

Abstract
Objective. Around one-third of patients with juvenile idiopathic arthritis (JIA) fail to respond to first-line methotrexate (MTX) or anti-tumor necrosis factor (TNF) therapy, with even fewer achieving ≥ American College of Rheumatology Pediatric 70% criteria for response (ACRpedi70), though individual responses cannot yet be accurately predicted. Because change in serum S100-protein myeloid-related protein complex 8/14 (MRP8/14) is associated with therapeutic response, we tested granulocyte-specific S100-protein S100A12 as a potential biomarker for treatment response.
Methods. S100A12 serum concentration was determined by ELISA in patients treated with MTX (n = 75) and anti-TNF (n = 88) at baseline and followup. Treatment response (≥ ACRpedi50 score), achievement of inactive disease, and improvement in Juvenile Arthritis Disease Activity Score (JADAS)-10 score were recorded.
Results. Baseline S100A12 concentration was measured in patients treated with anti-TNF [etanercept n = 81, adalimumab n = 7; median 200, interquartile range (IQR) 133–440 ng/ml] and MTX (median 220, IQR 100–440 ng/ml). Of the patients in the anti-TNF therapy group, 74 (84%) were also receiving MTX. Responders to MTX (n = 57/75) and anti-TNF (n = 66/88) therapy had higher baseline S100A12 concentration compared to nonresponders: median 240 (IQR 125–615) ng/ml versus 150 (IQR 87–233) ng/ml, p = 0.021 for MTX, and median 308 (IQR 150–624) ng/ml versus 151 (IQR 83–201) ng/ml, p = 0.002, for anti-TNF therapy. Followup S100A12 could be measured in 44/75 MTX-treated patients (34/44 responders) and 39/88 anti-TNF-treated patients (26/39 responders). Responders had significantly reduced S100A12 concentration (MTX: p = 0.031, anti-TNF: p < 0.001) at followup versus baseline. Baseline serum S100A12 in both univariate and multivariate regression models for anti-TNF therapy and univariate analysis alone for MTX therapy was significantly associated with change in JADAS-10.
Conclusion. Responders to MTX or anti-TNF treatment can be identified by higher pretreatment S100A12 serum concentration levels.
Juvenile idiopathic arthritis (JIA) is a clinically heterogeneous condition, frequently requiring therapy with conventional disease-modifying antirheumatic drugs (cDMARD) such as methotrexate (MTX). Combination therapy increasingly also includes biological DMARD (bDMARD) with anti-tumor necrosis factor (TNF) agents [e.g., etanercept (ETN) and adalimumab (ADA)]1,2,3. However, up to 40%, or even higher depending on the definition used, of patients will not respond to treatment with bDMARD4,5,6. Using biomarkers alongside known predictive demographic and clinical factors could help improve the prediction of response1,7,8.
S100A12 and myeloid-related protein complex 8/14 (MRP8/14 or S100A8/A9) are S100-protein family members. Both are calcium-binding proteins and phagocyte activation markers acting as proinflammatory ligands of Toll-like receptor-4, which are constitutively expressed predominantly in phagocytic myeloid cells (i.e., granulocytes and monocytes). It is thought that both proteins are secreted in a similar mechanism, either by nonclassical secretion from active cells or passively released from necrotic cells9. Both S100A12 and MRP8/14 are validated predictors of relapse risk and disease activity in JIA10,11,12. S100A12 concentration measured at the time of treatment withdrawal in patients with JIA predicted the development of flare better than MRP, with the combination of S100A12 plus high-sensitivity C-reactive protein performing best13. This suggests that differences exist in the performance of S100A12 and MRP8/14 as biomarkers, despite their many apparent similarities. Baseline MRP8/14 has already been shown to predict response to MTX and anti-TNF treatment in patients with JIA. However, the association of serum S100A12 with response to therapy in JIA has not yet been evaluated14,15.
MATERIALS AND METHODS
Study population
Data were analyzed from 3 prospective cohort studies that were designed to study either the response to starting MTX or starting anti-TNF treatment (alone or in combination with other therapy including MTX; Table 1) in patients with JIA diagnosed according to the International League of Associations for Rheumatology (ILAR) criteria3. The study was open for patients with undifferentiated JIA, but no such patient was enrolled. The prediction of response by MRP8/14 in these cohorts has already been published in detail14,15, and here we focus on reporting the associations of S100A12. Response to MTX was analyzed using data from the UK Childhood Arthritis Response to Medication Study (CHARMS, 75 patients). Data on response to anti-TNF treatment were collected in the Dutch Arthritis and Biologicals in Children (ABC) Register (n = 68), the German Registry for Biologics in Paediatric Rheumatology (BIKeR, n = 12), and the CHARMS (n = 8). Each of these studies recruited patients with all subtypes of JIA who fulfilled ILAR criteria and started either new DMARD or biologic therapy for active arthritis (CHARM). ABC and BIKeR cohort data were combined to increase statistical strength. MTX and anti-TNF therapies were prescribed at the dose according to the previously published study protocols4,6,14.
Baseline demographics and characteristics of patients starting MTX and anti-TNF therapy.
The BIKeR registry was approved by the ethics committee of the Ärztekammer Nordrhein Düsseldorf (ref 2/2015/7441). The CHARMS was approved by the Institute of Child Health/Great Ormond Street UK National Health Service Trust (MREC-05/Q0508/95), and the ABC Register was approved by the Medical Ethics Committee at Erasmus MC Rotterdam (MEC-225.804/2003/51). The BIKeR and ABC registries as well as the CHARMS included provision in their ethical approvals for the collection, storage, and analysis of biobanked samples. All 3 cohorts have been published in full elsewhere. Subjects were recruited with fully informed consent and child assent where appropriate4,6,14.
Definition of treatment response
Treatment responders achieved an American College of Rheumatology (ACR) Pediatric 50% criteria for response (ACRpedi50) or better score at followup, equivalent to ≥ 50% improvement in a minimum of 3 out of 6 core variables, with no worsening in > 1 remaining variable by > 30%. Core variables are (1) physician’s global assessment (PGA) score, using visual analog scale (VAS): range 0–10 cm, 0 = best score; (2) patient/parent global assessment of well-being (VAS: range 0–10 cm, 0 = best score); (3) Childhood Health Assessment Questionnaire (CHAQ, range 0–3, 0 = best score); (4) number of joints with active arthritis; (5) number of joints with limited motion; and (6) erythrocyte sedimentation rate (ESR)3,16. Disease activity and response were also quantified by parent/patient pain VAS, the achievement of inactive disease and change in Juvenile Arthritis Disease Activity Score (JADAS)-10, defined as the difference between baseline and followup JADAS-1017. The JADAS-10 score is quantified in 4 domains, 3 on a continuous scale (PGA, parent/patient global, and no. active joints out of 10 specified), and the fourth being the presence of a normalized ESR18. The modified definition of inactive disease (ID; Wallace, et al19) requires the absence of active arthritis, systemic features, uveitis, and normal ESR (≤ 20 mm/h), but accepts a higher acceptable PGA of ≤ 1.0 cm (which in practice is rarely scored as 0), compared to the standard ID definition. Because all patients achieving ID also fulfill ACR50, ACR50 was used as the measure of response; if any prediction of response was found with this lower threshold, it is likely the same, or a higher response would be present with the use of ID. Baseline demographics and clinical scores including JADAS-10 are shown in Table 1, and the followup characteristics (responders and nonresponders) are shown in Supplementary Table 1 (available with the online version of this article).
S100A12 measurement
Serum concentrations were measured using a well-described in-house ELISA assay as well as a commercial assay (CircuLex, CycLex Co. Ltd) on frozen samples11,13. Both assays were used to investigate whether measured concentrations were reproducible in both, and to identify a suitable commercial assay approved for research use in further studies, which do not have access to this in-house ELISA. Reference internal control sera were used in each assay. S100A12 is a stable biomarker that is reliably measurable in samples sent at room temperature as well as in repeatedly thawed and frozen samples. All reported S100A12 values refer to in–house assay results unless specified. Results using the commercial assay are shown in Supplementary Tables 2 and 3 (available with the online version of this article). All assays were performed blind to the clinical diagnosis and results were not reported to treating clinical staff during the study. Results are presented as median (interquartile range; IQR).
Statistical analysis
Categorical characteristics were tested using the chi-square test, continuous variables with the Mann-Whitney U test, and correlations with the Spearman (rs) or Pearson (r) test. Baseline and followup S100A12 were compared in paired analyses using the Wilcoxon signed-rank test. Baseline S100A12 concentration was assessed for its prediction of ACRpedi outcome by binary logistic regression modeling and association with change in JADAS-10 by linear regression modeling. Multivariable linear models were also fitted for change in JADAS-10, allowing correction for other potential predictors and to assess the added value of S100A12 in predicting response. For this modeling, known predictive variables (sex, age at JIA onset, disease duration, baseline JADAS-10, baseline CHAQ, no. previously used DMARD, and ESR) were prespecified7,8,20,21. Missing data were handled using the chained equations multiple imputation command ice in Stata/SE (v13.0). Patients treated with anti-TNF (ADA or ETN) were combined after being assessed as having identical characteristics. Cutoff values for baseline S100A12 as a predictive marker for treatment response were defined using receiver-operator characteristic (ROC) analysis13. Other analyses were performed with SPSS (IBM for Windows V.21) and Prism (Graphpad v5).
RESULTS
Baseline characteristics
Baseline median S100A12 concentration in patients before either therapy (MTX: n = 75, anti-TNF: n = 88) significantly correlated with baseline ESR (MTX rs 0.40, p < 0.001; anti-TNF rs 0.38, p < 0.001) and JADAS-10 (MTX rs 0.25, p = 0.04; anti-TNF rs 0.22, p = 0.04; Table 1). Subgroup analysis of S100A12 with number of active joints at start showed no correlation (Spearman’s ρ 0.19, p = 0.072). In MTX-treated patients, there was no difference in baseline S100A12 among JIA subtypes (p = 0.17, Kruskal-Wallis test). However, in patients treated with anti-TNF, a difference among patients of different subtypes was seen (p = 0.024), with the highest concentrations in polyarticular rheumatoid factor–positive JIA (median 411 ng/ml, n = 13) and the lowest in oligoarticular-persistent JIA (median 56 ng/ml, n = 5).
Clinical response to therapy
Followup was at a median of 6.6 months (IQR 5.8–7.6) for MTX and 3.2 (2.6–5.0) months for patients treated with anti-TNF. The clinical response of each treatment group was analyzed separately, therefore this difference did not affect the results shown. Based on achievement of ACRpedi50 or better at followup, 57 of 75 MTX-treated patients and 66 of 88 anti-TNF patients were responders. Of the 66 anti-TNF responders, 46 had an ACRpedi70 or better response, while 31 were in clinical remission. The modified criteria for ID were fulfilled by 25/75 of MTX and 31/88 of patients treated with anti-TNF. JADAS-10 at followup was median 3 (IQR 1–8) for MTX-treated and 4 (1–9) for anti-TNF–treated patients (Supplementary Table 1, available with the online version of this article), improving from baseline (Table 1). There were no significant differences between responders and nonresponders for either treatment group in baseline disease characteristics, excluding the variables included in the ID and JADAS-10 score (Supplementary Table 1).
Baseline S100A12 and response to therapy
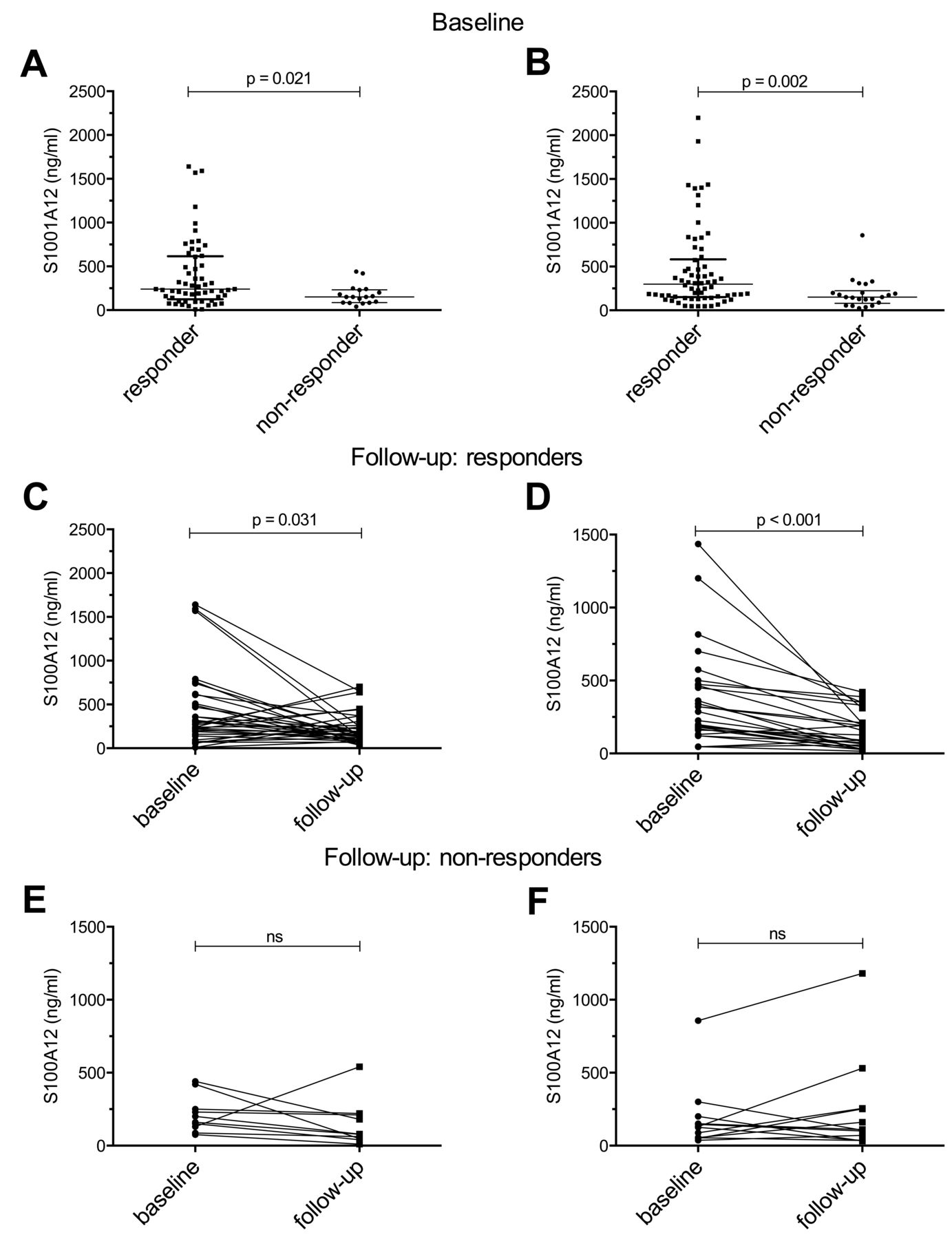
Baseline S100A12 concentration was higher in responders versus nonresponders [Figure 1A, MTX median 240 (IQR 125–615) ng/ml vs 150 (87–233) ng/ml, p = 0.02; Figure 1B, anti-TNF median 308 (IQR 150–624) ng/ml vs 151 (IQR 83–201) ng/ml, p = 0.002]. Increased baseline S100A12 was associated with OR > 1 for the prediction of ACRpedi50 and improvement in JADAS-10 in univariate models at followup, for both treatments (Table 2). For patients using anti-TNF and MTX therapy, logistic regression modeling was also performed with the additional variable “MTX at start” and the OR for baseline S100A12 did not change, and concomitant MTX was not a significant factor in the combined model (OR 3.46, 95% CI 0.93–12.85). Multivariate models constructed with known predictors of response, as detailed in the statistical methods above, tested their prediction of JADAS-10. Excluding S100A12, model variables explained 70% of the variance in change in JADAS-10 at followup for MTX-treated patients and 50% of the variance for the anti-TNF group. Including S100A12 as a variable improved the predictive models by 2% (not significant) for MTX and 5% (p = 0.004) for anti-TNF therapy (Table 2).

Baseline and followup S100A12 concentration by therapy used. Differences in baseline S100A12 concentrations in responders and nonresponders to MTX (A) or anti-TNF therapy (B) measured by the in-house ELISA are shown. Change in S100A12 concentration after treatment with MTX and anti-TNF therapy is shown for responders (C–D) and nonresponders (E–F). Horizontal bars indicate the median concentration and vertical bars the interquartile range. MTX: methotrexate; anti-TNF: antitumor necrosis factor.
Association of response to therapy to baseline S100A12 concentration.
Followup S100A12
Followup S100A12 concentrations were determined for MTX (44/75) and anti-TNF (39/88) patients, limited only by lack of serum for this analysis, which was performed blinded. Of these, 34/44 (77%) of MTX and 26/39 (67%) of anti-TNF patients were responders. At followup, both responders and nonresponders, irrespective of therapy, had comparable S100A12 concentrations: MTX responders median 165 (IQR 113–273), nonresponders 79 (46–213, p = 0.08); anti-TNF treatment responders median 110 (53–254), nonresponders 91 (42–235, p = 0.55; Figure 1). However, responders (those achieving ACRpedi50) had significant reduction from their baseline S100A12 concentration measured by the Wilcoxon signed-rank test (Supplementary Table 1, available with the online version of this article). Sensitivity, specificity, and likelihood ratios for prediction of response by S100A12 using ROC analysis are shown in Table 3.
Sensitivity, specificity, and likelihood ratios for the determined cutoff of S100A12 predicting response to MTX and anti-TNF therapy.
Use of concomitant therapy
Concomitant therapy was given according to physician choice. The percentage of patients using concomitant MTX at the start of anti-TNF therapy in the group of responders was 91% (60/66) and in the nonresponders, 63% (14/22). Systemic corticosteroid use at the start of MTX treatment (n = 25/61, 41%) was not associated with any significant differences in either baseline or followup S100A12. However, in the anti-TNF treatment group, those who were also receiving corticosteroids at the start of the treatment (n = 25/88) had higher baseline S100A12 than those who did not (median 380, IQR 177–838 ng/ml vs 187, IQR 128–331 ng/ml, p = 0.006) and also greater change at followup [ΔS100A12 −145 (−327 to −97) vs −84 (−149 to 13), p = 0.034]. However, there was no difference in corticosteroid use between patients characterized as responders or nonresponders, therefore concomitant corticosteroid use was unlikely to be the major factor in patients reaching clinical response. So few patients used concomitant DMARD (excluding MTX; MTX-treated = 3/66; anti-TNF–treated = 3/88) that no conclusions could be drawn.
Measurement of S100A12 by commercial ELISA
S100A12 measured by commercial assay (Supplementary Table 2, available with the online version of this article) was comparable with in-house assay results and also showed significantly higher S100A12 in responders versus nonresponders and higher baseline versus followup concentrations. However, while a good area under the curve (AUC) was obtained for both therapy groups, it was lower with the commercial (MTX AUC 0.662, 95% CI 0.532–0.791; anti-TNF 0.675, 95% CI 0.550–0.800) versus in-house assay (MTX AUC 0.675, 95% CI 0.559–0.805; anti-TNF 0.734, 95% CI 0.662–0.846). Sensitivity (commercial ELISA: MTX 45.6, anti-TNF 39.4; in-house ELISA: MTX 47.4, anti-TNF 58.6) and specificity (commercial ELISA: MTX 83.3, anti-TNF 86.4; in-house ELISA: MTX 88.9, anti-TNF 80.7) were also lower with the commercial ELISA. Absolute commercial assay concentrations were also higher than the in-house assay, about double, and the cutoff levels calculated for each therapy group were also much wider than with the in-house assay.
DISCUSSION
Baseline serum S100A12 was associated with response to both MTX and anti-TNF therapy in patients with JIA who had a high baseline concentration that decreased significantly with either MTX or anti-TNF treatment. Patients with higher baseline S100A12 concentration had higher disease activity and ESR, and were more likely to be treatment responders. Further, the addition of S100A12 to multivariate models improved the prediction of response.
The aim of our study was not to directly compare level of response to MTX versus anti-TNF therapy, or to consider their combined therapy versus individual use, but rather to determine whether S100A12 concentration can predict a response to therapy when a clinician initiates either of these medications. Further work and specific trials are needed to determine which therapy would be best initiated in which patients, and such studies would also require the availability of predictive markers of response, such as S100A12, which is discussed here.
S100A12 has already been shown to correlate with disease activity, and concentrations > 175 ng/ml potentially predict increased risk of flare in patients who have had treatment withdrawn10,13,22,23,24. The followup time of patients in our study was a median of 5 months. Most patients would be expected to show a treatment response within 3 months after initiation, with S100 concentrations shown to decrease in response to effective biological treatment within 4 weeks25,26.
Moncrieffe, et al and Anink, et al identified MRP8/14 as being associated with response to MTX and anti-TNF therapy, and also suggested predictive modeling could be improved by including additional variables14,15. S100A12, like MRP8/14, has the advantage over other cytokines, e.g., interleukin 1β, in having greater temperature stability, even withstanding storage and being mailed at room temperature. S100A12 measurement could therefore feasibly be incorporated into the routine laboratory examinations for JIA and also be incorporated into treatment prediction models7,21,27,28.
While a well-established experimental ELISA S100A12 protocol exists, it is not yet in routine use. The commercial ELISA has already been demonstrated to perform well in analyzing patient serum11,29. Both assays require serial dilution of serum to obtain reliable results, owing to the wide range of S100A12 concentrations among patients11. Therefore, while either assay can be used, results from each should not be directly compared and used only with assay-specific cutoffs. Although overall the same pattern of results was obtained with both assays, the in-house ELISA performed marginally better, as reflected by the slightly higher AUC and Youden Index values achieved for both MTX and anti-TNF treatment groups with the in-house assay compared to those of the commercial assay.
Whereas S100A12 and MRP8/14 have reported some similarities in intra- and extracellular functions, the mechanism of release for each remains unknown. There are clear differences in the expression and functions between the 2 proteins9. A hallmark of MRP8/14 is its formation of a heterodimer, while the hexamer is thought to be the active extracellular form of S100A1230. Adding S100A12 into the multivariable models (investigated for MRP8/14 by Moncrieffe, et al) did result in a further increase in explained variance, though only a relatively small percentage (2%, nonsignificant) for MTX, but 5% (p < 0.005) for the anti-TNF group14.
In this cohort, baseline ESR and number of active joints already differentiated well those patients who later became responders from nonresponders, which could be one reason the addition of S100A12 to a multimarker model added limited benefit. Other cohorts, particularly larger clinical cohorts, are required to ascertain whether S100A12 is a clinically useful predictive marker.
It is likely that no single biomarker can be sufficiently sensitive or specific for predicting response, and multimarker panels are increasingly being sought, such as the multibiomarker disease activity test for rheumatoid arthritis1,31. It is also important to acknowledge that there is, to date, a lack of clinically viable alternative biomarkers that could replace S100A12 or MRP8/14, or add to their prediction in such multivariable models. Additionally, heterogeneity within the same subgroup of JIA could be a further factor in variation in treatment response, and would further support the use of multimarker panels to individualize management strategies. Small cohort size also increases the chance of clinical heterogeneity leading to statistically significant outcomes, and we combined 2 cohorts for the anti-TNF group to counter this. Larger studies would require greater multicenter collaboration and the use of inception cohorts. One factor that could be investigated is the presence and influence of TNF-α gene polymorphisms, which could be associated with the heterogeneity of response to anti-TNF treatment32.
Biological and MTX therapies are associated with potentially significant adverse effects, and are expensive3,25,33. Most importantly, around a third of patients will show poor response to therapy4,5,6,7. In our study, the initiation of both MTX and anti-TNF treatment was effective and was associated with improvements in clinical disease activity measures, JADAS-10 score, attainment of ID, and ACRpedi50 responses. Because of limitations in the size of the dataset, we could not perform further subgroup analyses of response by each ACRpedi level, and instead used ACRpedi50 or better as the cutoff, using information from the JADAS score to supplement the measure of clinical improvement. Over 50% of patients in each group reached an ACRpedi50 or better response, in line with published literature, including the study of ETN efficacy by Quartier, et al, in which over half of treated patients with JIA had over a minimum 50% improvement in their core set criteria at 3 months25. Alongside the baseline characteristics, this result suggested that our patient population was an average group34. However, the effect of concomitant therapy use by patients (MTX plus anti-TNF therapy and/or other therapies such as corticosteroids) should be investigated specifically in more detail.
We have shown that high pretreatment S100A12 serum concentrations of patients with JIA are associated with a good response to MTX or anti-TNF therapy. Further work should be done to identify the ideal clinical scenarios in which this biomarker could best be used (at onset of treatment in the absence of corticosteroid treatment, for example, or limited to anti-TNF–treated patients, or to predict patients who will respond to one drug rather than another, or in combined therapies from the outset). In addition, this work highlights that there is a significant clinical need for the clinical evaluation of predictive biomarkers. However, to achieve these objectives, validation cohorts with frequent longitudinal followup are required.
ONLINE SUPPLEMENT
Supplementary material accompanies the online version of this article.
Acknowledgment
The authors thank all the patients and their families for participating in the included studies, the ward and clinical staff for help collecting samples and data, and laboratory teams for sample handling and processing, as well as each member of the study groups (Childhood Arthritis Response to Medication Study, CHARMS; Arthritis and Biologicals in Children, ABC Register; and the Biologics in Paediatric Rheumatology, BIKeR Registry). We especially thank M. Saers and S. Schleifenbaum for excellent technical assistance.
Footnotes
F.G. was supported by the European Union Seventh Framework Programme (FP7) EUTRAIN (ref.289903) grant. L.W. is supported by the Great Ormond Street Hospital Children’s Charity. D.H. and D.F. were funded by the Interdisciplinary Centre of Clinical Research at the University of Münster (IZKF CRA04) and received an unconditional grant from Pfizer Germany for this study. H.M. was supported in part by the US National Institutes of Health (NIH) Grant Award Nos. P30 AR070549, R01 HD089928, U01 AI130830. The content is solely the responsibility of the author and does not necessarily represent the official views of the NIH. The ABC register is maintained with unconditional support from the Dutch Board of Health Insurances (2003-2006), Pfizer, and AbbVie. The BIKeR Registry is supported by an unconditional grant from Pfizer Germany and also the FP7 grant, EC-GA 305266 MIAMI. The CHARMS study was funded by SPARKS UK (08ICH09), the Big Lottery Fund UK (RG/1/010135231), UK Medicines for Children Research Network (NIHR-funded), and NIHR GOS BRC.
- Accepted for publication September 22, 2017.








{kind=link}