC duration. The highest dose of oral GC was identified as the highest daily dose prescribed during the observational period.
We collected information about other fracture risk factors including age, sex, payer type, type of institution, physician’s specialties, comorbidities, and medications. Comorbidities that are associated with fracture, such as hyperparathyroidism, hyperthyroidism, endstage renal disease (ESRD), chronic pulmonary disease, and inflammatory bowel disease (IBD), were detected using ICD-10 codes during the observational period. We recorded the use of any medications related to RA or osteoporosis that were prescribed for > 30 days during the observational period.
Statistical analyses
Demographic and clinical characteristics were described in a descriptive analysis. The incidence of fracture was calculated [in 10,000 person-yrs (PY)] according to fracture site and sex. To identify factors associated with fractures, we performed multivariate logistic regression analysis, after adjusting for variables that were significant in crude analysis or significant in the literature. In addition, to examine the effect of oral GC use on various fracture types, we performed crude logistic regression analysis to find the association between variables such as duration, mean dose, and highest daily dose of GC and fractures. We then performed multivariable logistic regression analysis adjusted for age, sex, payer type, type of institution, physician specialties, RA- or osteoporosis-related medications, and comorbidities including hyperparathyroidism, hyperthyroidism, ESRD, chronic pulmonary disease, and IBD. Finally, we performed logistic regression analysis to identify the effect of oral GC use on RA patients without osteoporosis who are not considered at high risk of fracture.
All analyses were performed using SAS 9.2 (SAS Institute). P values < 0.05 were considered statistically significant.
RESULTS
Demographic and clinical characteristics of patients with RA
The mean age of the RA cohort was 54.2 years. A majority of those patients (78.4%) were female (Table 1). Hyperthyroidism and chronic pulmonary disease were present in 7.8% and 32.8% of patients, respectively. Regarding RA treatments, 48.6% of patients were taking methotrexate (MTX) and 2.6% biologic agents. GC were used in the treatment of 68.2% of patients for > 3 months. The mean dose of GC was 6.1 ± 4.7 mg, and the highest daily dose was 16.2 ± 15.8 mg.
Demographic and clinical patient characteristics (n = 138,240). Values are n (%) unless otherwise specified.
Fracture incidence in patients with RA
A total of 11,599 fractures were observed in 9964 patients among a total of 138,240 patients with RA in 499,881 PY (Figure 2). The incidence of fracture at any site was 232.0/10,000 PY in all patients, 144.7/10,000 PY in male patients, and 255.2/10,000 PY in female patients. The total incidence of vertebral, hip, and nonvertebral/nonhip fractures were 117.0/10,000 PY, 28.0/10,000 PY, and 89.0/10,000 PY, respectively.

Incidence of fracture according to anatomical site and sex.
Factors associated with fracture in patients with RA
Multivariable regression analysis showed the traditional risk factors for fracture, including advanced age, female sex, and comorbidities such as ESRD and chronic pulmonary disease, were all significantly associated with fractures in patients with RA (Table 2). In addition, factors related to the use of medical services such as payer type, type of institution, and physician specialty were also associated with fractures. The use of certain medications that are commonly prescribed for RA, including nonsteroidal antiinflammatory drugs and proton pump inhibitors, were associated with increased risk for fractures. In contrast, the use of MTX and biologic agents was not associated with fracture risk. Other medications that are known to be associated with increased risk of osteoporosis or fractures, including anticoagulants and antidepressants, were associated with increased risk of fracture. Antiosteoporotic agents, which are usually used in patients with osteoporosis, were also associated with increased risk of fracture in our analysis; this may be explained by indication bias. In contrast, thyroid hormone was not associated with fractures.
Demographic and clinical factors associated with fracture at any sites.
The effects of GC on fracture in patients with RA
We performed crude and multivariable logistic regression analyses to determine the specific effects of GC use on fractures (Table 3). Crude analysis showed that longer duration, higher mean dose, and higher dose of GC all increased the rate of vertebral and nonvertebral/nonhip fractures. In contrast, these variables were not significantly associated with hip fractures. An adjusted analysis showed GC duration ≥ 6 months (OR 1.76, p < 0.01), mean dose ≥ 2.5 mg (OR range 1.37–1.71, p < 0.01), and highest daily dose ≥ 10 mg (OR range 1.23–1.75, p < 0.03) all increased the risk of vertebral fractures. However, neither the duration nor the dose of oral GC increased the risk for hip and nonvertebral/nonhip fracture.
Effect of GC duration, mean daily dose, and highest dose by fracture site. Data are OR (95% CI).
Effect of GC use on fracture in RA patients without osteoporosis
Although patients with RA who do not have a history of osteoporosis are at increased risk of fracture, many physicians and patients do not consider them to be at high risk. The effect of GC use on fracture risk was comparable in RA patients with and without underlying osteoporosis (Table 4). An adjusted analysis showed duration of GC ≥ 6 months (OR 1.80, p < 0.01), mean dose ≥ 5 mg (OR range 1.46–1.80, p < 0.01), and highest daily dose ≥ 20 mg (OR 1.82, p < 0.01) all increased the risk of vertebral fractures. In contrast, neither the duration nor the dose of oral GC was associated with the risk of hip fracture. Unfortunately, we could not perform similar analyses on nonvertebral/nonhip fractures because of technical limitations with access to the database.
Effects of GC duration, mean daily dose and highest dose according to site in RA patients without osteoporosis. Values are OR (95% CI).
DISCUSSION
In our study, GC use, accompanied by other demographic and clinical variables such as age, sex, comorbidities, and medications, was significantly associated with increased fracture risk. The longer the duration of GC use, the higher the mean dose; the greater the highest daily dose, the greater the risk of vertebral fracture. In contrast, neither the duration nor the dose of oral GC increased the risk of hip and nonvertebral/nonhip fractures in patients with RA.
Among various risk factors for fractures, we focused on GC use in our study. Because prior fracture was one of the strongest risk factors for fractures25, it would be hard to identify other fracture risk factors. Therefore, we excluded patients who had experienced a recent fracture from our analysis to better identify the GC effect and other risk factors for new fractures. However, because of the limitation of the database we used, we excluded only patients who experienced fractures in 2009. In addition, some studies assumed that RA disease duration might affect the risk of fracture26. However, in our analysis, we could not adjust RA disease duration because of limitations in the claims database we used and our inclusion criteria. In general, patient age is well correlated with disease duration2,4,27. Therefore, age might be a valuable covariate for adjusting disease duration in our analysis.
Our results were comparable to those of previous studies with regard to some findings, but differed with regard to others. Our results of adjusted analysis confirmed prior results that longer GC use duration and higher mean doses increased the risk of total and vertebral fractures8,19,25. We found no association between GC duration or dose and risk of hip fracture; however, previous studies have reported that GC use was associated with increased risk of hip fractures8. Adjusted analyses showed that shorter GC use durations (≤ 6 mos) decreased the risk of fracture, and daily mean doses > 10 mg actually had a protective effect against hip fractures. We presume that our conflicting results are caused by a difference in the anatomical characteristics and mechanisms of fractures at different sites. Vertebral bones are composed of rich trabecular bone and a thin shell of cortex bone. As previously mentioned, trabecular bone is more likely to be affected by GC use than cortical bone20,21. More than half of vertebral fractures are asymptomatic26 and can develop with minimal or no trauma. Therefore, it is relatively common to see vertebral fracture in patients treated with GC. In contrast, the femur has a thick, strong outer cortex and relatively little trabecular bone. Femur fractures usually occur with higher energy trauma than vertebral fractures, such as falls. Patients who require temporarily high doses of GC may not be functionally active to sustain hip fractures. In addition, the point estimate for hip fracture risk in longer GC users was increased compared to short-term users in an adjusted analysis. This suggests that the longterm use of GC might also increase the risk of hip fracture, although this did not reach statistical significance. Moreover, the negative association between hip fracture and GC use may be a result of our study design, which excluded patients with recent fractures who might have a high risk of fractures. Concerning nonvertebral/nonhip fractures, the duration, mean dose, and highest dose of GC were associated with increased risk of fractures; however, they were not associated with risk of fractures in adjusted analysis. The results were compared with results of nonvertebral fractures in other studies, because there was no study that analyzed the risk of GC on nonvertebral/nonhip fractures in patients with RA. Our results about nonvertebral/nonhip fracture were not comparable with a previous study that reported that increase dose of GC is associated with nonvertebral fractures18. However, in another study, nonvertebral fractures were only associated with disease duration and BMD27. We assumed that other confounding factors, which were not available in this analysis, might be associated with fractures rather than GC, such as RA disease duration, BMD, and functional disability.
In a previous metaanalysis, the onset of bone loss measured by BMD was rapid within the first months after starting GC therapy. It then slowed down after about 1 year of therapy28. In addition, the risk of fracture escalates by about 75% within the first 3 months of starting GC therapy16. In contrast, other groups have reported that the risk of vertebral fracture was highest in the first 3–6 months after starting GC therapy28. However, in our study, GC use > 6 months was associated with an increased risk of fracture in an adjusted analysis, while use > 3 months was associated with an increased risk of fracture in a crude analysis. These differences were likely caused by variations in study design. Compared to previous observational studies that estimated fracture risk during GC use to determine when fractures occurred after starting these medications, we examined the longer effect of GC use on fracture development for the entire 3-year followup period, regardless of GC use at the time of fracture development.
Many researchers have suggested that the risk of fractures only increases in patients taking > 5 mg of GC daily18. However, in our study, GC doses > 2.5 mg were associated with an increased risk of fracture in an adjusted analysis, and even smaller daily doses were associated with an increased fracture risk in a crude analysis. However, in contrast to previous findings, the HR for the mean daily dose was not significantly increased with an increasing dose. We assume that this result was associated with the duration of GC use. Because we calculated the mean dose of GC as the total dose of GC divided by the duration, we could not examine each dose-change event. However, considering that most patients with RA use oral GC for a long duration, understanding the effects of the mean daily dose is more important than that of frequent dose changes.
Patients with RA are sometimes treated with high-dose GC in short-term management of disease flares. However, these high doses are not maintained over a long time. Therefore, we were interested in the effect of high-dose oral GC in the short term. In our analysis, the highest daily doses of oral GC > 10 mg/day also increased the risk of fracture in patients with RA.
There are still conflicting results regarding the cumulative dose of GC. Some groups have reported that the cumulative GC dose was not associated with vertebral fracture19,25, while others have suggested that higher cumulative GC doses increased the risk of fracture18. However, we could not calculate the cumulative dose of oral GC, because relevant information in the database was available only for a limited time.
In our study, we not only analyzed the entire Korean RA population, but also specifically evaluated patients without a history of osteoporosis. Despite widespread evidence that GC increase patient risk of fracture10,12,13, GC are less recognized as therapy that ought to be carefully supervised in patients without osteoporosis. Moreover, potent antiosteoporotic agents (including bisphosphonates and teriparatide) are not typically used in patients with osteopenia or normal BMD, despite longterm GC use10,29. According to our analysis, GC use > 6 months, a daily dose > 5 mg, or a highest daily dose of 20 mg all significantly increased the risk of fracture in RA patients without a history of osteoporosis. Therefore, we need to monitor these patients more closely to prevent fractures.
Our study has several strengths and limitations. First, although clinical risk factors such as RA disease activity and functional disability are associated with fractures, these variables were not available in this database. However, the strength of this database is that it includes almost the entire Korean population. Second, because of the database characteristics, we could not confirm whether patients had actually taken GC or not. Hence, we used the concept of medication possession rate to calculate GC use. In addition, it was impossible to calculate the cumulative lifetime dose of GC. Therefore, we focused on the association between recent use of GC and new fractures in patients with RA. Another limitation is that we did not include BMD in our analyses, although it is the most important associated risk factor for fracture. Instead, we examined the effect of oral GC in patients without a history of osteoporosis to adjust for the effect of BMD and the previous use of osteoporosis medications on fracture. Although we could not use the value of BMD in our analysis, the accuracy of diagnosis and prescription of osteoporosis is quite high, caused by high prevalence of BMD performance. A fourth limitation is that we adapted the definition of fracture from a previous study that estimated the incidence of fractures in the same database. It was not validated, and only 6 common sites of osteoporotic fracture were included24. Because we estimated fractures by diagnostic codes, we may have missed a considerable number of asymptomatic vertebral fractures. Therefore, a prospective study that investigates such asymptomatic fractures is needed to substantiate our findings. In addition, because of the regulation of claims database use in Korea, it was not possible to access the RA patient group without osteoporosis during revision of the manuscript. Therefore, we could not perform the additional analysis about nonvertebral/nonhip fractures in patients without osteoporosis.
The longer the duration and the higher the dose of oral GC, the greater the risk of vertebral fracture. However, GC use does not increase the risk of hip and nonvertebral/nonhip fractures in patients with RA. Further studies are needed to establish a firm conclusion for fracture risks as a result of longterm use of GC in patients with RA.
Footnotes
Supported by a grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute, funded by the Ministry of Health and Welfare, Republic of Korea (grant number HI16C0273).
- Accepted for publication November 7, 2017.








{kind=link}
{kind=link}