

Abstract
Objective. Previous studies combining biologic disease-modifying antirheumatic drugs (bDMARD) to treat rheumatoid arthritis (RA) have shown an increased risk of infection. However, the risk of infection with concurrent use of denosumab, a biologic agent for the treatment of osteoporosis, and a bDMARD remains unclear. Here, we evaluated the incidence of serious and opportunistic infections in patients treated concurrently with denosumab and a bDMARD and patients treated with a bDMARD alone.
Methods. A chart review of patients with RA from 2 Canadian rheumatology practices between July 1, 2010, and July 31, 2014, identified 2 groups of patients: those taking denosumab and a bDMARD concurrently (concurrent group) and those taking only a bDMARD (biologic-alone group). Patients were followed from the time of initiation of denosumab, or a matched index date for the biologic-alone group, to the end of the study or loss to followup. Instances of serious or opportunistic infections were recorded.
Results. A total of 308 patients (n = 102 for the concurrent group and n = 206 for the biologic-alone group) were evaluated. Within the concurrent group, 3 serious infection events occurred. Within the biologic-alone group, 4 serious infection events and 1 opportunistic infection event occurred. In both groups, all patients with serious or opportunistic infection recovered, and there were no instances of death during the study period.
Conclusion. This study demonstrated a low occurrence of serious and opportunistic infections in patients with RA taking bDMARD, including patients with concurrent denosumab use.
Rheumatoid arthritis (RA) is associated with a number of comorbidities, including osteoporosis, which leads to an increased risk of fractures1,2. Many factors contribute to this increased risk of fracture, including a chronic inflammatory state and treatment with glucocorticoids3,4. Given the well-recognized risk of bone loss associated with RA, patients with RA are often given pharmacotherapy for osteoporosis. Oral bisphosphonates have long been the mainstay in the treatment of osteoporosis5. Denosumab, a novel antiresorptive agent used for the treatment of osteoporosis6,7, provides an alternative. Denosumab is a fully human monoclonal antibody that binds to receptor activator of nuclear factor-ϰB (RANK) ligand (RANKL) and blocks the interaction of RANKL with its receptor on the surface of osteoclasts and osteoclast precursors. This leads to a reduction in osteoclast number and activity, a decrease in bone resorption, an increase in bone mass, and a reduction in vertebral and nonvertebral fracture risk1,8.
RANKL is expressed in activated T and B lymphocytes and in lymph nodes; therefore, there is a theoretical possibility that denosumab may increase the risk of infections due to inhibition of the RANK pathway9,10. In the pivotal FREEDOM study8, which assessed the use of denosumab in postmenopausal women with osteoporosis, there was no difference in the overall rates of infection between the denosumab and placebo groups, even though an imbalance in serious skin infections [associated with intravenous (IV) antibiotics or hospitalization] was observed. In addition, earlier studies showed no significant changes in white blood cell counts, overall lymphocyte counts, or lymphocyte subset counts in subjects receiving denosumab, and animal models suggest that immune function remains intact in the presence of RANKL inhibition1,11.
Nonetheless, given the possibility of increased risk of infection among patients treated with denosumab, there is an interest in understanding the safety of using denosumab to treat osteoporosis in patients being treated for RA with other biologic drugs. Previous studies have suggested that exposure to multiple biologic agents, each carrying an independent elevated risk of infection, may be associated with an even higher risk of infection. Two small studies found that the combination of a tumor necrosis factor-α (TNF-α) inhibitor with a second biologic agent, which used another mechanism of action (i.e., anakinra and abatacept, respectively), resulted in higher rates of infection12,13. Given these concerns, the current American College of Rheumatology (ACR) guidelines14 recommend against using biologics in combination for the treatment of RA.
Previous studies that have examined the use of denosumab in combination with other biologic drugs have found no evidence of increased infection risk associated with concurrent exposure8,15,16. In our present study, we used electronic medical records (EMR) and patient charts from 2 academic rheumatology practices in Canada to describe the occurrence of serious infections in 2 groups of patients with RA, specifically, patients with osteoporosis treated concurrently with denosumab and a biologic disease-modifying antirheumatic drug (bDMARD) and patients treated with a bDMARD alone.
MATERIALS AND METHODS
Study cohort
The study population consisted of adult patients with RA being treated with a bDMARD, including a group of patients with moderate to high risk for fracture (as determined by the clinician), who were treated concurrently with denosumab and a bDMARD. The study population was derived from patients from 2 academic rheumatology practices located in Hamilton, Ontario, Canada, between July 1, 2010, and July 31, 2014. The July 2010 inception date was selected because it coincides with the date Health Canada approved the use of denosumab for the treatment of postmenopausal women with osteoporosis at high risk for fracture. Since 2010, the medical records from these rheumatology practices included about 3000 patients taking bDMARD therapy. The diagnosis of RA was based on the clinical judgment of the treating rheumatologist, and this was identified for our study using both clinic notes and International Classification of Diseases codes used for billing purposes. Therefore the ACR classification criteria for RA may not have been applied to all patients.
Information regarding exposure to medications of interest, including start and stop dates, was obtained from the database of the Pharmaca Health Inc. pharmacy, which serves all the patients seen at the rheumatology practices in our study. Other data for the study, including determination of eligibility criteria, patient clinical characteristics, and outcomes, were obtained from review of EMR from the clinics, clinic visit notes, and linked patient data from the pharmacy database. Study approval was obtained from the institutional research ethics board (REB tracking number 14-12-003).
Eligible patients satisfied the following inclusion criteria: ≥ 18 years old with an RA diagnosis; registered in the Hamilton rheumatology medical practices ≥ 3 months before and 3 months after the index date as defined below; and received ≥ 1 injection, or infusion, or filled a prescription for a biologic medication for RA with Pharmaca Health Inc. during the study period. Patients were excluded if they had any of the following: evidence of human immunodeficiency virus or AIDS, treatment for any prevalent cancers, immunosuppressive therapies for conditions other than RA (i.e., organ transplant), or evidence of a nursing home stay.
Initial patient selection focused on the identification of patients who were concurrently exposed to biologic RA medication and denosumab (the concurrent group). Patients in the concurrent group were required to have moderate to high risk of fracture and have received ≥ 1 injection of denosumab while taking a bDMARD in addition to meeting the other eligibility criteria. Conversely, patients receiving only a bDMARD (the biologic-alone group) never received denosumab during the study period. The date of the first denosumab injection while receiving biologic therapy marked the “index date” and served as the start of patient followup for the concurrent group. This served as the index date even if the patient had been treated with a bDMARD before starting denosumab. The index date was required to have occurred between July 1, 2010, and July 31, 2014. Patients in the biologic-alone group were assigned index dates at random to provide comparable followup time to the concurrent group. Patient covariates were collected closest to the index date within 6 months before and/or after the index date. Hospitalizations were monitored 12 months prior to the index date until the end of the study.
The patients in the concurrent group were matched 1:2 to patients receiving solely a bDMARD, and results for the biologic-alone group are presented separately. The index dates for the concurrent groups were stratified based on the year each patient began concurrent therapy. An average index date was obtained for each year (e.g., 2010, 2011, 2012) to provide comparable followup for the biologic-alone group. The biologic-alone patients were randomly selected from the population of patients with RA derived from the 2 rheumatology practices and were then randomly assigned 1 of the average index dates, which also served as their starting point for monitoring patient followup. Patients in the biologic-alone group were required to have initiated biologic therapy prior to their index date, but were not required to have a moderate to high risk for fracture for study inclusion. As with the concurrent group, patient covariates were collected closest to the index date within 6 months before and/or after the index date. Hospitalizations were monitored 12 months prior to the index date until the end of the study.
In both the concurrent and biologic-alone groups, followup began at the index date and continued until the end of the study (July 31, 2014) or loss to followup from the respective Hamilton rheumatology medical practice, whichever came first. Reasons for loss to followup included patient relocation, noncompliance to medication, patient discontinuation of medication, or death. Drug discontinuation was determined using the pharmacy billing records to ensure that the patient filled his or her prescription. The assumption was made that patients were compliant with their medications if they had filled their prescription, unless there was documentation in a patient’s medical records suggesting potential noncompliance. Loss to followup was determined on the basis of specific evidence in the medical records to indicate that any of the criteria for loss to followup had been met; in the absence of such specific evidence, patients were assumed to be in followup and exposed to a bDMARD and denosumab, as relevant.
Exposures
Exposure to a bDMARD was defined as treatment with 1 of the following therapies during the followup period: a TNF-α inhibitor (adalimumab, certolizumab, etanercept, infliximab, or golimumab) or a biologic using another mechanism of action (abatacept, anakinra, rituximab, tocilizumab, or ustekinumab). Exposure to denosumab was defined as receiving ≥ 1 dose of denosumab (60 mg once every 6 mos) during the study period. Pharmaca Health Inc. provided documentation for bDMARD therapy and denosumab injections, including the date administered, dosage, quantity, and any patient reaction(s) to the medications. All data on the medication fill note were transmitted electronically from the pharmacy to the rheumatology practices. The medication history was further confirmed through an examination of the clinic EMR for each patient. Patients in the concurrent and biologic-alone groups at the index date were assumed to have continued their medications up until the end of the study period (July 31, 2014) or until loss to followup, whichever came first.
Outcomes assessment
The primary outcome of interest was the occurrence of serious infections during the followup period. A serious infection was defined as either hospitalization for at least 24 h associated with a primary diagnosis of infection, or an emergency room visit associated with a primary diagnosis of infection and treatment with at least 1 course of IV antibiotics. We reported the number of patients with at least 1 serious infection and the total number of serious infection events during the followup period. The secondary outcome of interest was the occurrence of opportunistic infection, including infection with the following pathogens: Mycobacterium tuberculosis, Mycobacterium avium, cytomegalovirus, varicella zoster virus, herpes simplex virus, Cryptosporidium, Toxoplasma gondii, Cryptococcus neoformans, Pneumocystis carinii, Histoplasma capsulatum, or other invasive fungi.
Outcomes of interest were identified by reviewing hospital discharge summaries in the clinic EMR for all included patients, in addition to reviewing clinic visit notes and any pharmacy queries during the followup period. To ensure events of interest were identified, patients were routinely asked at each clinic visit and by the pharmacy at the time of medication fill if they had been hospitalized. Any discrepancies between patient report and hospital or pharmacy notifications were investigated.
All potential events identified were independently reviewed by 2 internal adjudicators of the outcomes (ANL and JDA). When a disagreement existed between the 2 outcomes adjudicators, a third adjudicator (WGB) was consulted to resolve the disagreement.
Covariates
A number of covariates related to patient demographic, behavioral, and clinical characteristics, as well as details on diagnostic laboratory tests and medication use, were collected at baseline and assessed within 6 months prior to each patient’s index date. Baseline disease activity was collected for both groups, but the analysis did not adjust for differences in baseline disease activity. The information was derived from the rheumatology clinics’ EMR databases, clinic visit notes, and Pharmaca Health Inc. records.
Statistical analysis
The observed frequency of infection was recorded for the concurrent and biologic-alone groups. For both groups, descriptive statistics are presented as means (SD) for continuous and counts (percentage) for categorical variables. The risk of serious infection outcomes was evaluated in terms of the incidence rate per 100 patient-years (95% CI), which was calculated as the total number of infection events divided by the summation of patient-time at risk, where time at risk was censored at the end of the study or end of available followup. The rate of serious infection was separately evaluated in patients using methotrexate (MTX) and prednisone, given that both these medications may increase the rate of infection in this patient population and are potential confounding variables. Differences between incident rates were calculated using MedCalc Statistical Software version 14.12.0 (MedCalc Statistical Software BVBA) and descriptive statistics were summarized using SAS version 9.3 for Windows (SAS Institute Inc.).
RESULTS
We identified 191 patients who had a history of being treated with bDMARD therapies and denosumab. After excluding patients based on technical limitations (e.g., no patient data available in the clinic EMR) and applying the inclusion and exclusion criteria, 102 patients were identified for the concurrent group (Figure 1). After matching patients based on the derived index dates for patients in the concurrent group, 206 patients were identified for the biologic-alone group.
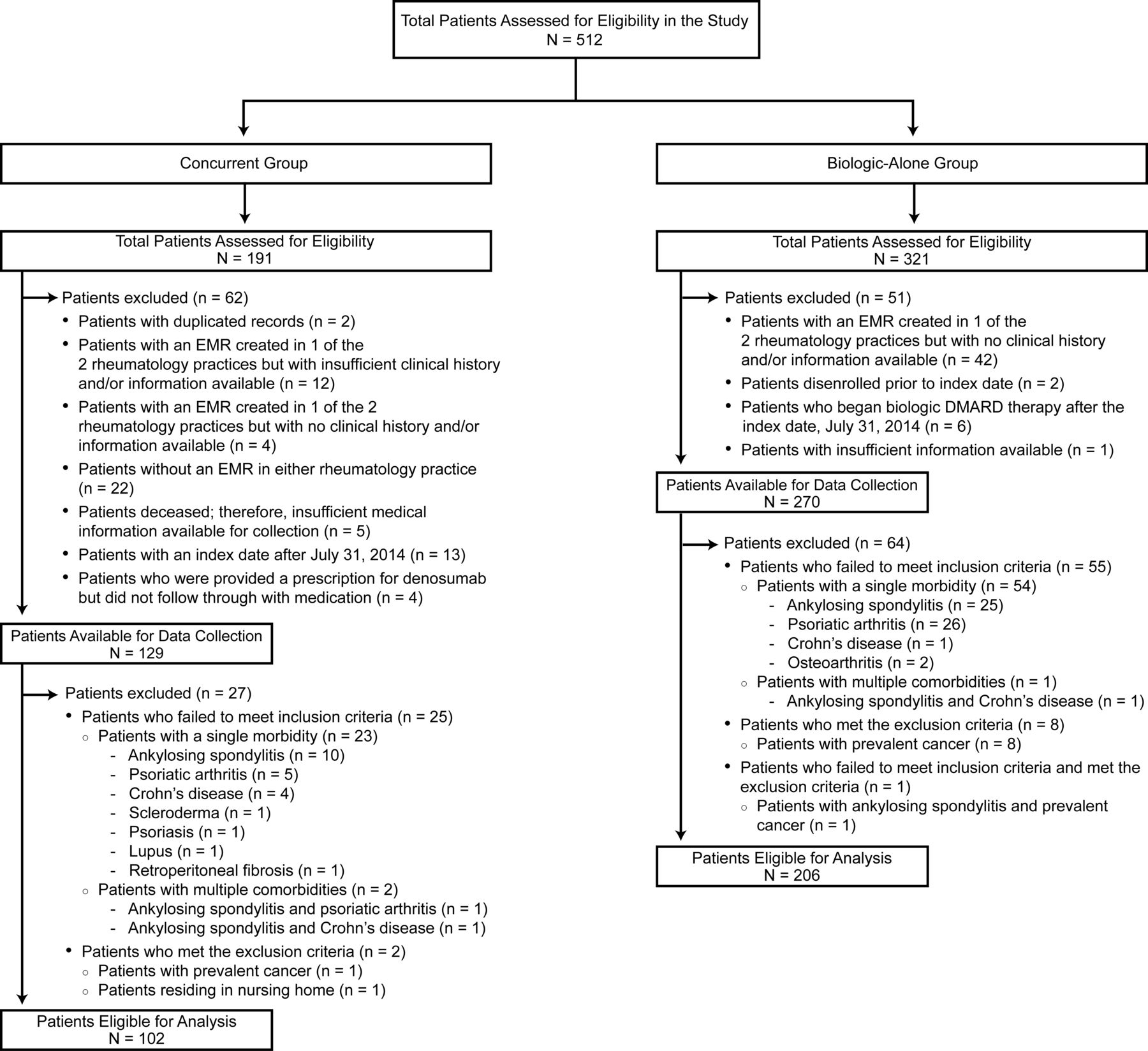
Flowchart of patient eligibility. DMARD: disease-modifying antirheumatic drug; EMR: electronic medical record.
Participant characteristics for both groups are provided in Table 1. Compared with patients in the biologic-alone group, concurrently exposed patients were more likely to be female and of older age. Concurrently exposed patients were also more likely to have a bone mineral density T score in the osteoporotic range and a history of fracture. Patients in the biologic-alone group had a higher frequency of cardiovascular disease, chronic obstructive pulmonary disease (COPD), and diabetes.
Participant characteristics. Data recorded within ± 6 months of the index date. Data are means (SD) unless otherwise noted.
Descriptive statistics pertaining to biologic and conventional DMARD use are provided in Table 2. Patients in the biologic-alone group had a higher frequency of MTX use and those in the concurrent group had a higher frequency of prednisone use. Rates of infection are provided in Table 3. Regarding the primary outcome, there were 3 serious infection events among the 102 patients in the concurrent group, and 4 serious infection events and 1 opportunistic infection event among the 206 patients in the biologic-alone group. The rates of serious or opportunistic infections were 1.22 per 100 patient-years (95% CI 0.25–3.56) in the concurrent group and 0.98 per 100 patient-years (95% CI 0.32–2.29) in the biologic-alone group (rate difference 0.24, p = 0.77). The most common type of infection was pneumonia (n = 6).
DMARD composition within the concurrent and biologic-alone groups. Data are shown as n (%) of patients, unless stated otherwise.
Incidence of serious and opportunistic infections within the concurrent and biologic-alone groups.
A subgroup analysis was performed examining rates of serious infection associated with MTX and prednisone use. Event rate per 100 patient-years was 0.83 (95% CI 0.02–4.60) in the concurrent group and 0.30 (95% CI 0.00–1.67) in the biologics-alone group among MTX users (rate difference 0.53, p = 0.46), 5.56 (95% CI 1.15–16.24) in the concurrent group and 3.30 (95% CI 0.08–18.57) in the biologics-alone group for prednisone users (rate difference 2.22, p = 0.65), and 4.55 (95% CI 0.12–25.33) in the concurrent group and 0.00 (95% CI 0.00–16.77) in the biologics-alone group for MTX and prednisone users combined (rate difference 4.55, p = 0.32).
DISCUSSION
Our present study showed that, in a real-world setting, the occurrence of serious infections was low in patients with RA treated concurrently with a bDMARD and denosumab, and in patients treated with a bDMARD alone. These results are consistent with those from previous retrospective cohort studies assessing infection rates in patients with RA treated concurrently with denosumab and a bDMARD17,18.
A retrospective cohort study using the US Medicare administrative claims database19 analyzed data from 5814 patients with RA to compare the rates of hospitalized infection in patients receiving denosumab concurrently with a bDMARD with those of patients receiving zoledronic acid concurrently with a bDMARD. The investigators specified an a priori noninferiority margin to compare the 2 groups and found that the rate of hospitalized infection was not greater among patients using denosumab [14.9 per 100 patient-yrs (95% CI 12.2–18.1)] compared with those using zoledronic acid [13.9 per 100 patient-yrs (95% CI 12.5–15.4)]19. It is important to note that in that study, patients within both groups may have experienced more than 1 infection in a single hospitalization, and in contrast to our study, patients may have had repeated infections. Further, the population in the study by Curtis, et al19 had higher percentages of comorbidities (e.g., diabetes and COPD) compared with our study population. Finally, over 50% of patients within both exposure groups in the study population in Curtis, et al19 used infliximab, which has been shown to result in a higher risk of infection compared with other bDMARD20,21. In comparison, our study population had a balanced use of bDMARD among patients in both the concurrent and biologic-alone groups. While the results of Curtis, et al19 are in agreement with our finding that there was no observed increased risk of hospitalized infection among patients treated concurrently with a bDMARD and denosumab, the above combined factors may have contributed to a greater incidence rate per 100 patient-years in their study compared with our findings.
Another study reported a higher rate of serious infections in 10 patients treated concurrently with denosumab and a bDMARD compared with rates in patients taking either denosumab (n = 159) or a bDMARD (n = 193) alone22. Interpretation of this result, however, is limited by the small number of concurrent users as well as the minimal information available on the patient populations including covariates and risk factors, duration of followup, and the time at risk in the different treatment groups. Further, the authors did not adjust their analyses for age, which is a known risk factor for infection. A previous Canadian prospective cohort study (RHUMDATA) of patients with RA found an increase in the infection rate in patients treated with denosumab alone (25.0 per 100 patient-yrs) versus those treated with denosumab in addition to a bDMARD (15.7 per 100 patient-yrs)23. However, the sample size in that study was also limited (n = 20 patients in the combination group; n = 43 in the denosumab-alone group), and no adjustment was made for potential confounding factors.
Access to detailed clinical information is a strength of our study, which provides a unique evaluation of a cohort of patients with RA in a real-world clinical practice setting. Previous studies have used large administrative databases or RA registries that provide large sample sizes, but often do not provide enough information regarding potential events of interest to confirm the occurrence and severity of such events. In our study, the patients’ full medical records were used to gather details surrounding potential events of interest. Further, patients taking a bDMARD were routinely asked about recent infections, hospitalizations, and use of antibiotics at each clinic visit, which maximized the total number of events identified. In addition, having 2 designated adjudicators of outcomes allowed for consistency and reproducibility of the adjudication of outcomes of interest.
The results of our study should be interpreted in light of particular limitations. First, the relatively small sample size and short followup duration may have contributed to the low number of events observed in both groups. Because of our limited sample size, the study was underpowered to detect differences between groups, and the interpretation of nonsignificant results should be viewed with caution. No adjustment was made for any observed imbalances in potential confounders, such as age and comorbidities, between the groups. A history of serious infections, which could be an important prognostic factor, was not uniformly available and hence not assessed. Additionally, we did not have information on the duration of prior exposure to biologics or denosumab, both of which might also influence risk of serious infection. We acknowledge that there are differences in missing data such as fractures and BMD in the biologics alone group. This may well explain the lack of osteoporosis treatment in this group. However, our findings suggest that the incidence of serious infections was low in both groups. The clinics that contributed patient data to our study are highly vigilant regarding vaccination protocols and counseling patients to stop their bDMARD in response to impending signs of infection; therefore, the observed rates of infection may have been lower than those in other clinic populations with different practice standards. Further, as a result of such proactive patient monitoring, infections occurring in this patient population may have been less likely to require hospital admission or IV antibiotics in the emergency room, thereby lowering the number of serious infections observed. Finally, event rates may have been underreported, especially given the definition of a serious infection in our study. This is a general limitation to retrospective studies in general, and is also applicable to our study.
Results from our study suggest that few patients with RA concurrently treated with a bDMARD and denosumab had serious infections or opportunistic infections. The small number of infections observed is consistent with that reported in previous cohort studies and provides additional evidence of the safety of concurrent treatment with denosumab and a bDMARD. Future studies using larger cohorts could shed further light on this important question.
Acknowledgment
Lisa A. Humphries, PhD, of Amgen Inc. and Martha Mutomba (on behalf of Amgen Inc.) provided editing, formatting, and submission support.
Footnotes
Dr. William G. Bensen died March 15, 2017.
Full Release Article. For details see Reprints and Permissions at jrheum.org
Amgen Inc. funded this study. A.N. Lau has received consulting fees, speaking fees, and/or honoraria from Amgen Inc. W.G. Bensen received consulting fees, speaking fees, and/or honoraria from Amgen Inc. J.D. Adachi has received consulting fees, speaking fees, and/or honoraria from Amgen Inc. S. Wade has received consulting fees from Amgen Inc. L. Spangler, A. Balasubramanian, and N. Pannacciulli are employees of Amgen Inc. and have received Amgen Inc. stock and/or stock options. C.J. Lin is a former employee of Amgen Inc. and has received Amgen Inc. and Genentech/Roche stock and/or stock options.
- Accepted for publication August 11, 2017.
Free online via JRheum Full Release option








{kind=link}