

Abstract
Objective. To identify and address patient-reported barriers in osteoporosis care after a fracture.
Methods. A longitudinal cohort of fragility fracture patients over 50 years of age was seen in a provincewide fracture liaison service. Followup interviews were done at 6 months for osteoporosis care indicators. Univariate statistics were used to describe baseline characteristics, osteoporosis-related outcomes, and reasons cited for not achieving them. Two phases of this program were compared (Phase I: education and communication, and Phase II: risk assessment education and communication). Phase II was further divided into those who fully participated and those who declined.
Results. Phase I (n = 3997) had lower testing and treatment rates than Phase II (n = 1363). Rates were highest in those confirmed as having participated in Phase II (n = 569). Phase II nonparticipants (n = 794) had results as in Phase I. In Phase I, the main patient-reported barriers for not visiting their physician or not having a bone mineral density (BMD) test were patient- and physician-oriented (e.g., being instructed by their physician to not have the BMD test). In Phase II, BMD testing was part of the program, thus the main barriers were around treatment choices. Phase II eligible nonparticipants experienced many of the same barriers as Phase I patients, with lower BMD testing rates (54.9% and 65.4%, respectively).
Conclusion. Evaluating and addressing barriers to guideline implementation reduced those barriers and was associated with higher downstream treatment rates. Monitoring barriers in a program like this provides useful insights for program changes and research interventions.
International clinical guidelines agree that persons over 50 years of age with a fragility fracture should have a fracture risk assessment completed, which usually requires bone mineral density (BMD) testing, and if indicated, be considered for bone-sparing mediations with proven fracture reduction benefit1,2,3. Uptake of these guidelines continues to be poor, with Solomon and colleagues4 reporting a low and declining trend in osteoporosis treatment after hip fracture between 2002 and 2011.
Fracture liaison services (FLS) have emerged as efficacious5,6,7,8 models of care for improving attention to osteoporosis after a fracture, with superior results when compared to education-based models5,6,9. However, even these coordinator-based interventions fall short of assessment and treatment targets, creating gaps in their potential to reduce the refracture risk in these higher-risk patients. Refractures are associated with elevated mortality, morbidity, and healthcare costs10,11,12. Identifying barriers to the implementation of guidelines can lead to more accurate targeting of interventions, thereby effecting change toward optimal practice and better care13,14. Barriers to effective fracture prevention have been studied at the level of the healthcare system15. However, important barriers to effective osteoporosis management can be found at the level of the patient as well. As noted by Majumdar, et al16, patient-level factors have been relatively understudied, and the patient perspective is particularly important in the clinical setting, where an acute fracture event may represent an important “teachable moment.”
In Ontario (population 14.4 million17), Canada, the Fracture Clinic Screening Program (FCSP) was initiated as an FLS in 2007 and has currently placed fracture prevention coordinators (FPC) in 37 fracture clinics around the province. Experience has shown the importance of the patient as an agent of change, be it in terms of attending appointments, adhering to medication, or advocating for bone health6,16,18,19, and as a result, the FCSP and its evaluations have taken a strong patient-centered approach16,18,20.
In the original program (Phase I), the coordinator’s function included case finding, educating, and liaising with primary care, who assumed responsibility for testing, risk assessment, and treatment (if indicated). In June 2012, the hospital sites began shifting to an additional role for the coordinator, that of ordering BMD tests and communicating the results, the calculated refracture risk, and the relevant guideline material back to the primary care providers (PCP). In this new program, all the educational and liaison functions of the first phase continued. Phase II was initiated at a site as soon as the negotiations supporting this role were complete, and it was staggered over 16 sites during our study period (June 2011–November 2014). In all cases, quality assurance data were gathered by the FPC at baseline and 6 months after screening to record testing and treatment initiation rates, as well as to assess barriers for the achievement of these outcomes13,21. The barriers were specifically gathered to allow for insights that could improve access and uptake of guideline-based care in this population. The purpose of our study was therefore to report on the barriers to bone health testing and treatment from the perspectives of patients in Phases I and II of the FCSP, and to align the barriers with osteoporosis-related outcomes by the different phases of the program.
MATERIALS AND METHODS
The study population consisted of a longitudinal cohort of fragility fracture patients (> age 50, low-energy fracture) who were not tested for osteoporosis in the year prior to screening and not treated for osteoporosis. Cases were identified through case-finding activities (e.g., electronic or paper chart review) of the FPC embedded in 35 hospital fracture clinics in our province between June 2011 to November 2014. FPC spoke to eligible patients, usually at their first clinic visit postfracture, and confirmed whether they were fragility fractures and over age 50; if so, they were then invited to participate in the FCSP program. The samples included in this analysis were a total of 4360 persons who were screened from June 2011 to November 2014, and were successfully contacted for a 6-month followup to assess BMD testing and treatment status. The 6-month time frame has been recommended for quality indicators in this field22 to prevent refracture within the vulnerable first year. Phase I (educational and liaison role) and Phase II (additional role of ordering BMD and communication of completed risk assessment) overlapped in this time period. In total, 16 hospitals transitioned to a Phase II program over our period of study and contributed to our sample. Within Phase II of the program, 2 subgroups emerged. First, the eligible persons who participated in the additional role of the FPC and had their testing arranged and communicated to their PCP (named Phase II: Confirmed Participants), and second, a group who declined this additional role, preferring to have their PCP manage this. The second group was called “Phase II: Eligible, Nonparticipants” and received equivalent to Phase I educational/liaison model of care.
Deidentified interviewer-administered surveys gathered on secure servers through zero-footprint tablets for quality assurance and program evaluation purposes were used for this study. All data were gathered by the patient’s FPC. Approval for use of the quality assurance data for research purposes was provided by the Research Ethics Board at St. Michael’s Hospital (REB# 13-156).
The variables used in this analysis included sociodemographics (age, sex, and fracture location), osteoporosis-related outcomes, and the reasons why patients were not initiating osteoporosis testing or taking their prescribed treatment. Self-reported osteoporosis-related outcomes of interest included BMD testing (had a BMD test done at followup), treatment initiation (being prescribed medication for osteoporosis, osteopenia, or bone health at followup), and medication (currently taking the medications prescribed for osteoporosis, osteopenia, or bone health at followup).
When patients responded as not having initiated testing or indicated they were not taking their prescribed medication at followup, their reported reasons were recorded in multiple-choice options (or open-ended text boxes for less-frequent responses). For example, those reporting not having a BMD test done were asked about making the appointment with the physician and also about reasons for not having had the test (including if it was coming up or they were told they did not need one). All reasons were based on the patient’s perception. All options offered to patients are listed in the Results section.
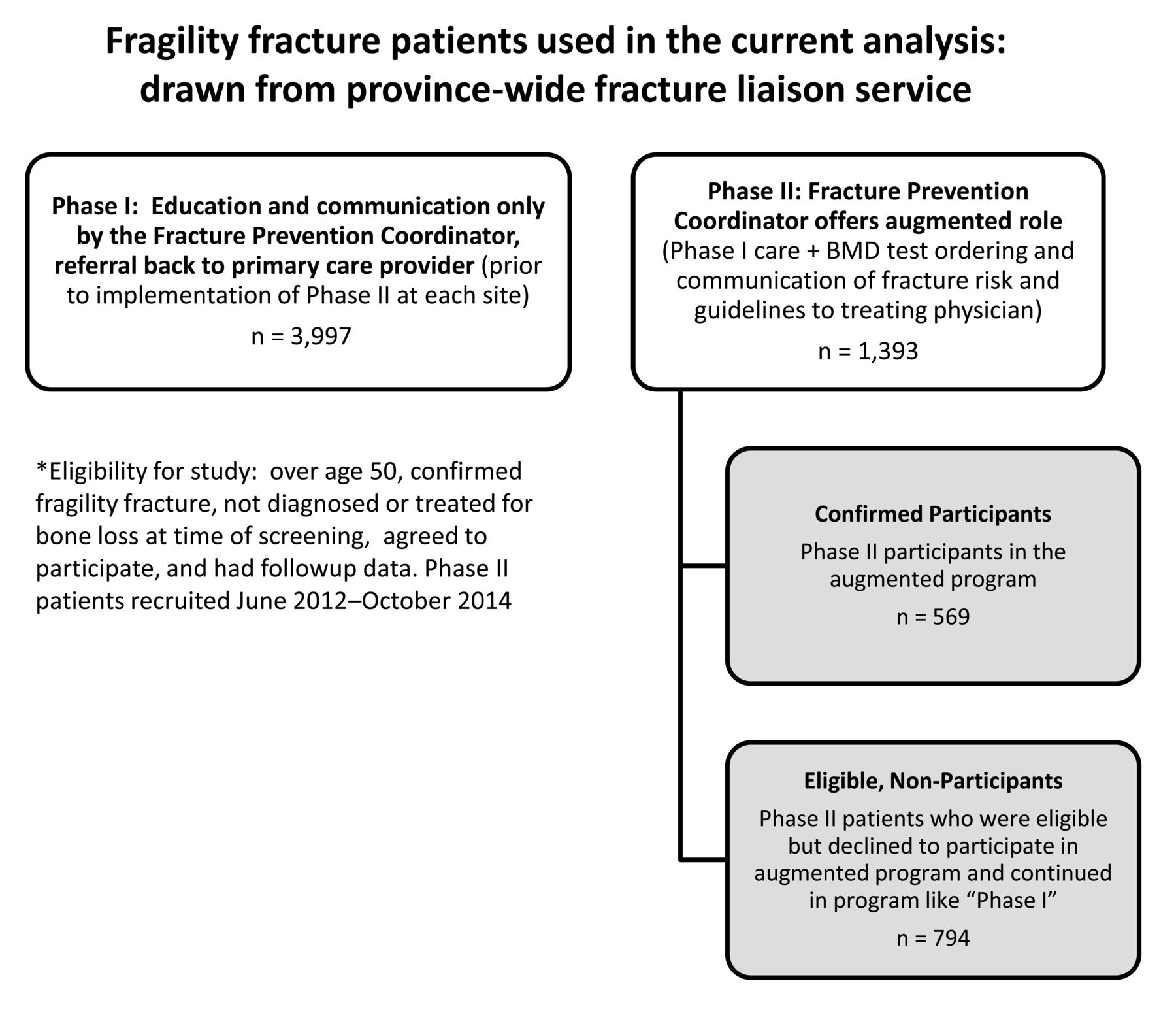
Univariate statistics were used to describe baseline characteristics, osteoporosis-related outcomes, and reasons cited for not achieving them. Comparisons were made using Fisher’s exact test and a p value for statistical significance of 0.05. We considered any quantified difference of < 5–10% to be likely of little clinical importance. We then subdivided Phase II participants into those confirmed as having participated (Confirmed Participants) and the Eligible Nonparticipants, allowing a comparison with those who actually experienced the change in program (Phase II Confirmed Participants) and those who had more of a Phase I experience in their fracture screening program care (Phase II Eligible Nonparticipants; Figure 1).
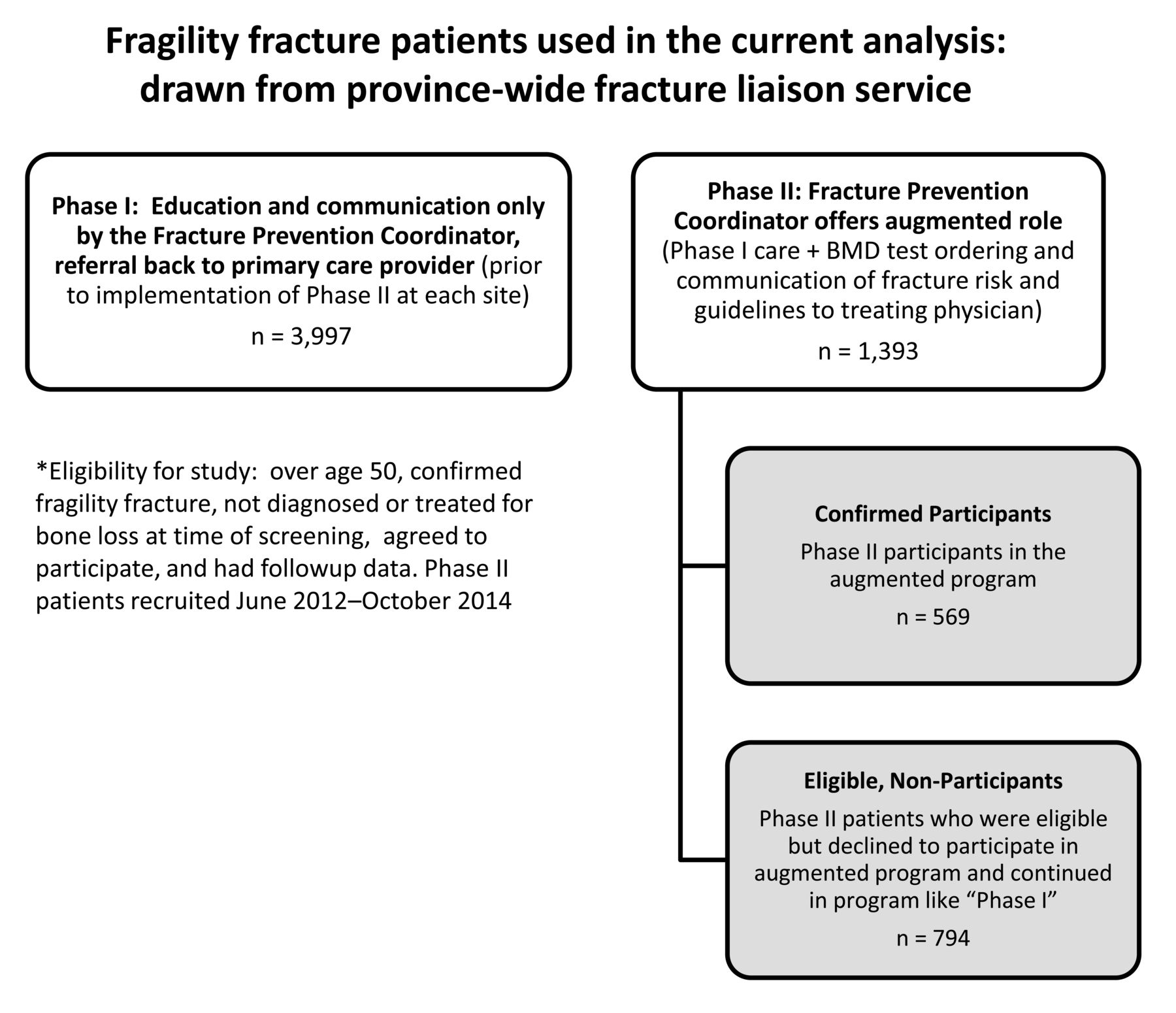
Source of the data used in this analysis. Two overlapping cohorts of Phase I patients moving through a program of education and facilitated communication. Phase II patients had this plus BMD testing by the coordinator, who relayed the reported results back to primary care. Phase II further divided those who participated in this augmented program (Confirmed Participants) and those who declined and received a Phase I type program of care (Eligible Nonparticipants). BMD: bone mineral density.
RESULTS
Study population
Phase I included 3997 patients over 50 years of age who sustained a fragility fracture, did not have treatment for osteoporosis, did not undergo BMD testing in the last year, had a PCP, and had followup data within 6 months of screening. Phase I patients had a mean age of 68.5 years. Nearly 78% were female and the wrist was the most commonly reported fracture location (Table 1). Phase II included 1363 patients (mean age 67.9 yrs, 73.1% female) who met all the same criteria as in Phase I but were screened at sites after the start of BMD testing and risk assessment within the program. In Phase II, there were 569 participants who we confirmed as having fully participated in the addition of BMD testing and risk assessment within the program (Confirmed Participants) and 794 eligible nonparticipants who did not have their testing done within the screening program (Eligible Nonparticipants). The latter group was comparable to patients in Phase I in terms of sociodemographics (Table 1). Persons enrolled during Phase II were slightly younger than those in Phase I, with the Phase II Confirmed Participants subgroup being slightly younger (mean 65.2 yrs ± SD 10.2). Phase II participants had a higher proportion of males than Phase I (26.9% vs 22.6%, respectively), with the highest subgroup being those in the Confirmed Participants subgroup (33.6% males). In all groups and subgroups, wrist fracture was the most prevalent type of fracture found at the time of screening.
Description of participants who were undiagnosed and untreated at baseline with followup data within 6 months of screening, by program phase. Values are n (%) unless otherwise specified.
Osteoporosis outcomes — BMD testing and risk assessment
Comparing Phase I to all Phase II participants, BMD testing rates differed by 5.3% (Fisher’s exact test, p < 0.0001) and were statistically significant, though only a modestly clinically important change from a program point of view (Table 1).
However, further comparisons contrasted the Phase I participants and the Phase II Confirmed Participants, and then Phase II Eligible Nonparticipants. More patients were tested for their bone density and had a fracture risk assessment done in the Phase II Confirmed Participant subgroup (95.1%) than in Phase I (65.4%). The latter was similar to the testing rate reported among Phase II Eligible Nonparticipants (54.9%; Table 1).
BMD test results were available for Phase II Confirmed Participants only and their fracture risk could be calculated using Canadian Osteoporosis Guidelines, and the Canadian Association of Radiologists and Osteoporosis Canada 2010 fracture risk assessment1. Within this group, 42.7% were at high risk for refracture, and 52.5% were at moderate risk for refracture (Table 1).
Treatment initiation
Treatment initiation rate was higher in the Phase II program as a whole, compared to Phase I (26.3% vs 20.5%, respectively) and although this was statistically significant, it was only modestly clinically important. When the Phase II group was subdivided into Confirmed Participants and Eligible Nonparticipants, a clearer signal was seen. The Confirmed Participants had a higher rate of treatment initiation (35.7%) than either Phase I or Phase II Eligible Nonparticipants (20.5% and 19.6%, respectively; Table 1). Within the Confirmed Participants group, 57.1% of those found to be at high refracture risk reported initiating treatment within 6 months and 22.9% of those at moderate risk, where treatment indication is less certain, initiated medication (Table 1).
Patient-reported barriers — reasons why patients did not see their PCP about bone health at followup
Of 3997 patients in Phase I, 708 (18%) reported that they did not return to their PCP for bone health assessment during the followup period. The PCP therefore could not order the BMD test. The 2 most common reasons were that the patient chose not to go to their physician for bone health followup (26.4%), and other health issues took precedence (21.2%; Table 2). Over 10% reported that they did not have time to see their PCP. Similarly, 158 (20%) of the 794 Phase II Eligible Nonparticipants reported not seeing their PCP for bone health assessment and for similar reasons, yet only 1% of Phase II Confirmed Participants reported the same (n = 7, 1%; Table 2).
Patient-reported barriers for not receiving fracture risk assessment or a prescription for pharmacotherapy within 6 months of screening by program phase (role of the coordinator shifts between Phase I and Phase II to include ordering BMD testing and communicating report of results to primary care). Values are n (%) unless otherwise specified.
Reasons why patients did not have a BMD test
As described in Table 2, 661 Phase I patients had returned to their PCP but did not have a BMD test. In Phase I, 39.2% reported that their physician said they did not need a BMD test, and nearly 10% indicated that their physician prescribed treatment without referring them for a BMD test (Table 2). Phase II Confirmed Participants did not report these barriers because they did not need to return to their PCP to access BMD testing, and 95% had the testing done. However, Phase II Eligible Nonparticipants had experiences similar to those of Phase I patients, with 35.1% reporting they were told they did not need the test and 10% having treatment without BMD testing.
Patient preferences were also noted. In Phase I, 8.5% stated other health issues took precedence and 6.2% did not want to have a BMD test. Very similar to the findings in Phase II, Eligible Nonparticipants (185) visited their PCP but were not tested, with 7.6% citing other health issues taking precedence and 3.8% not wanting the test. The same 2 reasons were the most prevalent among the small number (n = 19, 5%) of Phase II participants who did not have testing (Table 2).
Reasons why patients who were prescribed medication were not taking it at followup
Of the 134 (16.3%) Phase I patients who were not taking their prescribed medications at the time of followup, the most commonly cited reason was that they had not yet started the medications or filled their prescriptions (31.3%; Table 2). Concerns about side effects were also common (24.6%) and more prevalent than the 13.4% who reported experiencing side effects. Among Phase II patients participating in BMD testing within the program, 20 (9.8%) patients were not taking their prescribed medications at followup; of these, 7 patients had experienced side effects and 5 had not yet started the medications or filled their prescriptions. Finally, Phase II Nonparticipants had 13.5% not taking their medication at followup, with the most common reasons being having experienced side effects (n = 8).
DISCUSSION
As seen in the Phase II Confirmed Participants, eliminating the need for the patient to return to their PCP for referral for BMD testing, a necessary part of fracture risk assessment, eliminated the most prevalent barriers for returning to PCP and for BMD testing. This was also associated with higher treatment initiation rates (Phase II Confirmed Participants: 36% vs Phase I Patients and Phase II Eligible Nonparticipants: 20%).
Subgroup analyses of the Phase II participants demonstrated that this effect was removed when patients declined the new program when offered (Phase II Eligible Nonparticipants). The existence of this subgroup allowed us to see the importance of the uptake of the new program to achieve the elimination of these barriers. This corresponds with the results of a recent paper published by Beaton, et al23 evaluating the effect of BMD testing and risk assessment within the program on treatment outcomes, using a smaller sample of matched cases and controls. In our current study, however, we focused on the barriers to bone health testing and treatment, and we identified patients who were eligible but did not, for various reasons, participate in Phase II.
In Phase I of the program, the main patient-reported barriers for not visiting their PCP or not having a BMD test were patient- and physician-oriented (e.g., patient not wanting to follow up with PCP or being instructed by their physician to not have a BMD test). Phase II addressed the obstacles most amenable to change by providing physicians with a better foundation for informed decision making. Expedited BMD tests within the program allowed coordinators to send risk assessments and patient-specific, guideline-based recommendations directly to the PCP, with the goal of achieving higher rates of fracture risk assessment and pharmacotherapy for patients for whom it is indicated. As a result, those participating in Phase II (Confirmed Participants) did not report any physician-oriented barriers and the BMD testing rate was accordingly high (95%). On the other hand, those in the Eligible Nonparticipant subgroup in Phase II experienced many of the same barriers as those reported by Phase I patients, with similarly lower BMD testing rates at followup (54.9% vs 65.4%, respectively). The results for Phase I patients and Phase II Eligible Nonparticipants are consistent with studies that have used a more educational approach and returned the patient to the PCP for testing and treatment initiation, where programs depended on patients prioritizing underrecognized bone health issues at the time of their fracture6,7,24,25,26,27,28. Listening for patient-reported barriers helped to shed light on the gaps to full guideline implementation that could be modified in the program.
The proportion prescribed osteoporosis medication but not taking it at followup was lower in Phase II Confirmed Participants than Phase I patients and Phase II Eligible Nonparticipants. In Phase I, the main patient barriers included not having started medications/filled prescriptions and being concerned about side effects (but not having experienced them). These concerns were echoed by fragility fracture patients in other studies29,30, including our own group31. Our findings correspond with a previous study of postmenopausal women in the United States who self-reported being diagnosed with osteoporosis32. Lindsay, et al found that one of the main reasons for discontinuation of osteoporosis treatment was concerns about longterm safety and the experience of side effects, while the cost of medication, as in our study, was one of the least frequent reasons for discontinuation of osteoporosis medication32. Simonelli, et al29 surveyed PCP and orthopedic surgeons, finding that 61% reported concerns over potential side effects as a barrier to initiating osteoporosis treatment. In our study, we do not know the source of the patients’ concerns (media, or message from healthcare provider or family/friend). In general, the patient barriers identified in our study, particularly regarding knowledge and behaviors such as medication taking and following up with their PCP, are in line with the emerging barriers to the translation of research and evidence to practice13.
Among the strengths of our study was that the questions and multiple choice options asked of patients who did not initiate BMD testing or were not taking their prescribed medication were based on a previous qualitative study conducted to better understand testing/medication decision-making processes20,31. These were patient-centered in focus, thereby allowing for negative feedback about the program. Another strength was that our study was based on a large, multicenter cohort of individuals representing the fragility fracture population in Ontario. Finally, we observed a serendipitous comparative opportunity regarding eligible patients who did not participate in BMD testing and risk assessment within the program. Ongoing evaluations will be conducted as Phase II becomes the standard of care in the Ontario fracture screening program to reduce this potential care gap.
A limitation of our study is that there was a significant loss to followup in each phase of the program, which may affect the generalizability of our results. However, the loss to followup in Phases I and II were similar, and we have no reason to believe that any resulting attrition bias would be more favorable to one phase over another. Further, patients were not randomized to either phase, thus our results are based on 2 samples obtained at 2 different timepoints. Our direct comparison of the 2 phases regarding changes in patient-reported barriers may not be entirely attributable to the phases of the program themselves. There may be other differences between the phases that may explain our findings, including differences in patient characteristics and time-dependent factors. However, as described earlier, the patient samples in Phases I and II of the program were very similar.
Another limitation is that the main osteoporosis-related outcomes of interest were self-reported; however, Cadarette, et al33 found that there is minimal measurement error in self-reports of BMD testing. We also did not identify barriers from the perspective of physicians. Jaglal, et al34 found that PCP ordered BMD tests and tried to manage osteoporosis appropriately; however, they reported being confused about the available osteoporosis treatments and most were unaware of existing osteoporosis guidelines34. Further, Simonelli, et al29 found physician concerns over side effects an impediment to treatment and this may have been conveyed to their patients. In general, FLS-type programs still rely on the agency of the patient who is concurrently dealing with an acute fracture and the shared decision-making process with their PCP. Ultimately, it is the patient who needs to fill prescriptions and take the medication.
Our findings have important implications for FLS programs. The enhanced model (Phase II in our analysis) helped reduce what were previously dominant barriers to care (personal prioritization of bone health needs over fracture care, and PCP awareness of guidelines), and was associated with higher treatment rates. It also found that when the program was not in place, results reflected those of the simpler (Phase I) program with higher barriers and lower outcome rates. The upstream barriers were remedied by bringing risk assessment into our program and conveying the results and targeted guideline information out to PCP. PCP have multiple clinical practice guidelines to implement, and each physician will likely have relatively few postfracture patients to manage29,34. Enabling the coordinator to order BMD tests and facilitate communication of risk and targeted guidelines to PCP appears to have brought us closer to successful guideline implementation by supporting patients and their PCP in their treatment decision making. Our results also point to the importance of monitoring gaps in program implementation, and to the need for attention to the next set of barriers: perceived side effects of this class of drugs and medication-taking behaviors. Our findings demonstrate that listening to and acting on patient-reported barriers to care is important and can lead to positive change.
Acknowledgment
The authors gratefully acknowledge the support of Osteoporosis Canada, which implements the Ontario Osteoporosis Strategy Fracture Clinic Screening program on behalf of the Ontario Ministry of Health and Long-Term Care. The authors also thank members of the Fracture Clinic Screening Program Evaluation Team for their contributions to the program and its overall evaluation.
Footnotes
Supported by funding from the Ontario Ministry of Health and Long-Term Care (MOHLTC) through the fracture clinic screening program of the Ontario Osteoporosis Strategy. The views expressed are those of the authors and do not necessarily reflect those of the MOHLTC.
- Accepted for publication April 13, 2018.








{kind=link}