

Abstract
Objective. To test the sensitivity to change of the Outcome Measures in Rheumatology Clinical Trials (OMERACT) ultrasound (US) scoring system for tenosynovitis when applied in a multicenter design.
Methods. RA patients with US-verified tenosynovitis were recruited when scheduled for treatment intensification. Tenosynovitis was assessed at baseline, and 3 and 6 months followup, using the semiquantitative OMERACT scoring system.
Results. Expressed in median (25th; 75th percentiles), the overall greyscale and Doppler score decreased significantly from baseline at 4 (2; 7) and 3 (2; 6), to 6 months at 2 (0; 3) and 0 (0; 1, p < 0.01), respectively, and showed high responsiveness (standardized response mean ≥ 0.8).
Conclusion. The OMERACT US scoring system for tenosynovitis showed high responsiveness, supporting its use for diagnosing and monitoring tenosynovitis in multicenter trials.
Tenosynovitis is a very common disease manifestation in patients with rheumatoid arthritis (RA)1,2. It has been associated with lower physical function3 and may be one of the best imaging predictors for early development of RA2,4,5. Several studies have confirmed the limitations of clinical examination for detection of tenosynovitis in comparison with ultrasound (US)6,7,8, and a highly validated and reliable US scoring system is therefore needed if implementing US-tenosynovitis as an outcome measure in clinical trials. In 2012, the Outcome Measures in Rheumatology Clinical Trials (OMERACT) US group proposed a new tenosynovitis scoring system9. Good single- and multicenter intra/interobserver agreement (k = 0.66–0.84/0.48–0.68) among the sonographers in this study and good sensitivity to change in single-center design has been reported using this OMERACT system, whereas the sensitivity to change in a multicenter design has never been tested. Studies have shown that US low-grade synovial hypertrophy without Doppler signal is common in RA6,10, but whether it represents true inflammation (i.e., can be eliminated by antiinflammatory therapy) is being debated.
The primary aim of our study was therefore to test the sensitivity to change of the OMERACT US scoring system for tenosynovitis in a multicenter design to validate it as an outcome measure in RA multicenter clinical trials. Second, we aimed to investigate whether tendon sheaths with minimal signs of inflammation (low-grade synovial hypertrophy without Doppler signal) improved during therapy. Finally, the association between US scores, and clinical disease activity and physical disability was investigated.
MATERIALS AND METHODS
Patients with RA from 6 rheumatology outpatient clinics in 4 countries (Denmark, France, Italy, and Spain) with US-verified tenosynovitis were recruited if they were scheduled for treatment intensification with conventional synthetic (cs) disease-modifying antirheumatic drug (DMARD) and/or biological (b)DMARD. The hand or foot with the most affected tendon sheaths on US was chosen at baseline and all tendon sheaths in that region were assessed at baseline, and 3 and 6 months followup. The following tendon sheaths were selected for assessment in the wrist and hand: abductor pollicis longus, extensor pollicis brevis, extensor carpi radialis longus, extensor carpi radialis brevis, extensor pollicis longus, extensor indicis and digitorum communis, extensor digiti minimi, extensor carpi ulnaris, flexor carpi radialis, flexor pollicis longus, and flexor digitorum superficialis, and flexor digitorum profundus. The following were selected in the ankle and foot: tibialis anterior, extensor hallucis longus, extensor digitorum longus, peroneus longus, peroneus brevis, tibialis posterior, flexor digitorum longus, and flexor hallucis longus. The study was conducted in accordance with the Declaration of Helsinki and each participant gave written informed consent. The study was assessed by the national or local committees on health research and no ethics approval for this type of study was needed.
Ultrasound
A General Electric Logiq E9, or a MyLab Twice US unit with a high frequency linear probe (6–15 MHz or 6–18 MHz) was used. Color (CD) or power Doppler (PD) were used depending on which Doppler modality was the most sensitive on the individual machines11. The Doppler settings were adjusted in each clinic according to published recommendations12. Tenosynovitis in the selected hand/foot was assessed by greyscale (GS) and CD/PD using the OMERACT semiquantitative scoring system9. This scoring system includes a 4-grade semiquantitative scale for GS (i.e., grade 0, normal; grade 1, minimal; grade 2, moderate; grade 3, severe) and Doppler (i.e., grade 0, no intratenosynovial Doppler signal; grade 1, focal intratenosynovial Doppler activity; grade 2, multifocal intratenosynovial Doppler activity; grade 3, diffuse intratenosynovial Doppler activity) with an average time consumption of 20 s for each tendon sheath6.
Clinical/biochemical parameters and patient-reported outcomes
An overall patient-reported visual analog scale (VAS) tenosynovitis pain score from 0 to 100 mm of the most affected hand/foot was performed at all visits. The 28-joint Disease Activity Score [DAS28, based on C-reactive protein (CRP)], patient global VAS, CRP, and Health Assessment Questionnaire (HAQ), were evaluated, blinded for the US results for each visit.
Statistical analysis
Data were analyzed using 2-sided Wilcoxon signed-rank test for paired data, with p value < 0.05 considered significant. For GS and Doppler calculations, the sum score on patient level was used. Sensitivity to change was calculated using the standardized response mean (SRM) as follows: trivial < 0.20; small, 0.20–49; moderate, 0.50–79; or good, ≥ 80. The association between change in GS/Doppler score, and DAS28 and HAQ was assessed by a mixed model for repeated measurement. Owing to the small sample size (67 patients) seen at 3 timepoints, only 2 variables (DAS28 and HAQ) were chosen.
RESULTS
There were 68 patients with RA included. Of these, 63 completed the study, 4 dropped out before 6 months by withdrawing informed consent; 1 patient did not meet the inclusion criteria and was excluded from the data analyses. Fewer than 3.5% of the data were missing and therefore no data imputations were made.
The most common baseline tenosynovitis locations were extensor carpi ulnaris (ECU), involved in 70.7% of the assessed hands, and tibialis posterior tendon, involved in 44.4% of assessed ankles.
Intensification with bDMARD was initiated in 58% of the patients at baseline and the treatment was intensified in only 6% of the patients during the study. Further baseline characteristics of the patients, baseline distribution of tenosynovitis, and treatment are presented in Table 1, Figure 1, and Supplementary Table 1 (available with the online version of this article).
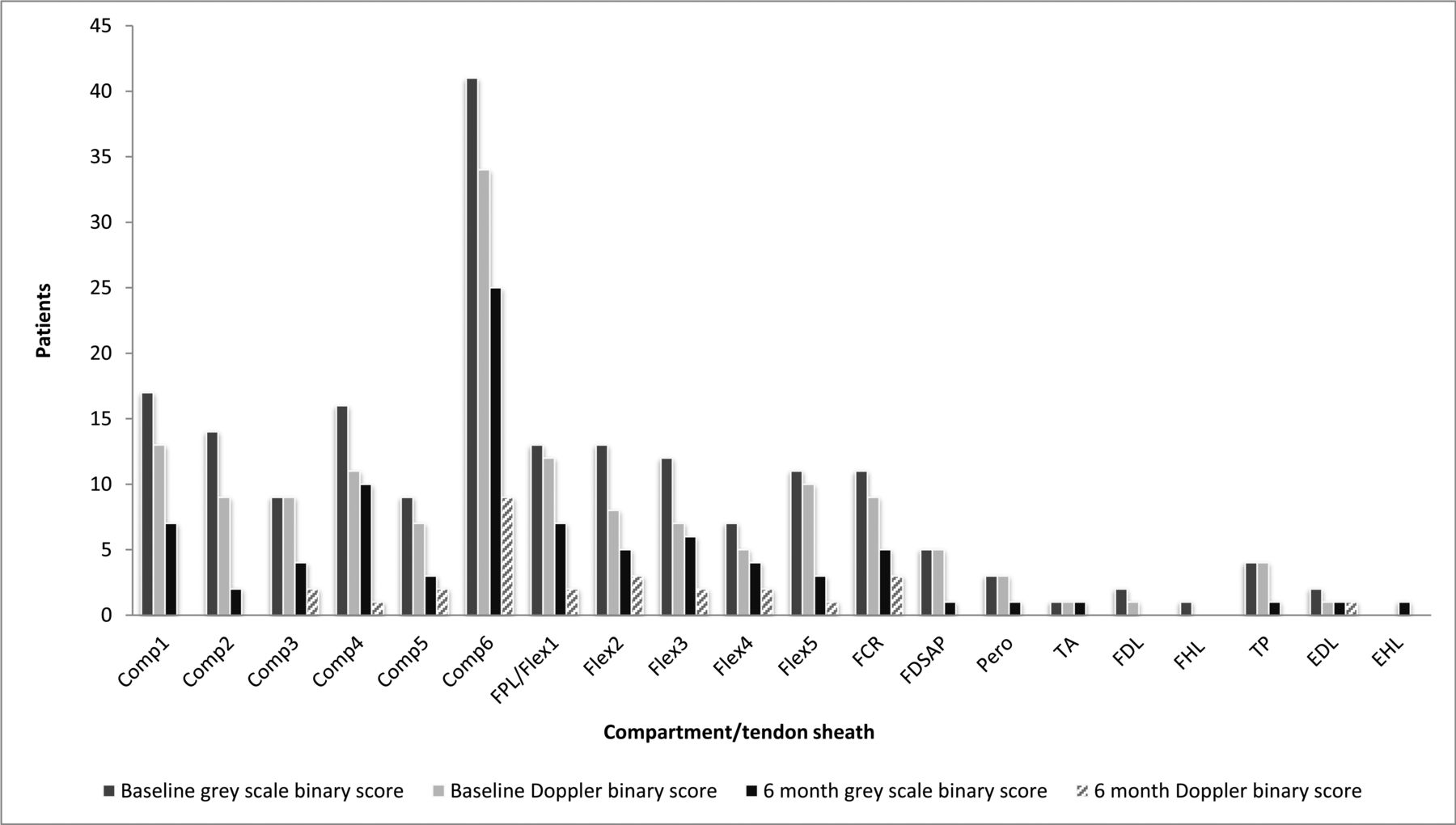
Baseline distribution of tenosynovitis. Comp1: abductor pollicis longus and extensor pollicis brevis; Comp2: extensor carpi radialis longus and extensor carpi radialis brevis; Comp3: extensor pollicis longus; Comp4: extensor indicis and extensor digitorum communis; Comp5: extensor digiti minimi; Comp6: extensor carpi ulnaris; FCR: flexor carpi radialis; FPL/Flex1: flexor pollicis longus/1 flexor tendons of the digits; FDSAP: flexor digitorum superficialis, and flexor digitorum profundus; Flex2: 2 flexor tendons of the digits; Flex3: 3 flexor tendons of the digits; Flex4: 4 flexor tendons of the digits; Flex5: 5 flexor tendons of the digits; Pero: peroneus longus and brevis tendons; TA: tibialis anterior tendon; EHL: extensor hallucis longus tendon; EDL: extensor digitorum longus tendon; TP: tibialis posteriortendon; FDL: flexor digitorum longus tendon; FHL: flexor allucis longus tendon.
Demographics, and clinical and laboratory characteristics of patients. Values are n (%) or mean ± SD unless otherwise specified.
Sensitivity to change
The overall GS and Doppler score decreased significantly (p < 0.01) from baseline to both 3 and 6 months and was highly responsive (SRM ≥ 0.8), in line with changes in clinical variables and patient-reported outcomes (p < 0.01, Table 2). The most pronounced change in outcome variables was seen between baseline and 3 months, with global VAS being the most responsive score (SRM = 1.2). The outcome changes on site level are presented in Supplementary Tables 2, 3, and 4 (available with the online version of this article).
Change in tenosynovitis ultrasound scores, DAS28, HAQ, CRP, and patient-reported outcomes, and their SRM, during 6 months of followup for all patients. Values are mean ± SD or median (IQR: 25; 75 percentile).
The responsiveness of tenosynovitis scoring was higher (1.3 for both greyscale and Doppler) in patients with early RA (< 1 yr) than in established RA (0.7 and 0.8 for greyscale and Doppler, respectively). Patients who had been initiated on csDMARD or bDMARD had an SRM of 0.8 and 0.9, and 0.8 and 1.0 for greyscale and Doppler, respectively. Numerically, slightly higher responsiveness (1.2 and 1.3 for greyscale and Doppler, respectively) was observed when a combination of csDMARD and bDMARD was initiated.
Responsiveness of Doppler-negative tenosynovitis
At baseline, 39 tendon sheaths had GS = 1 and Doppler = 0. Only 3 of these tendon sheaths did not respond to treatment (i.e., remained unchanged during the 6-month observation period). Only 2 tendon sheaths with Doppler = 0 at baseline had a GS > 1 and both changed to GS = 1 and Doppler = 0 at both 3 and 6 months.
US association with clinical variables of overall disease and of tendon sheath involvement
Changes in GS and Doppler were not associated with changes in HAQ (p = 0.6–0.7) but with changes in DAS28 (both p = 0.02), using a mixed model for repeated measurement.
DISCUSSION
To our knowledge, this report is the first to test the OMERACT US tenosynovitis scoring system in a multicenter followup study. The OMERACT scoring system had high responsiveness, (i.e., the SRM was high at > 0.8), when treatment intensification as a result of increased disease activity was initiated among RA patients with US-verified tenosynovitis.
The incidence and pattern of tenosynovitis were comparable to previous studies6,13,14,15,16,17, and ECU was the most frequently occurring tenosynovitis, independent of RA disease duration, as in earlier studies.
In tendon sheaths without Doppler signal, 92.3% of positive GS scores responded to treatment (i.e., decreased in score). These results show that in established RA, minimal tenosynovial hypertrophy can respond to treatment, and thereby reflect true inflammation.
A significant association was found between change in US scores and DAS28, as previously detected in some but not in other previous studies18,19. Changes in US scores were not associated with changes in HAQ, as previously seen in a single-center study6. A significant association between HAQ and magnetic resonance imaging (MRI)-detected tenosynovitis has formerly been shown in early RA cohorts3,20. The different disease durations of the US and MRI cohorts most likely explain this difference, because permanent disability is more frequent among patients with established RA, making the HAQ score less responsive.
US assessment systems of tenosynovitis have previously been investigated6,7,9,13,16. In our multicenter study, both GS and Doppler scores decreased significantly from 0 to 6 months, in agreement with previous single-center studies6. Because it is now documented that the OMERACT US tenosynovitis scoring system has an excellent intra- and inter-reader agreement among trained investigators6,9 and a substantial ability to detect change over time in both the single-center6 studies and our multicenter study, it has the potential to be implemented as an outcome measure in future multicenter clinical trials. Because tenosynovitis is a common disease manifestation for patients with RA and may predict erosive development20, but is also difficult to assess appropriately by clinical examination, this finding is highly relevant.
A minor limitation is that the OMERACT US tenosynovitis scoring system has been tested only by the developers and very experienced ultrasonographers.
Our RA multicenter study documents a high responsiveness of both OMERACT GS and Doppler tenosynovitis scores. Further, low-grade GS tenosynovitis, even in tendon sheaths without Doppler activity, is responsive to treatment. Finally, the OMERACT US tenosynovitis score was associated with DAS28 but not with HAQ. Our data support the use of the OMERACT US scoring system for diagnosing and monitoring tenosynovitis in multicenter trials.
ONLINE SUPPLEMENT
Supplementary material accompanies the online version of this article.
- Accepted for publication September 8, 2017.








{kind=link}