

Abstract
Objective. We aimed to estimate the proportion of underdiagnosis and undertreatment of cardiovascular risk factors (CVRF) in an international multicenter cohort of patients with psoriasis and psoriatic arthritis (PsA).
Methods. A cross-sectional analysis was conducted of patients with psoriatic disease from the International Psoriasis and Arthritis Research Team cohort. The presence of modifiable CVRF [diabetes, hypertension (HTN), dyslipidemia, smoking, elevated body mass index, and central obesity] and the use of appropriate therapies for HTN and dyslipidemia were determined. The 10-year CV risk was calculated according to the Framingham Risk Score. Physician adherence with guidelines for the treatment of dyslipidemia and HTN was assessed. Regression analysis was used to assess predictors of undertreatment of HTN and dyslipidemia.
Results. A total of 2254 patients (58.9% PsA, 41.1% psoriasis) from 8 centers in Canada, the United States, and Israel were included. Their mean age was 52 ± 13.8 years and 53% were men. Of the patients, 87.6% had at least 1 modifiable CVRF, 45.1% had HTN, 49.4% dyslipidemia, 13.3% diabetes, 75.3% were overweight or obese, 54.3% central obesity, and 17.3% were current smokers. We found 59.2% of patients with HTN and 65.6% of patients with dyslipidemia were undertreated. Undertreatment was associated with younger age (≤ 50 yrs), having psoriasis, and male sex.
Conclusion. In real-world settings, a large proportion of patients with psoriasis and PsA were underdiagnosed and undertreated for HTN and dyslipidemia. Strategies to improve the management of CVRF in psoriatic patients are warranted.
Patients with psoriasis and psoriatic arthritis (PsA) have an increased cardiovascular (CV) risk. Based on recent metaanalyses, patients with psoriasis and PsA have a 29% and 55% higher risk of developing incident myocardial infarction, respectively1,2. While the increased CV risk in psoriatic patients is attributed in part to the chronic systemic inflammation related to skin and joint disease3,4, the high prevalence of traditional CV risk factors (CVRF) in psoriatic patients significantly contributes to their high CV risk5,6,7. Indeed, the presence of traditional CVRF, including hypertension (HTN), smoking, dyslipidemia, and diabetes mellitus (DM), is associated with a higher burden of atherosclerosis and increased risk of developing CV diseases (CVD) in patients with psoriatic disease4,7,8,9,10. Thus, despite limited data, it is conceivable that controlling CVRF could reduce the risk of CVD in PsA, as has been shown in the general population.
Extensive literature supports the strong link between obesity and its related metabolic abnormalities and psoriatic disease. Patients with psoriatic disease, particularly those with severe psoriasis and PsA, have a higher prevalence of DM, HTN, and dyslipidemia compared with the general population5,11,12,13. This association is stronger than with other chronic inflammatory arthritic conditions, such as rheumatoid arthritis (RA) and ankylosing spondylitis14,15,16.
The recent European League Against Rheumatism recommendations for CVD risk management suggest that all patients with PsA should be assessed for CVRF every 5 years17. The Canadian Cardiology Society considers PsA an independent risk factor for CVD18. Stratification of patients according to their predicted CV risk, as calculated by validated clinical algorithms such as the Framingham Risk Score (FRS), is the first step in the formulation of treatment decisions. However, unlike the recent suggestion to use a multiplication factor of 1.5 for adjusting the estimated CV risk in patients with RA17, there is no parallel modification for CV risk estimation in patients with psoriatic disease. Clinicians are encouraged to use the general population guidelines for CV risk estimation and for the management of CVRF in patients with psoriasis and PsA.
Recent publications found major gaps in the management of CVRF in patients with RA19,20,21; however, little evidence exists about the extent of underdiagnosis and undertreatment of CVRF in patients with psoriasis and PsA. Analysis of patients with psoriasis enrolled in clinical trials found that 19%, 22%, and 39% of patients with DM, HTN, and dyslipidemia, respectively, were untreated for these conditions22. This study also found major gaps in the treatment of HTN and dyslipidemia; however, the generalizability of the results may be limited because the analysis was based on a highly selective population of patients recruited for clinical trials. Little information exists about the adherence to treatment recommendations in patients with PsA and psoriasis in the clinic setting. Additionally, to the best of our knowledge, no study thus far has compared the treatment practices for CV risk management in psoriatic patients across different healthcare systems in different countries. Investigating the physician adherence to screening and treatment guidelines for CVRF among psoriatic patients could identify gaps in care and provide support to develop strategies that address these potential gaps.
The aim of our study was to estimate the proportion of underdiagnosis and undertreatment of CVRF in an international multicenter cohort of patients with psoriasis and PsA, and to investigate factors associated with undertreatment of HTN and dyslipidemia in these patients.
MATERIALS AND METHODS
Population and setting
A cross-sectional analysis of patients with psoriatic disease from the International Psoriasis and Arthritis Research Team (IPART) cohort was conducted. IPART is an international network of dermatologists and rheumatologists from 10 sites mostly in North America that was established to investigate disease-related outcomes in patients with psoriatic disease. Adult patients with PsA and those with psoriasis alone are enrolled and assessed according to a standardized protocol. For our present study, information from 8 sites (5 from Canada, 2 the United States, and 1 Israel) that enrolled more than 50 patients with psoriasis and/or PsA was extracted from the last available study visit. The majority of the patients was enrolled in specialty clinics in academic centers; community-based dermatology and rheumatology clinics and family medicine clinics were additional sources of recruitment. The health systems and access to health services vary across the 3 countries. The United States has a multipayer healthcare system (public and private systems), and access to healthcare services and coverage of medication costs vary widely between individuals. In contrast, the Canadian and Israeli healthcare systems are largely publicly funded and health services are widely available to all citizens. This study was approved by the University Health Network Research Ethics Board (08-0630-AE).
Data collection
Patient evaluation included a history of lifestyle habits, medications and comorbidities, physical examination with blood pressure measurement (measured once), anthropometric measures, and laboratory assessment including nonfasting glucose and lipid profile. Detailed joint examination was conducted including the assessment of tender and swollen joint counts in 68/66 joints, respectively, and the number of dactylitic digits and tender entheseal count according to the Spondyloarthritis Research Consortium of Canada enthesitis index. Low disease activity was defined as having tender and swollen joint counts and enthesitis counts of 1 or less in patients with PsA. The Psoriasis Area and Severity Index (PASI) was used to estimate psoriasis activity. Severe psoriasis was defined as PASI ≥ 10.
Evaluation of traditional CV risk factors
The presence of traditional modifiable CVRF [DM, HTN, dyslipidemia, smoking, elevated body mass index (BMI), and central obesity] and the use of appropriate therapies for HTN and dyslipidemia were determined based on patients’ report, physical examination, and laboratory tests.
Patient height and weight were used to calculate BMI and determine the proportion of patients who were overweight (BMI ≥ 25) or obese (BMI ≥ 30). Central obesity was defined by a waist circumference > 88 cm for women or > 102 cm for men among whites and > 80 cm for women or > 94 cm for men in other ethnic groups23.
HTN was defined as a former medical history of HTN, elevated blood pressure measurement [systolic blood pressure (SBP) ≥ 140 mm Hg or diastolic (DBP) ≥ 90 mm Hg], or the use of blood pressure-lowering drugs. Patients with elevated blood pressure in the absence of a former medical history of HTN or use of appropriate mediations were considered to have undiagnosed HTN.
DM was defined as either elevated nonfasting glucose levels (glucose ≥ 11.1 mmol/l or 200 mg/dl), previous medical history of DM, or use of glucose-lowering medications. Patients with elevated levels of blood glucose in the absence of a previous medical history of DM or use of appropriate mediations were considered to have undiagnosed DM.
Dyslipidemia was defined as a medical history of dyslipidemia, use of lipid-lowering therapy, or abnormal lipid profile [low-density lipoprotein cholesterol (LDL-c) > 3.5 mmol/l (135 mg/dl) or nonhigh-density lipoprotein cholesterol (non–HDL-c) > 4.3 mmol/l (166 mg/dl)] regardless of other CVRF18. Patients with an abnormal lipid profile in the absence of previous medical history of dyslipidemia or use of appropriate mediations were considered to have undiagnosed dyslipidemia.
The 10-year CV risk was calculated according to the FRS derived from an update of the Framingham Heart Study based on the following variables: age, sex, smoking status, total cholesterol, non–HDL-c, and SBP24. When lipid profile was missing (44% of the study population), a BMI-based Framingham global 10-year CV risk score was calculated using the following variables: age, sex, smoking status, SBP, and BMI25. Patients were stratified into 3 risk categories: low (< 10%), intermediate (10–20%), high (> 20%). Patients with preexisting clinical CV disease or DM were included in the high-risk group.
Adherence with treatment recommendations for CV risk factors
Adherence with guidelines for the treatment of dyslipidemia and HTN was assessed. The results were reported for the entire study population and by disease status (PsA or psoriasis). Treatment goals for HTN were defined using the 2014 guidelines for the management of HTN in adults (Eighth Joint National Committee)26. The treatment goals were SBP < 140 mm Hg (or < 150 mm Hg if age > 65) and DBP < 90 mm Hg for the overall population, and SBP < 130 mm Hg and DBP < 80 mm Hg for patients at high CV risk. The treatment goals for dyslipidemia were defined according to the 2013 American College of Cardiology/American Heart Association (ACC/AHA) guideline for the treatment of blood cholesterol. Lipid-lowering therapy was indicated in any of the following: (1) clinical CVD; (2) DM and LDL-c ≥ 70 mg/dl (1.8 mmol/l); (3) 10-year CV risk according to FRS ≥ 7.5% in people 40 to 75 years of age; (4) LDL-c ≥ 190 mg/dl (4.9 mmol/l)27. Because HbA1c or fasting glucose levels were not available for the majority of the study patients, adherence to treatment guidelines of diabetes was not assessed.
Statistical analysis
Statistical analyses were performed using SAS (version 9.4). Descriptive statistics were computed with continuous variables summarized by their means and SD, and categorical variables summarized by proportions. The following categorical variables were assessed as predictors of undertreatment of HTN and dyslipidemia: age group (≤ 50 vs > 50 yrs), sex, disease status (psoriasis vs PsA), severe psoriasis, low PsA disease activity, nonsteroidal antiinflammatory drug use, and corticosteroid use. Logistic regression models were used to assess the association between the above detailed variables and undertreatment of HTN and dyslipidemia.
The initial regression model included only a single covariate. All variables that achieved significance at the 5% level were then included in a more comprehensive multivariable model to identify independent predictors of undertreatment. The effect of each factor was measured with an OR that was estimated along with the respective 95% CI.
RESULTS
A total of 2254 patients (58.9% PsA, 41.1% psoriasis) from 8 centers in Canada, the United States, and Israel were included in the analysis. The mean age was 52 ± 13.8 years and 53% were men. The mean duration of psoriasis and PsA were 21.5 ± 15 years and 13.7 ± 12.1 years, respectively. The characteristics of the study population are shown in Table 1.
Characteristics of the study population (n = 2254). Values are n (%) or mean ± SD.
CVRF in the study population
Of the patients, 87.6% had at least 1 modifiable CVRF. Based on the FRS classification, 30%, 18%, and 52% of patients were in a high, moderate, or low risk category, respectively. Of the patients, 6.5% had ischemic heart disease, 45.1% HTN, 49.4% dyslipidemia, 13.3% DM, 54.3% central obesity, 75.3% were overweight or obese, and 17.3% were current smokers.
The distribution of the different CVRF varied widely across the different sites (Figure 1).
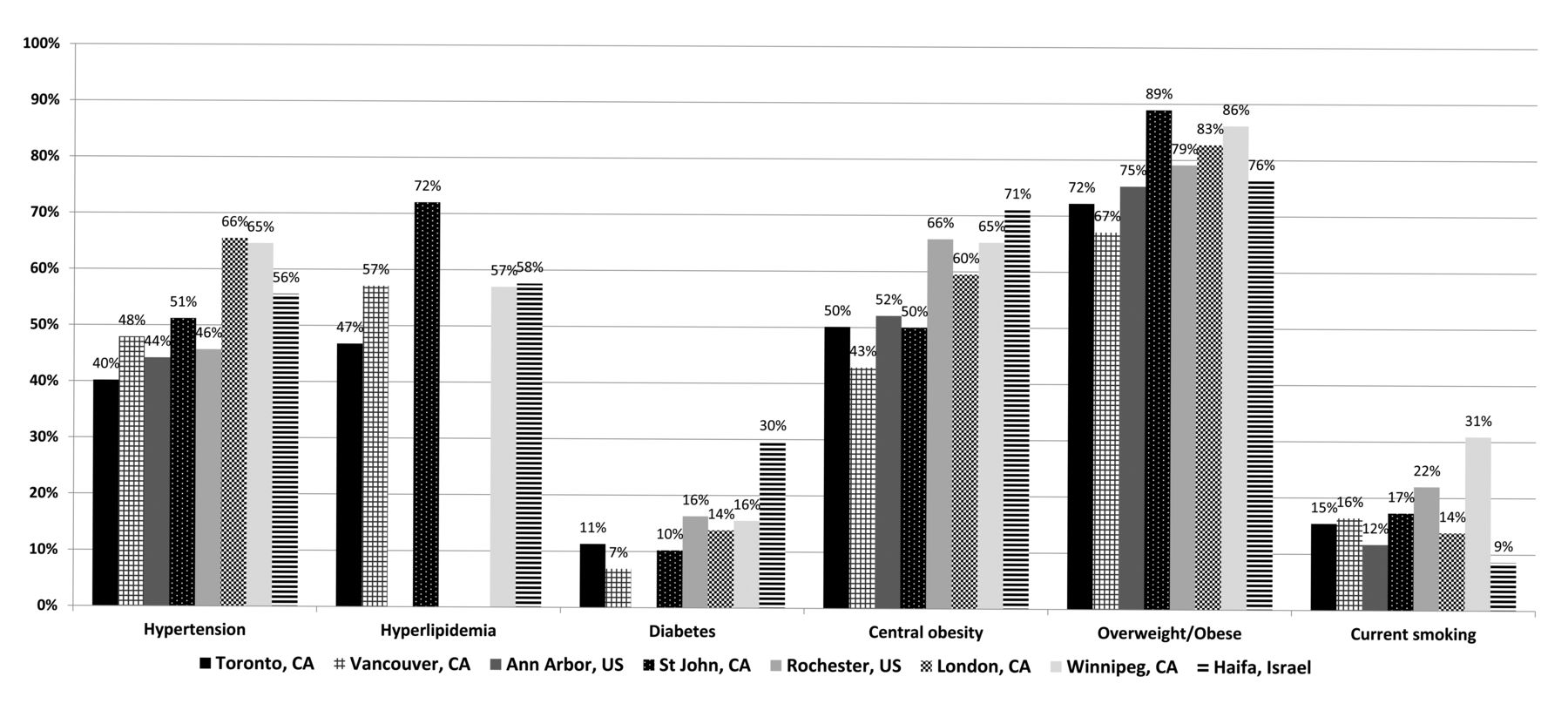
The prevalence of cardiovascular risk factors by site.
The majority of the patients had at least 1 or more CVRF (87.6%). The proportions of patients with more than 1 CVRF were ≥ 2: 70.6%; ≥ 3: 52.9%; ≥ 4: 35.4%; and ≥ 5: 16.7%. Of the patients, 29.3% were using antihypertensive medications, 20.5% were using lipid-lowering drugs, and 10.4% were using antidiabetic drugs. The frequency of underdiagnosis of diabetes was low. Only 9 (4.9%) of 177 patients with diabetes were previously undiagnosed.
Underdiagnosis and undertreatment of HTN
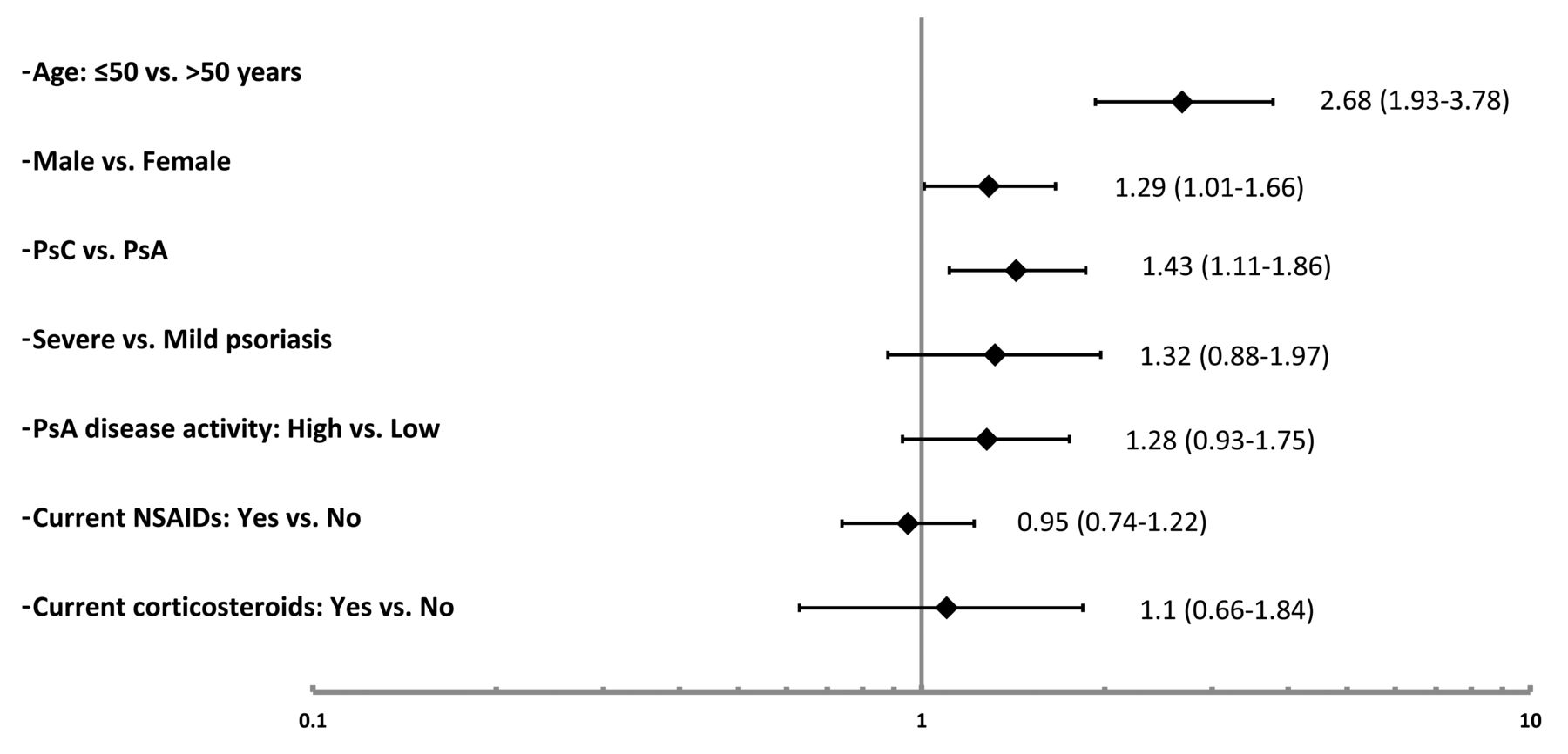
Underdiagnosis and undertreatment of HTN were observed in a significant proportion of the patients across all sites. A total of 1017 (45.1%; PsA: 48.5%, psoriasis: 40.2%) of the study patients had HTN; however, 233 (23%; PsA: 19.9%, psoriasis:39.1%) of these patients did not have a previous diagnosis of HTN and were not taking any blood pressure–lowering medications. Adherence to treatment recommendations was low with 602 patients (59.2%; PsA: 55.9%, psoriasis: 64.8%) found to be untreated or undertreated. Of the patients with clinical CV disease or DM, 60.9% were undertreated for HTN. Among the patients with HTN, the prevalence of undertreatment was lowest in Israel (42.2%) and highest in Winnipeg, Manitoba, Canada (75.2%). We assessed the association between a variety of demographic and disease-related factors and undertreatment of HTN (Figure 2). The following factors were associated with undertreatment of HTN among patients with HTN in univariate regression analysis: younger age (≤ 50 yrs of age: OR 2.68, 95% CI 1.93–3.78), male sex (OR 1.29, 95% CI 1.01–1.66), and disease status (psoriasis vs PsA: OR 1.43, 95% CI 1.11–1.86). In multivariable regression analysis, younger age (≤ 50 yrs of age: OR 2.59, 95% CI 1.87–3.58) and disease status (psoriasis vs PsA: OR 1.36, 95% CI 1.05–1.78) remained independent predictors of undertreatment of HTN.
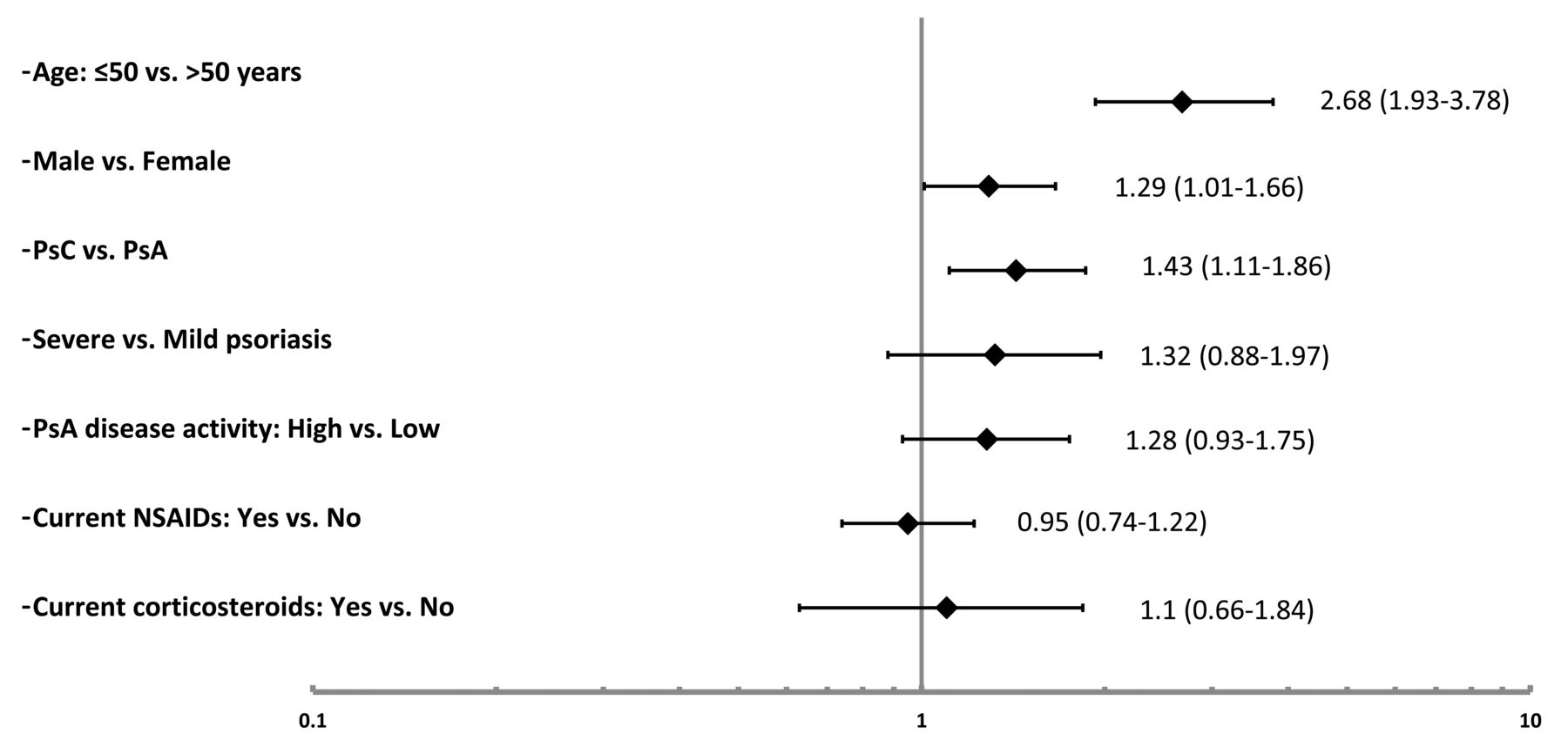
Factors associated with undertreatment of hypertension. Values are OR (95% CI). PsC: psoriasis; PsA: psoriatic arthritis; NSAID: nonsteroidal antiinflammatory drugs.
Underdiagnosis and undertreatment of dyslipidemia
The analysis was limited to 1260 patients with information about their lipid profile. A total of 623 (49.4%) of the study patients had dyslipidemia. However, 35.8% of them did not have a previous diagnosis of dyslipidemia (PsA: 33.6%, psoriasis: 40.3%). Based on the ACC/AHA guidelines, 696 patients (55.2%) had an indication for using lipid-lowering medications. However, adherence to treatment recommendations was low, because only 34.4% of these patients reported using lipid-lowering drugs (PsA: 36.2%; psoriasis: 31.2%). Adherence prevalence was higher in patients with clinical CVD (79%) and DM (61.5%). The prevalence of undertreatment of dyslipidemia was lowest in Israel (38.6%) and highest in Vancouver, British Columbia, Canada (80%). Among the various factors assessed (Figure 3), only younger age was associated with undertreatment of dyslipidemia among patients with an indication for lipid-lowering therapy (≤ 50 yrs of age: OR 1.73, 95% CI 1.02–2.94).
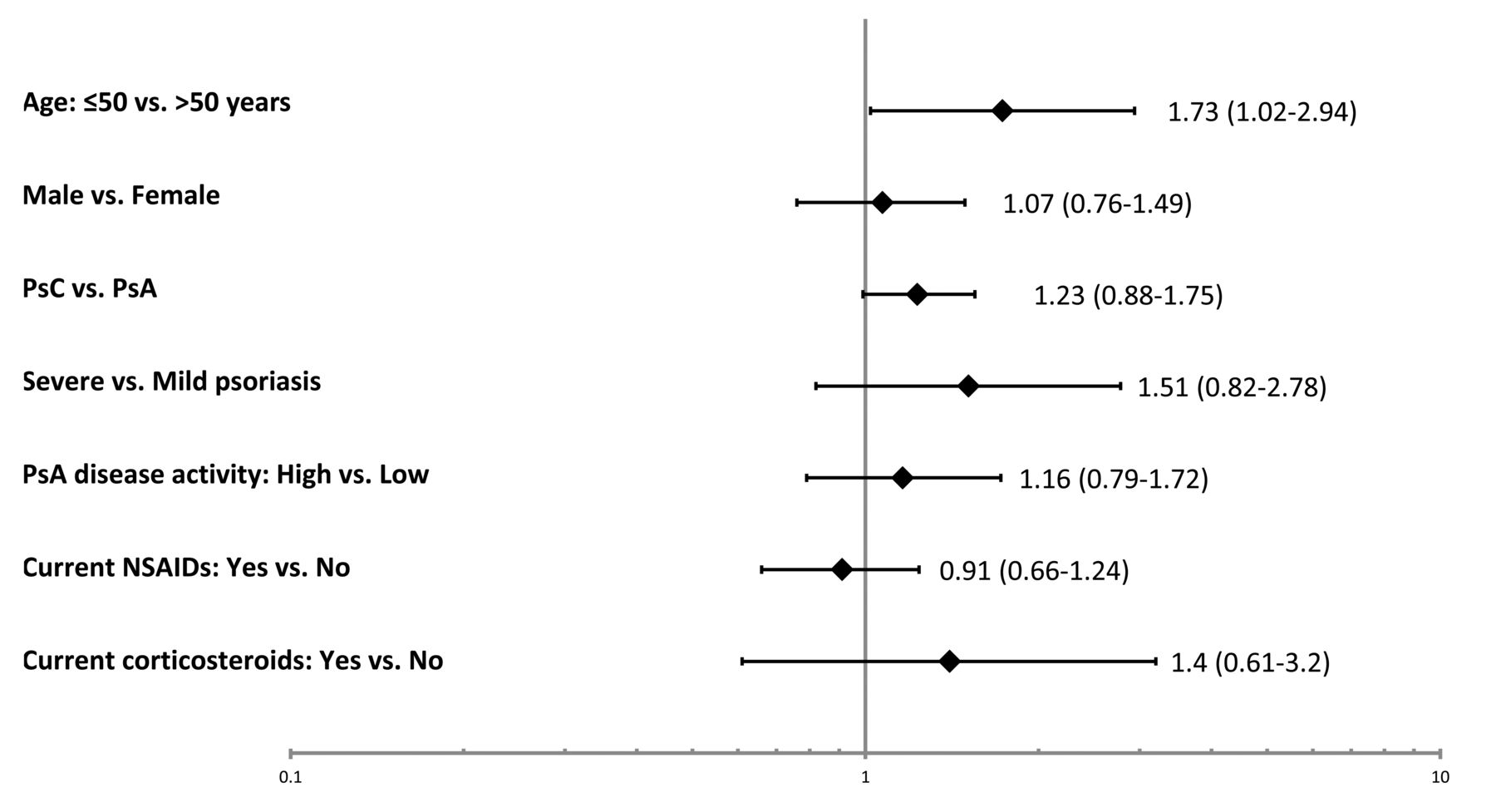
Factors associated with undertreatment of dyslipidemia. Values are OR (95% CI). PsC: psoriasis; PsA: psoriatic arthritis; NSAID: nonsteroidal antiinflammatory drugs.
Sensitivity analysis
Because the Toronto cohort dominated the study population, consisting of over 50% of the study participants, we performed a sensitivity analysis to assess the proportion of underdiagnosis and undertreatment of CVRF by excluding the patients from Toronto. The results were remarkably similar: underdiagnosis and undertreatment of HTN were found in 26.2% and 62.2% of the patients, respectively. Underdiagnosis and undertreatment of dyslipidemia were found in 25.2% and 41% of the patients, respectively.
DISCUSSION
In this large international study, we found a high prevalence of underdiagnosis and undertreatment of HTN and dyslipidemia among patients with psoriasis and PsA. Despite the known association between CV morbidity and psoriatic disease, a significant proportion of the patients with HTN and dyslipidemia were undiagnosed, and among those who had an indication for treatment, suboptimal adherence to treatment recommendations was found. Wide variations in adherence to treatment recommendations for HTN and dyslipidemia were observed across the different sites. These results are in line with studies that found inadequate management of CVRF in patients with psoriasis and other rheumatic diseases that may contribute to the increased CV risk observed in these patients20,22.
In accordance with previous studies, a high burden of CVRF was found in the study population. Of the patients, 87.6% had at least 1 modifiable CVRF and a third of the patients were classified as having high 10-year risk for CV events. Although the increased CV risk in psoriatic disease is partially independent of traditional CVRF, their presence is associated with a higher burden of atherosclerosis and a greater risk of developing clinical CVD7,28,29. Thus, intense control of traditional CVRF is likely the best approach to reduce CV morbidity in psoriatic patients despite the lack of specific primary prevention studies in this population. Observational studies and subgroup analysis of clinical trials suggest that lipid-lowering therapy could reduce CV risk in patients with inflammatory arthritis, supporting efforts to improve control of abnormal lipid levels as an effective measure to reduce CV morbidity30,31.
Gaps in care of CV risk have been extensively investigated in patients with RA; however, only a few studies have assessed this in psoriatic patients. Slightly lower rates of undertreatment of HTN (21.8% untreated, 40.4% not meeting treatment targets) and dyslipidemia (38.6% untreated) were reported in patients with severe psoriasis enrolled in 3 clinical trials22. Jafri, et al reported slightly higher rates of pharmacologic treatment of HTN and dyslipidemia in patients with PsA compared with the general population in a population-based study using administrative data11. However, owing to the design of that study, the rates of underdiagnosis of these risk factors could not be assessed. As we found in our study, underdiagnosis could be high in psoriatic patients (35.7% of patients with dyslipidemia and 23% of patients with HTN). Therefore, the rates of undertreatment of HTN and dyslipidemia in patients with PsA were likely underestimated in the study by Jafri, et al. Our study did not include a control group; however, it could be that even if the level of adherence is similar to the general population, the higher CV risk in psoriatic patients requires special attention to primary prevention of CV events, as per current recommendations for other high-risk populations, such as patients with DM.
Potential explanations for the gaps in screening and management of CV risk in psoriatic patients may include unawareness of the increased CV risk in psoriatic disease, time constraints especially when attention is directed to the management of active psoriatic disease, limited knowledge about CV prevention strategies, and lack of specific guidelines for CV prevention in psoriatic patients. Further, there is disagreement in the rheumatology and dermatology communities about the role of these specialists or family doctors in the management of CVRF for some of the reasons mentioned above32. The factors responsible for this gap in care have been identified in other rheumatic diseases. Studies in RA suggested that awareness of the increased CV risk has not translated into adherence to treatment recommendations20. In our study, we did not find any disease-related factors to explain the gaps in care of HTN and dyslipidemia. However, patients with psoriasis were more likely to be undertreated for HTN and dyslipidemia, although the latter did not reach statistical significance. This finding may suggest different adherence to CV risk management across the 2 specialties, rheumatology and dermatology. Additional factors that were associated with undertreatment included younger age and male sex. It is possible that younger patients who are followed by dermatologists or rheumatologists do not visit primary care physicians as often as older patients do.
Our study provides unique comparative data about CV prevention practices across different countries. Variations were observed in the prevalence of HTN (40.2% to 65.5%), DM (6.9% to 29.6%), dyslipidemia (46.8% to 72%), and smoking (8.6% to 30.9%). The prevalence of overweight and central obesity was markedly elevated across all sites, measuring over 80% in some sites. Differences were also observed in screening and managing HTN and dyslipidemia across the different sites. These variations could reflect differences in ethnicities and genetic susceptibility to CVRF or differences related to healthcare systems and access to care. However, it should be noted that the majority of patients were recruited from specialty clinics in academic medical centers in which a high degree of awareness of CV risk could be expected, thus the gaps in care of patients in community rheumatology and dermatology clinics may be even higher.
Our study has several limitations including the lack of nonpsoriatic controls and the significant proportion of missing lipid profile data, mostly from the 2 US centers, that precluded us from providing a complete assessment of the management of dyslipidemia. As indicated, the study population came mostly from specialty clinics in academic centers, which may limit the generalizability of the results. However, it could be expected that gaps in care are at least similar if not larger in the general population of patients with psoriasis and PsA. Because of the lack of information about fasting glucose or HbA1C, we used a less accurate measure to determine whether a patient has undiagnosed DM, based on nonfasting glucose levels. Only 9 patients (4.9%) were found to have previously undiagnosed DM. More sensitive measures of DM may have revealed a higher prevalence of undiagnosed DM. Additionally, no information was available on the type and dose of lipid-lowering and antihypertensive medications used by the study participants; thus, we could not assess the effect of various treatment approaches on CVRF. Last, by its design, our study did not assess the management of obesity, smoking, and sedentary lifestyle that contribute to CV risk. Given the high proportion of overweight and obesity (> 75%) in psoriatic patients, weight reduction could be another effective measure to manage CVRF.
Our study has several strengths. To our knowledge this is the first study that has assessed gaps in care of CVRF in both patients with psoriasis and PsA. The patients are well phenotyped, allowing us to analyze the association between a variety of disease-related and demographic factors and adherence to treatment recommendations. Last, the study provides data about the prevalence of CVRF and the quality of care of these factors across different populations of psoriatic patients and healthcare systems.
In this large international study, we found significant gaps in screening and treating CVRF in patients with psoriasis and PsA. Additionally, we report a high burden of CVRF in our study population. This high-risk group could benefit from improvement in the screening and management of CVRF to address the gaps in care identified in our study. Although questions exist regarding the optimal treatment targets for CVRF in psoriatic patients, adherence by physicians to, at a minimum, the general treatment recommendations for primary CV prevention is warranted. The high burden of CVRF and the gaps in care observed across all sites highlight the need for new strategies for quality improvement in prevention of CV morbidity in psoriatic patients. Future strategies should consider local resources, type of healthcare systems, and all physicians involved, including dermatologists, rheumatologists, primary care physicians, and cardiologists.
- Accepted for publication October 11, 2017.








{kind=link}
{kind=link}
{kind=link}