

Abstract
Objective. To prospectively evaluate automated multiplex PCR and isothermal microcalorimetry tests for rapid and accurate diagnosis of septic arthritis.
Methods. Patients with acute arthritis were prospectively included from October 2014 to September 2015. In synovial fluid (SF), leukocyte count and differential, culture, PCR, and microcalorimetry were determined. Septic arthritis was diagnosed by positive SF culture or (1) local clinical signs and symptoms, (2) increased SF leukocyte count, and (3) exclusion of noninfectious causes of inflammatory arthropathy. The performance of individual tests was compared with McNemar’s test.
Results. Among 57 patients, 22 (39%) were diagnosed with septic arthritis. SF culture grew a pathogen in 10 patients (46%), PCR was positive in 5 (23%), and microcalorimetry in 10 (46%). Compared to SF culture, 49 concordant pairs were found for both methods (PCR and microcalorimetry; 86% agreement). In SF, PCR failed to detect Staphylococcus aureus (2 patients), Streptococcus pneumoniae (1 patient), Streptococcus dysgalactiae (1 patient), and Clostridium clostridioforme (1 patient). Microcalorimetry failed to detect S. dysgalactiae (1 patient), Streptococcus agalactiae (1 patient), and C. clostridioforme (1 patient). No statistical differences between the performance of SF culture, and PCR and microcalorimetry, respectively, were found. The processing time for PCR was 5 h and for microcalorimetry a median of 8.8 h (range, 2.3–64 h), whereas cultures required a median of 4.5 days (range, 3–14 days).
Conclusion. Performance of SF PCR was inferior while microcalorimetry was similar to culture but provided results considerably faster. [Clinical trial registration number (https://www.clinicaltrials.gov): NCT02530229]
Septic arthritis is a medical emergency with high morbidity and an annual incidence of 4–10 infections per 100,000 inhabitants1,2. It requires prompt arthroscopic or open surgical intervention to avoid irreversible bone and cartilage destruction with consecutive development of secondary osteoarthritis (OA) and extension into the adjacent tissue. Therefore, early diagnosis of septic arthritis and its discrimination from noninfectious inflammatory conditions, such as crystal-induced arthropathy or exacerbation of rheumatoid arthritis (RA), is important to avoid surgical and antimicrobial undertreatment and overtreatment1,2,3,4,5. Joint aspiration is the standard preoperative diagnostic procedure performed in clinical routine. However, culture of synovial fluid (SF) requires time and has limited sensitivity, especially when previous antibiotic therapy was administered.
Molecular methods, such as PCR, were intensively investigated for rapid and accurate diagnosis of bacterial infections, particularly in patients who previously received antibiotic treatment. Broad-range, 16S ribosomal DNA PCR have shortcomings, including limited sensitivity, risk of contamination, and difficulties in identification of mixed bacterial infections6,7, whereas multiplex PCR is limited to predetermined microorganisms for which primers are included in the test kit8,9. Multiplex PCR has shown promising results for the diagnosis of periprosthetic joint infection in sonication and SF8,9,10,11. However, it has not yet been evaluated for the diagnosis of septic arthritis in SF of native joints.
Microcalorimetry measures growth-related heat production of reproducing cells in biological fluid and delivers real-time evaluation of microbial growth. It has obtained promising results in the diagnosis of septic arthritis12 and periprosthetic joint infection with sonication fluid13, with a mean detection time of about 6 h. Hence, microcalorimetry could be a promising screening test for rapid diagnosis of septic arthritis.
In this prospective study, we aimed at evaluating the performance of a fully automated multiplex-PCR cartridge system and isothermal microcalorimetry for rapid detection of microorganisms in SF and compared them to conventional diagnostic methods, including SF leukocyte count, culture, and cytopathologic examination.
MATERIALS AND METHODS
Study design
This prospective study (public clinical trial identification NCT02530229) was conducted in accordance with the Declaration of Helsinki and was approved by our institutional ethics committee (EA1/306/14); patients gave written informed consent.
Study population
Patients aged 18 years and older presenting in the surgical emergency room of a tertiary healthcare center between October 2014 and September 2015 with acute inflammatory signs of the native hip or knee joint were included. SF obtained by joint aspiration was analyzed. Patients with an aspirated SF volume of < 5 ml were excluded from the study. If the likelihood of septic arthritis was estimated as high based on clinical and laboratory variables at admission, a surgical intervention was performed.
Definitions
Septic arthritis was diagnosed if a pathogen grew in the SF or synovial tissue (if collected during surgery) or the following 3 criteria were present1,12,14: (1) local signs and symptoms of inflammation (pain, redness, warmth, effusion, new impairment of joint function), (2) increased SF leukocyte count (> 50,000/µl) or granulocyte percentage (> 90%), and (3) absence of other (noninfectious) causes of acute arthritis, such as crystal-induced arthropathy, reactive arthritis, activated OA, and RA. Culture of SF was considered positive if the causing pathogen was cultured on solid media. Growth in broth only was considered positive in case of isolated highly virulent organisms. If the SF culture grew a pathogen and concomitant crystals were found, a co-existent condition of septic arthritis and crystal-induced arthropathy was diagnosed. If subsequent surgery was performed, the results of intraoperative tissue cultures were included. Tissue culture was considered positive if at least 1 specimen grew a high-virulence pathogen (e.g., Staphylococcus aureus, Enterobacteriaceae, Streptococcus, Enterococcus, Candida spp.) or at least 2 specimens grew a low-virulence pathogen [e.g., coagulase-negative staphylococci, Cutibacterium (formerly Propionibacterium) spp., other bacteria of the normal skin microbiota]15.
Conduction of joint aspiration
An orthopedic or traumatology surgeon performed joint aspiration following standardized aseptic technique. In a first step, skin was prepared. Then, a sterile 18-gauge spinal needle and a 10-ml syringe were used to aseptically collect SF. The needle was repositioned without withdrawing it through the skin if no SF was obtained. No fluid was injected into the joint cavity. The presence or absence of purulence and the collected volume of SF was registered.
Preoperative diagnostic tests
A vial containing EDTA was filled with a minimum of 1 ml of SF for automatic processing of leukocyte count and granulocyte percentage. The EDTA vial was gently turned by hand-mixing 5 times. In cases of clotting, 10 µl hyaluronidase (Sigma-Aldrich Chemie) was added and incubated for 10 min at room temperature. A pediatric blood culture bottle (BacTec PedsPlus/F, Becton Dickinson and Co.) was filled with a minimum of 1 ml of SF. A native vial was inoculated with more than 1 ml for gram stain and culture. SF was inoculated on Schaedler, blood, and chocolate agar plates (Becton Dickinson); the remaining fluid was inoculated in thioglycolate broth for enrichment. For 7 days the aerobic cultures were incubated at 37°C and monitored daily, while the anaerobic cultures were incubated for 14 days. The pediatric blood culture bottle was incubated at 36 ± 1°C for 14 days or until a positive growth was signaled. A native vial with 1 ml was used for multiplex PCR and microcalorimetry. Another 1-ml aliquot was used for polarization microscopy for detection of inflammatory cells and urate, pyrophosphate, and hydroxyapatite crystals.
Intraoperative diagnostic tests
If subsequent surgery (arthroscopy or arthrotomy) was performed, at least 5 tissue samples were collected, homogenized, and inoculated on agar plates, as described above; the remaining homogenate was inoculated in thioglycolate broth.
Multiplex PCR analysis
For detection of specific pathogens (Supplementary Table, available from the authors on request), a multiplex PCR device (Unyvero, Curetis) was used as previously described10,11. This multiplex PCR device allows a semiquantitative DNA determination by 8 multiplex PCR reactions in parallel. The Implant and Tissue Infection cartridge was used following these steps: the Unyvero sample tube, prefilled with specific lysis reagent, was inoculated with an aliquot of 180 µl of SF and introduced in the lysator for 30 min. Then, the sample tube and the master mix were inserted together into the cartridge that was prefilled with integrated reagent containers and buffers for DNA purification, a DNA purification column, and 8 independent PCR chambers with individual arrays for array purification. A series of hybridization procedure images were recorded by a fluorescence camera. Each analyte had a specific threshold of positivity of 104 DNA fragments/ml. For this study, the third generation of cartridges, which also included 16S DNA primers, was used. A complete PCR test cycle required 5 h of standard processing time until yielding a result.
Microcalorimetry measurements
A vial with a minimum of 1 ml of SF was immediately transported to our laboratory for microcalorimetry and PCR analysis. In the laboratory, a 4-ml microcalorimetry vial, prefilled with 2 ml of tryptic soy broth, was filled with 1 ml of SF. Then the vial was introduced into an isothermal microcalorimeter with 48 independent measuring channels (model 3102 TAM III, TA Instruments) and a sensitivity of 0.225 µW. First, a working temperature of 37°C was reached within an equilibration phase of 15 min, followed by a 45-min stabilization phase. Then, the continuous measurement of heat production (expressed in µ-Watt) was performed for at least 5 days. Finally, after finalization of the microcalorimetry measurement process, aerobic and anaerobic quantitative cultures were performed by plating the remaining microcalorimetry fluid on agar plates.
Statistical analysis
To evaluate the performance of each diagnostic method, the sensitivity, specificity, positive predictive value, negative predictive value, and accuracy of each test were calculated by comparing them to the gold standard measurement methods (cultures, leukocyte count/differential, etc.), respectively. Student t test and Mann-Whitney U test were used to compare demographic groups. McNemar’s chi-square test (2-sided) was used to compare the results between diagnostic tests. The level for statistical significance was defined at p value < 0.05.
RESULTS
Demographic data and infection characteristics
Table 1 summarizes the characteristics of 57 patients with acute arthritis, involving 50 knee and 7 hip joints. A total of 22 patients were diagnosed with septic arthritis. In the group of 35 patients with noninfectious arthritis, the cause of joint complaints was identified for 27 patients (77%), including posttraumatic or postoperative joint effusion in 9 patients, meniscus lesion in 5 patients, activated OA in 3 patients, reactive arthritis in 3 patients, noninfectious necrosis in 2 patients, RA in 2 patients, crystal-induced arthropathy in 2 patients, and loose body in the joint in 1 patient. In 8 patients (including 7 with septic arthritis and 1 with noninfectious arthritis), empiric antimicrobial treatment was administered before joint aspiration.
Demographic data and infection characteristics.
Microbiological findings
The microbiology and route of infection are summarized in Table 2. The causative pathogen of septic arthritis was identified by culture of SF and/or intraoperative tissue in 14 cases (64%). The most common isolated pathogens were Streptococcus spp. (5 patients) and S. aureus (5 patients).
Microbiology and route of infection in 22 patients with septic arthritis.
Performance of diagnostic tests
Table 3 depicts the performance of diagnostic tests. The SF leukocyte count and granulocyte percentage showed the highest sensitivity (94%). Among 22 patients with septic arthritis, SF culture was positive in 10 (46%) compared to PCR, which was positive in 5 patients (23%, p = 0.134), and microcalorimetry in 10 patients (46%, p = 0.683). When considering only pathogens for which primers were included in the PCR test kit, the detection rate increased to 25% (5 of 20 detectable microorganisms). The accuracy of SF culture, PCR, and microcalorimetry were similar. The sensitivity of intraoperative tissue histology and culture of patients undergoing surgery was 77% (i.e., 10 of 13 patients) and 56% (i.e., 10 of 18 patients), respectively.
Performance of preoperative diagnostic tests for the diagnosis of septic arthritis.
In 1 case, joint aspirate culture showed growth of S. aureus as well as crystals and was classified as septic arthritis with coexistent crystal-induced arthropathy.
Discordant test results
Figure 1 shows the comparison of PCR and microcalorimetry with conventional culture of SF. For both tests, 49 concordant pairs were found (i.e., the agreement rate was 86%). Table 4 summarizes discordant cases and negative SF analyses. In 5 cases of septic arthritis, PCR failed to detect the pathogen where culture grew the underlying microorganism. In 2 of 5 cases, there was no primer for detection of the causing pathogen included in the cartridge of the PCR test (Streptococcus pneumoniae and Clostridium clostridioforme). In 3 cases, all analyses of SF missed the pathogen that was detected in the intraoperatively harvested tissue cultures. In 3 cases with noninfectious arthritis, only PCR analysis from SF was positive, whereas all the other methods were negative. In 2 cases, Cutibacterium acnes was identified by PCR, a low-virulent microorganism, which is typically classified as contaminant in the absence of foreign material and preceding intervention (aspiration, arthroscopy, or injection). Klebsiella pneumonia was detected in a noninfectious case by PCR. Analogically, in 2 patients with noninfectious arthritis (i.e., crystal-induced and reactive arthropathy), only microcalorimetry was positive. In these 5 cases, the PCR and microcalorimetry tests were both considered false-positive.

Results of synovial fluid culture, PCR, and microcalorimetry in 22 patients with septic arthritis.
Patients with concordant false-negative and discordant results.
Turnaround time and feasibility of diagnostic tests
The turnaround time of PCR was 5 h, whereas microcalorimetry required a median of 8.8 h (range, 2.3–64 h; Figure 2), and cultures a median of 4.5 days (range, 3–14 days). The PCR was fully automated and its handling did not require an experienced laboratory technician. Microcalorimetry required a laboratory technician to calibrate the machine and prepare the probes with the required broth. Microbial growth was recorded live and annotated by the technician.
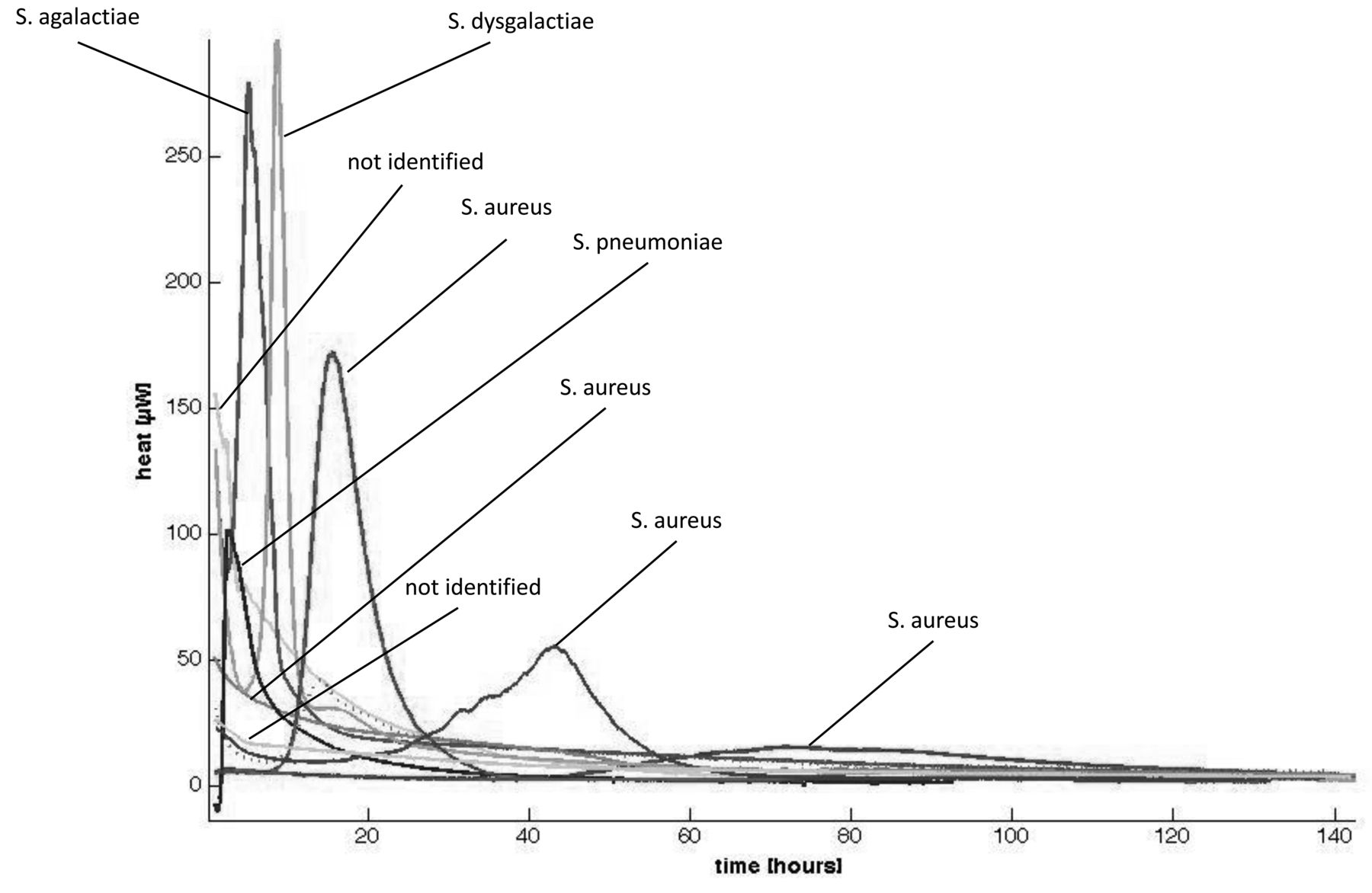
Microcalorimetry (heat flow) curves. Streptococcus spp.: S. pneumoniae, S. agalactiae, S. dysgalactiae. Staphylococcus spp.: S. aureus.
DISCUSSION
Nonmicrobiological methods, such as determination of SF leukocyte count, obtained the highest sensitivity for detection of septic arthritis. However, these tests can also be positive in noninfectious inflammatory joint diseases (e.g., in crystal-induced arthropathy or exacerbated rheumatic diseases) and do not provide information on the causative pathogen. The sensitivity of polarized light microscopy for detection of crystals in SF is limited and depends to a large extent on the experience of the investigator16,17. Therefore, microbiological tests for accurate detection of pathogens are still required in the diagnosis of septic arthritis.
To our knowledge, this is the first report on the performance of multiplex PCR for diagnosing septic arthritis from SF. The fully automated multiplex PCR test evaluated in our study showed no significant differences in performance compared to culture in SF. However, the sensitivity of multiplex PCR is low and is restricted by the limited number of bacteria that can be identified, because only selected primers for detection of specific pathogens involved in the investigated disease are included. This explains why 2 pathogens that were not included in the test kit (S. pneumoniae and C. clostridioforme) were missed. The performance of the evaluated PCR test kit could probably be improved by including additional PCR primers for pathogens commonly involved in septic arthritis such as additional streptococcal species. Additionally, preanalytical processes that concentrate DNA may improve the detection of low-grade infections caused by skin bacteria.
Sensitivity of microcalorimetry was on par to cultures and superior to PCR. Microcalorimetry yielded results in a median of 8.8 h, which was considerably faster than cultures. However, microcalorimetry does not yet identify the microbiological agent and consecutive sequencing is necessary to determine antibiotic resistance. In future work, characteristic microcalorimetric curves of pathogenic agents should be identified for a rapid identification of the causing agent.
The sensitivity of SF culture in our cohort with septic arthritis was low compared with other studies that reported detection rates of up to 82%18. This discrepancy may be explained in part by about a quarter of our patients having been given antibiotics before puncture. However, it must be noted that the PCR test also did not detect additional pathogens.
We acknowledge several limitations of our study. First, no attempts were made to identify pathogens in false-negative SF samples by culture and/or PCR. It remains unclear why a large proportion of SF samples from patients with septic arthritis remained negative. One approach to clarify this question would be to eliminate potential PCR inhibitors in SF, such as blood contamination of the SF sample, or use alternative methods, such as whole-genome sequencing19. In addition, pathogens that are difficult to cultivate or difficult to detect were not specifically searched for, such as mycobacteria, Sporothrix schenckii, Borrelia burgdorferi, or Tropheryma whipplei, which could have been missed. However, these pathogens rarely present as acute episodes and are less likely to be the causative pathogen in our study population. Second, no determination of bacterial counts and DNA quantity was performed in SF. Therefore, no estimation of viable or nonviable bacteria can be provided, especially in comparison between previously treated and untreated patients. Third, the definition criteria for septic arthritis in this cohort, although widely used, introduced circularity and may favor the detection results of leukocyte count/differential and culture. Additionally, these criteria may not always accurately distinguish infections from noninfectious arthropathy. Hence, septic arthritis may have been overdiagnosed, particularly as diagnostic tests for crystal-induced and rheumatic arthritis may also lack sensitivity.
The performance of SF PCR was inferior to culture (even though not statistically significant), while microcalorimetry’s performance was on par to culture, but with the advantage of providing results within 5 h and 8.8 h, respectively. This benefit is relevant in clinical practice, because rapid diagnosis of septic arthritis and early initiation of adequate surgical and antimicrobial treatment represents the mainstay of successful management for septic arthritis3. However, because of its low sensitivity and the need for susceptibility testing, multiplex PCR and microcalorimetry cannot currently replace culture. With improvement of the detection rate, PCR and microcalorimetry may complement or replace culture, providing rapid microbiological results.
Acknowledgment
We thank Maren Engel, Antje Spranger, and orthopedic surgeons from our institution for recruiting study patients.
Footnotes
Supported by a research grant from the PRO-IMPLANT Foundation (www.pro-implant-foundation.org). Curetis GmbH provided diagnostic PCR test kits and reagents for this study. None of the funders had a role in study design, data collection, and interpretation, or the decision to submit the work for publication. AT and NR report a grant from Curetis GmbH and the PRO-IMPLANT Foundation during the conduct of the study.
- Accepted for publication May 31, 2018.








{kind=link}
{kind=link}