

Abstract
Objective. To assess associations between cardiorespiratory fitness (CRF), measured as peak oxygen uptake (VO2peak), and cardiovascular disease (CVD) risk, measured by arterial stiffness, in patients with ankylosing spondylitis (AS).
Methods. VO2peak was assessed by a maximal walking test on a treadmill. Arterial stiffness was measured noninvasively (Sphygmocor apparatus). Cross-sectional associations between VO2peak and arterial stiffness were analyzed using backward multivariable linear regression.
Results. Among 118 participating patients, there were significant inverse associations between VO2peak and arterial stiffness, independent of traditional CVD risk factors and measures of disease activity.
Conclusion. Reduced CRF may be related to increased risk of CVD in AS.
Physical activity is a cornerstone of the treatment of ankylosing spondylitis (AS), and traditionally the focus has been on flexibility exercises. The majority of the patients with AS reports performing low-intensity exercises1,2, which do not improve cardiorespiratory fitness (CRF), and a study found that patients with AS have lower CRF than controls3.
CRF is the circulatory and respiratory systems’ ability to supply oxygen to the skeletal muscles during sustained physical activity, and the most important lifestyle factor to improve CRF is physical activity at moderate to high intensity4. CRF can be measured as maximum oxygen uptake (VO2peak) with gas analyses during maximum exercise or estimated by indirect exercise tests calculating VO2peak3,4,5. Low CRF is an independent predictor of cardiovascular disease (CVD) in the general population and in patient groups with increased risk of CVD such as those with diabetes6, and improvement of CRF is associated with lower risk of CVD4. Possibly, also in patients with AS, low CRF is a risk factor for CVD; however, this has not been analyzed previously.
Patients with AS have an increased risk of CVD7, and arterial stiffness, a validated marker of CVD risk8, has been shown to be elevated in these patients9,10. In the general population, there is an inverse association between CRF and arterial stiffness11,12. The hypothesis of our study was that there is an inverse relationship between CRF and arterial stiffness independent of traditional CVD risk factors and disease activity in patients with AS.
MATERIALS AND METHODS
This was a cross-sectional study in a cohort of patients with AS described previously10. The study was approved by the local Committee of Ethics (approval number S-02059) and performed according to the Helsinki declaration. All patients gave their written consent.
Information on demographics, height at adulthood, medical history, and medications was self-reported in questionnaires, and later confirmed in an interview with a cardiologist. Body mass index (BMI) was calculated from measured height and weight. Loss of height was calculated as height at adulthood minus height at data collection. C-reactive protein (CRP), total cholesterol (TC), and high-density lipoprotein cholesterol (HDL-C) were analyzed consecutively. Disease activity was assessed by the AS Disease Activity Score (ASDAS)-CRP and by the Bath AS Disease Activity Index13,14.
CRF was estimated indirectly as VO2peak by a maximal walking test on a treadmill (modified Balke protocol), as described previously (Supplementary File 1, available with the online version of this article)3. The test was ended when the participants were unable to increase inclination or speed of the treadmill and reported a perceived exertion on Borgs scale 17–203.
Brachial blood pressure and arterial stiffness were measured after at least 5 min of supine rest. Arterial stiffness was measured noninvasively (Sphygmocor apparatus) both as augmentation index (AIx) and pulse wave velocity (PWV), described in detail previously (Supplementary File 1, available with the online version of this article)10.
The statistical analyses were performed using SPSS version 21. Unadjusted associations between VO2peak and arterial stiffness were investigated in scatterplots with calculation of regression lines.
AIx and PWV were dependent variables in separate age- and sex-adjusted univariate linear regression analyses. We included the following independent variables: VO2peak, traditional CVD risk factors (smoking, BMI, TC, HDL-C, and central mean arterial pressure), measures of inflammation and disease activity (CRP and ASDAS), use of nonsteroidal antiinflammatory drugs, and other factors known to influence the arterial stiffness measurements (height in AIx analyses and loss of height in PWV analyses). PWV was log-transformed to obtain normality of the residuals.
We then performed backward multivariable regression with variables with a p value < 0.25. Nonsignificant variables (p ≥ 0.05) were removed until only significant variables (p < 0.05) remained. Nonsignificant variables from the adjusted univariate analyses were re-entered into the final model to check for confounding. We assessed possible interactions between CRP and VO2peak as well as ASDAS and VO2peak. The residuals of the final models were assessed for normality. We also performed similar analyses excluding patients with established CVD.
RESULTS
Out of 159 patients with AS in the cohort, 118 had available data on both CRF and arterial stiffness. Missing data were mostly due to logistical reasons (Supplementary Figure 1, available with the online version of this article). Descriptive data are given in Table 1.
Characteristics of the patients.
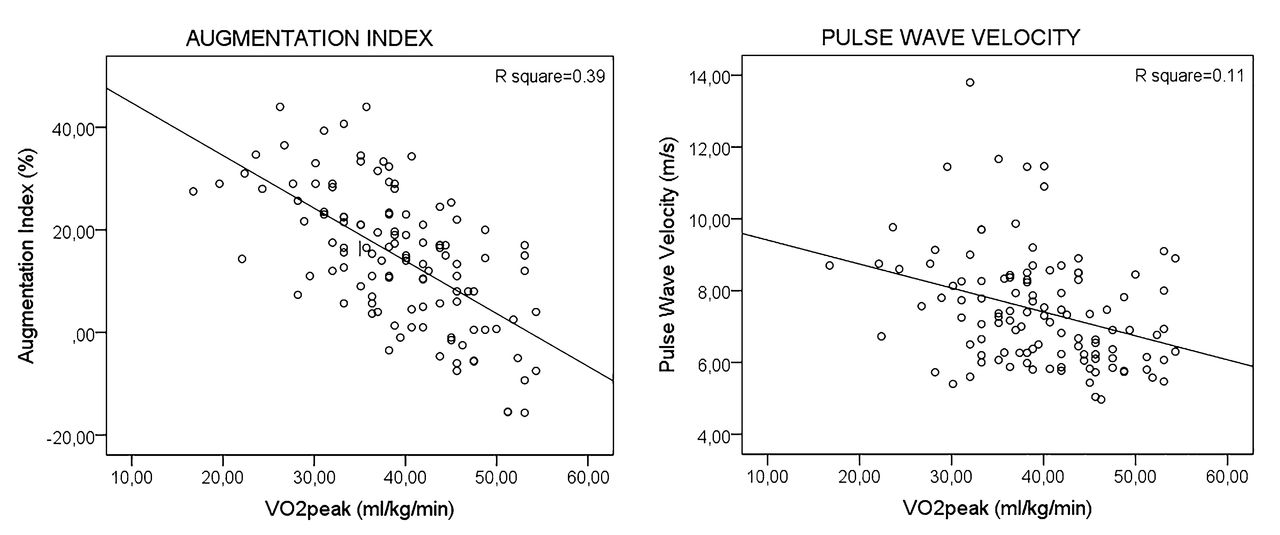
Scatterplots (Figure 1) indicated inverse relations between VO2peak and both AIx (p < 0.001) and PWV (p < 0.001). In the multivariable linear regression models, VO2peak was independently and inversely associated with AIx (β −0.3, 95% CI −0.6 to −0.1, p = 0.01) and log-transformed PWV (lnPWV; −0.005, CI −0.010 to −0.001, p = 0.03; Table 2). There were no interactions between CRP and VO2peak or ASDAS and VO2peak. Analyses with exclusion of patients with established CVD (9 patients) did not alter results (data not shown).
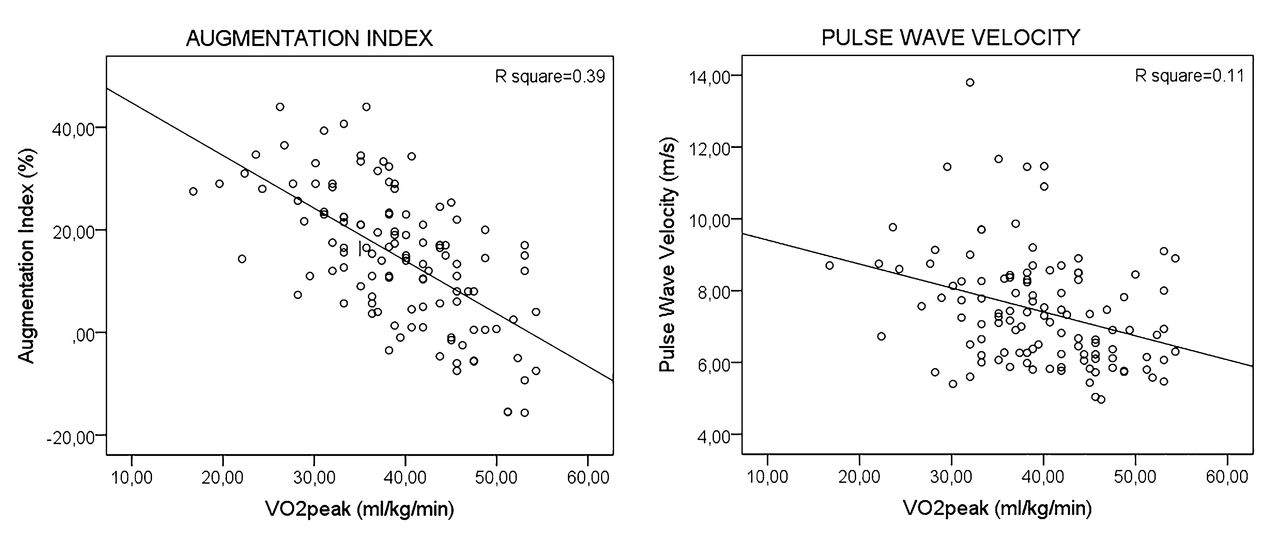
Scatterplots for cardiorespiratory fitness and arterial stiffness. Associations between VO2peak and arterial stiffness measured as augmentation index and pulse wave velocity with a regression line. VO2peak: peak oxygen uptake.
Associations between cardiorespiratory fitness and arterial stiffness, in multivariable linear regression.
DISCUSSION
Our data demonstrate cross-sectional independent inverse associations between VO2peak (a measure of CRF) and arterial stiffness (a measure of CVD risk), assessed both as AIx and PWV in patients with AS.
Although similar inverse relations between CRF and arterial stiffness have been found in the general population11,12, we have not identified other studies analyzing associations between CRF and arterial stiffness in patients with AS or other inflammatory joint diseases (IJD). In patients with rheumatoid arthritis (RA), 1 study found inverse associations between increasing levels of self-reported physical activity and AIx, in line with our results15. Another study on RA found that higher CRF was associated with a better CVD risk profile; however, arterial stiffness was not an outcome16. We have previously published results from a randomized controlled trial evaluating the effects of high-intensity exercise in patients with AS showing significant treatment effects on both VO2peak (increased) and arterial stiffness (decreased), although, owing to the low sample size, associations between the changes of these variables were not evaluated17.
CRF is determined by genes, age, sex, physical activity, smoking, obesity, and medical conditions, where physical activity is the most important lifestyle factor4. In the general population there is a dose-response relation between physical activity and CRF in which physical activity/exercise at moderate and high intensity results in improvement of CRF. Thus, CRF is a marker of habitual physical activity4.
Arterial stiffness is determined by the functional and structural properties of the arterial wall. Traditional CVD risk factors (hypertension, hypercholesterolemia, BMI, and smoking) and IJD are associated with increased arterial stiffness18. Moreover, regular aerobic high-intensity exercise can reduce arterial stiffness in healthy adults and patients with increased risk of CVD19. Regular aerobic exercise can affect both functional and structural components of the arterial wall, and about 40% of the CVD risk reduction of aerobic exercise is believed to be attributed to improved vascular hemodynamic properties, including arterial stiffness8,19.
Accordingly, regular exercises may be an important factor behind the associations between CRF and arterial stiffness measurements in our present study. In studies of the general population, improvement of CRF (where the participants increased the amount of exercise) has been associated with lower risk of CVD4. Therefore, high-intensity exercises aiming at improving CRF may be an attractive way to reduce arterial stiffness and CVD risk in patients with AS.
Our group has previously published results from the same AS cohort in which disease-related complaints were barriers for physical activity20, and disease activity (ASDAS) was inversely associated with CRF3. Accordingly, high disease activity may result in less physical activity and reduced CRF, which in turn is associated with increased risk of CVD. Reducing disease activity by optimal medical treatment may facilitate increased exercise at intensities needed to improve CRF and thereby reduce CVD risk.
There are some limitations of our study. This is a cross-sectional study, and the results are associations and cannot indicate causality. There may be bidirectional effects; high CRF may reduce the arterial stiffness by mechanisms mentioned previously, but increased arterial stiffness may also reduce CRF through increased systolic heart load, limiting cardiac output and thus reducing VO2peak11. However, repeating the analyses after exclusion of patients with CVD did not alter the results, indicating that established CVD is not the only factor explaining the association between CRF and arterial stiffness. Ideally, VO2peak should have been measured by direct gas analyses during a maximal exercise test. However, estimation of VO2peak by an indirect maximal exercise test is regarded as the second-best test and is considered as an acceptable test of CRF in research. The validity has been tested by comparing the estimated with direct measurement of VO2peak5. Estimation of VO2peak may be difficult in patients with physical disabilities (e.g., arthritis in joints of the lower limbs), and may result in underestimation of VO2peak. However, 98% of the patients reported reaching ≥ 17 on Borgs scale, indicating that the majority of patients exercised until exhaustion. Further, the mean heart rate at the end of the exercise test (172 bpm) was close to the expected maximum heart rate (220 bpm minus age), which in this cohort is 171 bpm, suggesting that VO2peak was not underestimated. Another important aspect is that in our present study we have analyzed associations between biomarkers; VO2peak (marker of CRF) and arterial stiffness (marker of CVD risk). Biomarkers mirror only some aspects of the truth, and conclusions must be drawn with caution. Clinical cardiovascular endpoints would have been more optimal endpoints, but would not be achievable in this cohort with a mean age of 49 years and with a sample size of 118 patients.
We found that low VO2peak was associated with higher arterial stiffness in patients with AS, indicating that low CRF is associated with increased CVD risk. The clinical implication of this association may be that CVD risk can be reduced by increasing CRF in patients with AS, but longitudinal intervention studies are warranted that analyze the effect of exercises improving CRF upon CVD risk in AS.
ONLINE SUPPLEMENT
Supplementary material accompanies the online version of this article.
Footnotes
Supported by The Norwegian Rheumatism Association.
- Accepted for publication April 6, 2018.








{kind=link}