

Abstract
Objective. Magnetic resonance imaging (MRI) has been increasingly recognized as a critical tool for the assessment of patients with rheumatoid arthritis (RA) and is able to reliably identify synovitis, bone marrow edema, bone erosion, and joint space narrowing (JSN)/cartilage loss. Understanding the exact relationship between each MRI feature and local synovial pathobiology is critical to dissect disease pathogenesis as well as develop future predictive models.
Methods. A systematic review was performed of the current published literature examining the relationship between MRI abnormalities and synovial pathobiology in patients with RA.
Results. Eighteen studies were identified; most focused on validation of MRI as a tool to detect and quantify synovitis, with a significant relationship demonstrated. Additionally, from the limited data available, a critical role seems likely for synovial pathways, at least in driving joint damage. However, there was a lack of data examining the relationship between synovial pathobiology and bone marrow abnormalities and JSN.
Conclusion. Although understanding the interrelationship of these disease biomarkers offers the potential to enhance the predictive validity of modern imaging with concomitant synovial pathobiological analysis, further studies integrating MRI with synovial tissue analysis in well-controlled cohorts at distinct disease stages before and after therapeutic intervention are required to achieve this.
Magnetic resonance imaging (MRI) is an excellent tool to delineate pathology in rheumatoid arthritis (RA) because it can define bone, cartilage, fluid, and soft tissues. This is possible because MRI can delineate structures with high water content on T2-weighted fat-suppressed or short-tau inversion recovery sequences, and following injection of gadolinium-DTPA (Gd-DTPA), regions of high vascularity. Thus, feasibly MRI can quantify both synovial volume and inflammation and act as a surrogate noninvasive marker of histological inflammation. Specific MRI features of RA synovial joints have been demonstrated to be of particular prognostic value: synovitis, bone marrow edema (BME), bone erosions, and cartilage thinning. MRI has the capacity to detect bone erosions 2 years earlier1 than plain radiographs and sensitivity to detect change even in small cohorts2, an effect that is of critical relevance given the capacity of improved treatment algorithms to halt joint damage3. Consequently, MRI is now well recognized as a robust outcome measure in clinical trials.
Historically, the pathological events leading to joint damage in RA have been suggested to be a sequence of primary synovitis leading to BME, cartilage thinning, and finally erosions. There is increasing data to challenge this model. First, although a significant relationship between BME and synovitis4 and between synovitis and the development of bone erosions has been demonstrated5, debate regarding the exact contribution of synovitis/BME in initiating and/or sustaining bone erosion continues6 with some evidence suggesting that BME per se may be an independent predictor of erosive progression4,7,8,9,10,11,12,13. Further, there is evidence primarily from MRI studies to support a bio-mechanical effect on erosive progression14. Second, MRI studies have noted BME and erosions as early events, with cartilage thinning occurring later15. Third, a number of radiographic studies have reported an incongruent relationship between cartilage thinning and erosions15,16. Finally, recent data have demonstrated an association between MRI-documented BME, synovitis, baseline cartilage damage, and subsequent cartilage loss17. These observations raise a number of fundamental questions regarding mechanisms of joint damage and in particular whether synovial pathobiological pathways initiate and/or sustain a local environment that drives BME, erosions, and/or cartilage thinning.
It was within this context that a systematic literature review was conducted to assess published data investigating the relationship between RA synovial pathobiology and MRI BME, synovitis, erosions, and cartilage thinning.
MATERIALS AND METHODS
The study methodology was conducted in line with the PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analyses) guidelines18 and was registered with PROSPERO (www.crd.york.ac.uk/NIHR_PROSPERO, registration CRD42016033875). Because this was a systematic review, no ethics approval was sought, in accordance with the policy of Barts Health NHS Trust.
Search strategy
Relevant articles, reviews, and abstracts were identified through an initial search of EMBASE, MEDLINE, and the Cochrane Library for articles published up to March 2016. The MEDLINE MeSH keyword search terms (rheumatoid arthritis, rheumatoid and arthritis, RA, rheumatoid, inflammatory arthritis, nuclear magnetic resonance imaging, magnetic AND resonance AND imaging, synovitis, synovi, pathology, histopathology, immunohistochemistry, pathol, histo, immune, joint surgery, arthroscopy, biopsy, joints, surgery) and adopted Boolean operators are presented in Table 1. These were modified to accommodate each search database. EMBASE and Cochrane search terms are presented as Supplementary Tables 1 and 2, respectively, available from the authors on request.
The MEDLINE MeSH keyword search terms and Boolean operators from 1946 to present.
Eligibility criteria
Studies including patients with RA undergoing an MRI scan of a peripheral synovial joint along with sampling of synovial tissue were eligible. Outcome measures for MRI scanning included BME, joint erosion, synovitis, and cartilage thickness. Outcome measures for synovial tissue included macro/microscopic histological assessment and immunohistochemical and gene expression analysis. To be included within the review, studies had to directly compare 1 MRI RA feature with 1 or more synovial outcome measures. All types of study designs were included and analysis was restricted to humans. Articles not in English, with no translation available, and abstracts with no corresponding full-text article were excluded.
Two reviewers (FH and AM) independently reviewed the titles and abstracts from potentially relevant articles identified through the search strategy. Both reviewers assessed the full texts of all potentially eligible articles.
Data extraction
Data were entered onto a predefined data extraction table. For each study, the following data were recorded regarding study design: type of study, disease stage (e.g., early vs established disease), procedure for synovial sampling, time interval between synovial sampling and MRI scan, whether concomitant disease-modifying antirheumatic drugs (DMARD) and/or steroid therapy were controlled for, joint imaged, and joint biopsied. The following MRI variables were also recorded: MRI feature scored, acquisition strength, and method of assessment of MRI features. Additionally, the following variables regarding synovial tissue analysis were recorded: number of synovial samples taken, procedure for synovial tissue preparation, macroscopic assessment of synovium, histological assessment of H&E stained samples, immunohistochemical assessment, synovial gene expression analysis, and main conclusions. Data extraction was performed by 1 reviewer (FH) and was verified by a second (AM). Any disagreements regarding data extraction were resolved following discussion among the reviewers.
Quality assessment
The quality of each study was independently assessed by 2 reviewers (FH and AM) using an adapted standardized quality scoring tool (Supplementary Table 3, available from the authors on request)19,20 to assess the following components: (1) study population, (2) MRI assessment and scoring, (3) histological assessment, and (4) study design and analysis and data presentation. A score of “1” or “0” was allocated for each question according to whether the study fulfilled the criteria or not, respectively. A study was considered to be high quality if it exceeded or equaled the mean score (% of total) in its class [cross-sectional vs randomized controlled trial (RCT) vs cohort study].
RESULTS
Search strategy
A summary of the results of the search strategy is presented in the PRISMA flow chart shown in Figure 1. This indicates that a total of 505 articles were identified. Following the exclusion of duplicates (n = 117) and review articles (n = 103), 273 articles were screened. Of these, 237 were excluded (134 because they did not include patients with RA, 91 because they did not include histopathological analysis of synovial tissue, 10 because they were examinations of tissue in vitro or in animal models, and 2 because no MRI scans were included). Of the remaining 36 articles, 18 were then excluded: 2 because no English translation was available, 5 because of no synovial histopathobiological examination (3 had no synovial histology and 2 had synovial explants in vitro only), 1 because there was no comparison of MRI and synovial pathobiology (not relevant to task), 4 because they did not include patients with RA, and 6 because they were abstracts only with no full text (Supplementary Table 5, available from the authors on request). Eighteen articles were then identified that satisfied the eligibility criteria and were therefore included in the review.
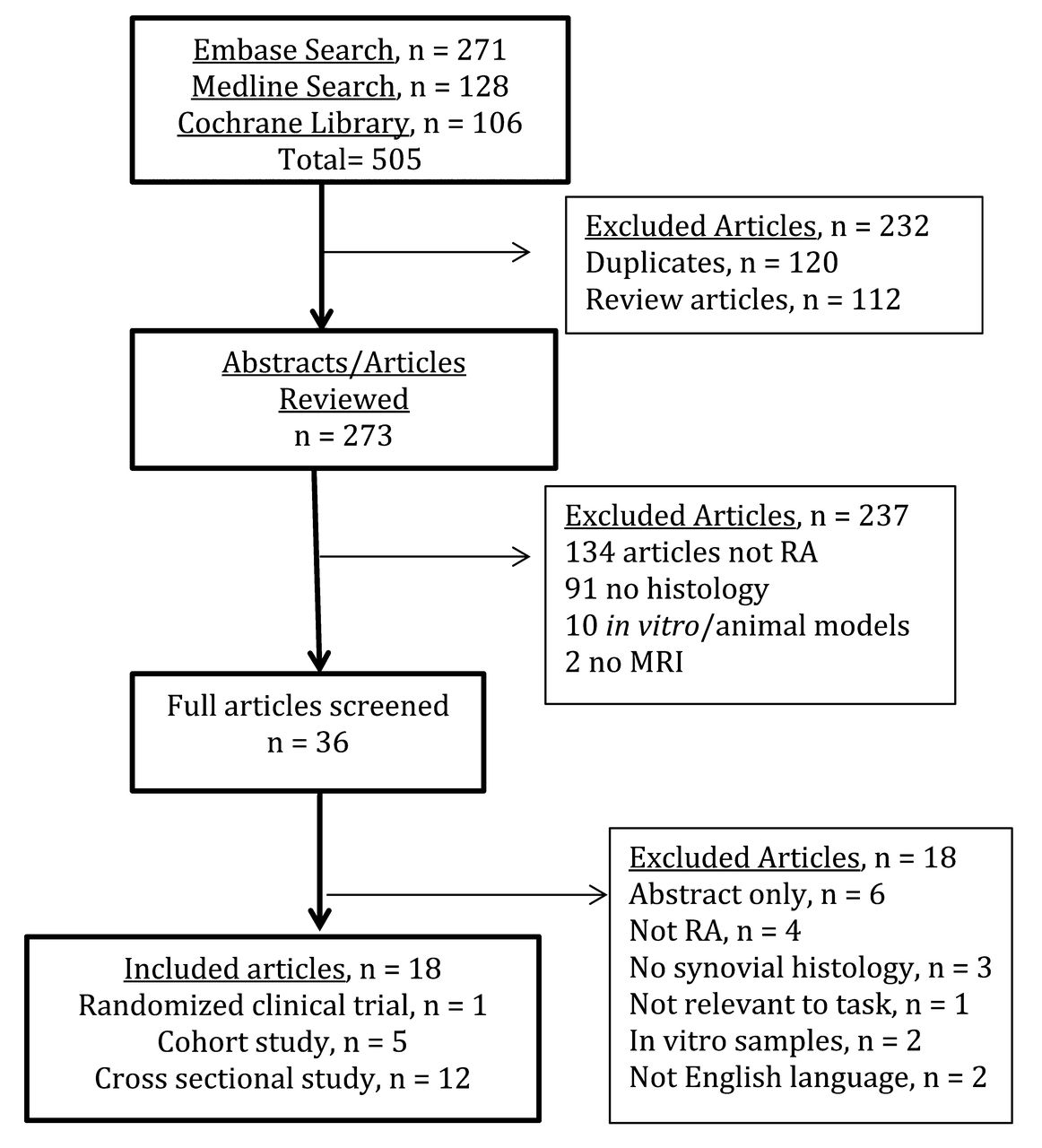
PRISMA flow chart presenting the results of the search strategy. PRISMA: Preferred Reporting Items for Systematic reviews and Meta-Analyses; RA: rheumatoid arthritis; MRI: magnetic resonance imaging.
Characteristics of included studies
A summary of the characteristics of the 18 studies is presented in Table 2 (MRI characteristics) and Table 3 (histopathobiological characteristics)21–30,31,32,33,34,35,36,37,38,39. A total of 442 participants were included in the analyses from the 18 studies. Of these, 327 had RA, 19 spondyloarthropathy, 4 psoriatic arthritis, 55 osteoarthritis, 2 healthy controls, and 35 other arthritic conditions. Eleven studies were cross-sectional observational studies21–30,31 and 1 study was a retrospective analysis32. Four studies were prospective open-label clinical trials33,34,35,36, 1 study was a blinded RCT37, and 1 study was a prospective observational clinical study38. Fifteen studies included patients only with established RA (although exact disease duration was not specified in 2 of these studies31,35) and 3 studies specifically included patients with disease duration of < 2 years26,36,38. Fourteen studies sampled synovium from the knee joint and 4 studies included samples from small joints26,31,32,35. Variable methods for synovial sample retrieval were reported: 7 studies using arthroscopy29,31,33,34,36,37,38, 4 arthroplasty21,27,28,32, and 3 using both22,23,30. Two studies used blind needle biopsy24,25 and 2 miniarthroscopy (Table 2)26,35. Acquisition of images was performed on a 1.5T MRI scanner with contrast administration in 13 studies21,22,23,26,27,28,29,30,32,33,34,36,37 and without in 1 study38. Two studies used a 0.5T + contrast administration24,25 and 2 a 3T+ contrast protocol31,35, although the latter study used a 0.2T scanner in a significant proportion of patients (4/10) with claustrophobia (Table 2).
Summary of studies directly correlating MRI features with synovial pathobiology: MRI characteristics.
Summary of studies directly correlating MRI features with synovial pathobiology: histobiological characteristics.
Quality assessment of studies
A summary of quality scoring of studies is provided in supplementary data (Supplementary Table 4, available from the authors on request). Quality scores were converted to percentages of the maximum score within each class of study. The mean (range) quality score was 56% (25–75) for cross-sectional studies and 68% (46–93) for cohort studies indicating a broad range of scores. The 1 RCT had a quality score of 71%.
Synovitis
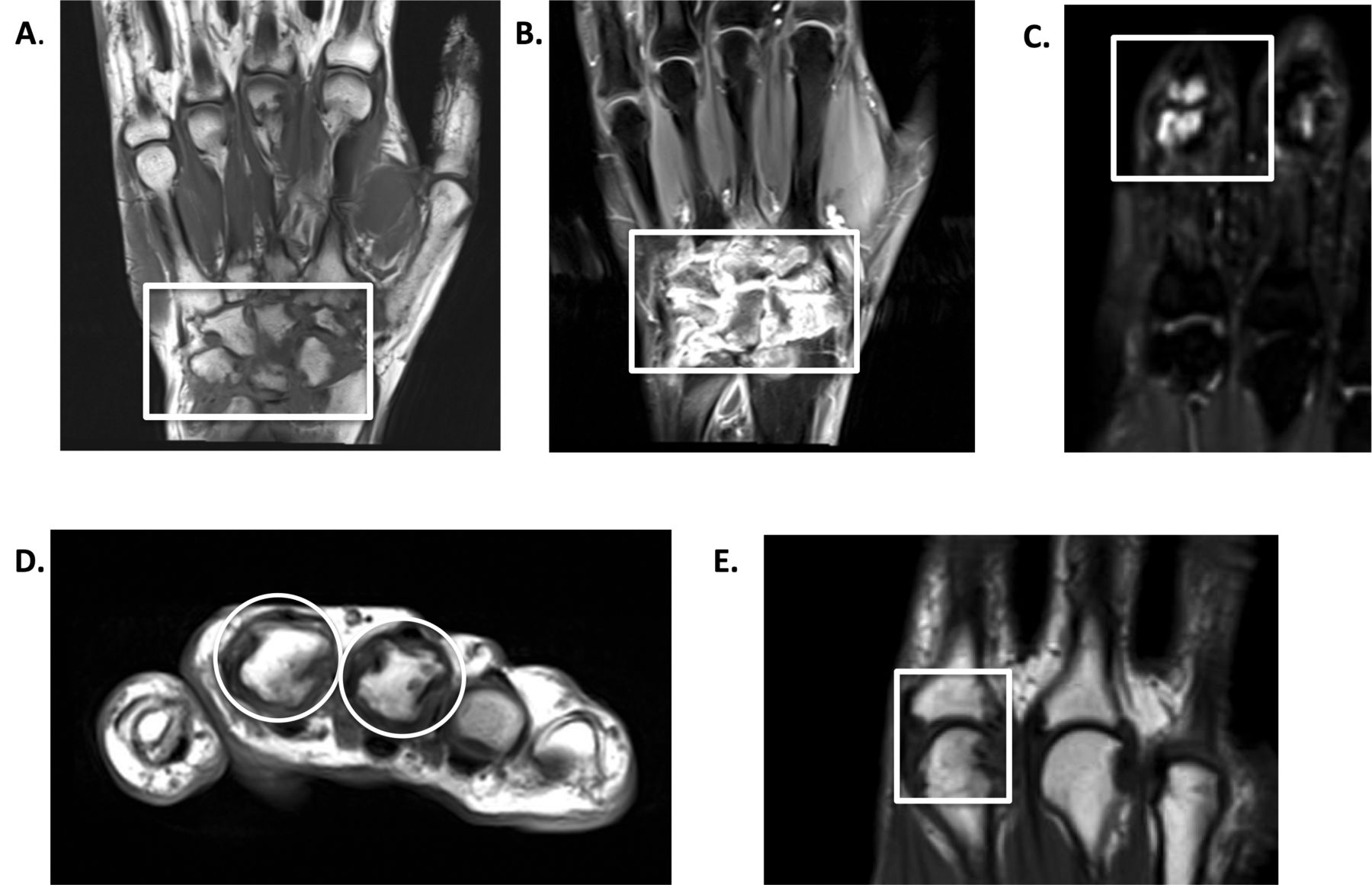
MRI synovitis can be assessed by static and dynamic protocols. Subsequent to the acquisition of T1-weighted images (Figure 2A), static protocols assess the volume of enhancing synovitis following the administration of a Gd-based contrast agent (Figure 2B) at a fixed timepoint. Synovitis volume can then be assessed manually or using a semiautomated method by outlining the synovial tissue. Static images can also be assessed using the widely validated semiquantitative Outcome Measures in Rheumatology (OMERACT)-Rheumatoid Arthritis Magnetic Resonance Imaging Scoring (RAMRIS) synovitis score40. Dynamic contrast-enhanced (DCE)-MRI involves the rapid acquisition of sequential images during and after administration of contrast and assesses rate of enhancement of synovial tissue. Results can be influenced by factors such as synovial perfusion and capillary permeability; thus, dynamic versus static protocols may be able to more sensitively reflect local synovial inflammatory activity41,42.
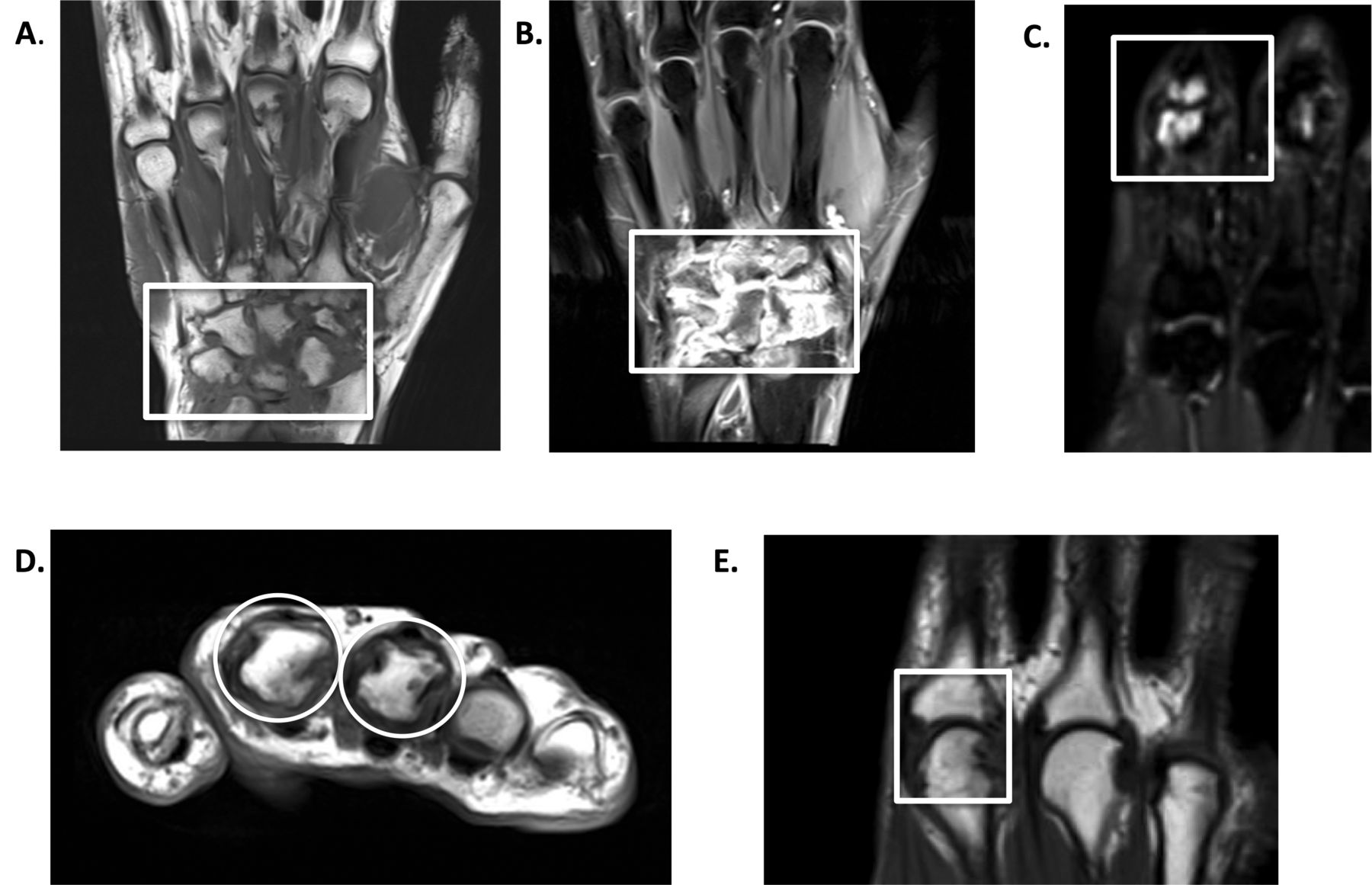
Assessment of RA joint abnormalities by magnetic resonance imaging. Coronal T1-weighted (A) image of wrist joint demonstrating extensive synovial thickening that enhances following administration of gadolinium (B). (C) T2 fat-suppressed coronal image demonstrating bone marrow edema within the head of the proximal and base of the middle phalanx. (D) Axial T1-weighted image demonstrating erosions of bone cortex within second and third metacarpal heads. (E) Coronal T1-weighted image of MCP joints demonstrating significant joint space narrowing within second MCP joint. RA: rheumatoid arthritis; MCP: metacarpophalangeal.
Does MRI synovitis reflect histopathological inflammation?
Sixteen studies were identified that directly examined the relationship between the degree of MRI synovitis and local synovial pathobiology21,22,23,24,26,27,28,29,30,31,32,33,34,35,36,37. Macroscopic synovitis and MRI synovitis was assessed in 3 studies both semiquantitatively22 and using dynamic MRI protocols34,37 with all 3 suggesting a significant correlation between macroscopic and MRI synovitis. Six studies21,22,23,24,28,31 using dynamic MRI and 3 studies26,27,32 using static MRI protocols also directly examined the relationship between MRI-determined synovitis and synovial inflammation assessed microscopically following routine H&E staining. Eight out of 9 of these studies21,22,23,24,26,27,28,31 concluded that histological inflammation correlated with either semiquantitative or DCE-MRI synovitis. Although immunohistochemical analysis of the synovial cell infiltrate was performed in 7 studies27,29,31,33,35,36,37, only 6 directly reported the relationship between histological markers and synovitis with a significant relationship reported between MRI synovitis and CD4+ T cells37, CD68+ sublining macrophage number27,29,31, cell proliferation (Ki67)27, and neoangiogenesis (CD31)27. Three of the 4 studies also reported a significant relationship between MRI synovitis and degree of histological vascularity through semiquantitative assessment of H&E stained tissues30 expression of the neoangiogenesis marker CD3127, endothelial cell marker QBend3025, and von Willebrand factor expression36. Conversely, Vordenbäumen, et al35 reported no significant relationship between either sublining macrophage number or vascular endothelial growth factor (VEGF; an immunhistochemical marker of vascularization) and RAMRIS synovitis.
Does MRI synovitis identify modulation of synovial pathobiology following effective therapeutic intervention?
Longitudinal data examining whether MRI is sensitive enough to detect modulation of histological synovitis following effective therapeutic intervention was evaluated in 4 studies incorporating serial MRI scans and paired synovial biopsies. First, an open-label placebo-controlled study of intraarticular anti-CD437 reported a significant correlation between MRI synovitis and macroscopic synovitis with a trend toward improvement in both histological and MRI synovitis only in patients receiving active treatment. Second, Buch, et al33 in a prospective open-label trial reported on the synovial effect of abatacept in a cohort of 13 patients. Although the study did not report directly on the relationship between modulation of MRI synovitis and synovial histology, it did report on the relationship between synovial gene expression and MRI synovitis, documenting a significant association between downregulation of the T cell cytokine interferon-γ and reduction in MRI synovitis scores in responders to treatment. Third, a prospective open-label trial of 16 patients with RA investigated the effect of tumor necrosis factor (TNF) inhibitor therapy on hypoxia, macroscopic and microscopic synovial inflammation, and MRI synovitis34. Patients underwent a baseline needle arthroscopic synovial biopsy and DCE-MRI of the knee, both of which were repeated 3 months after starting anti-TNF therapy. The study demonstrated a significant inverse relationship between hypoxia and clinical response to anti-TNF therapy. The investigators also looked directly and found a significant relationship between macroscopic synovitis/vascularity and MRI synovitis. There were also significant associations demonstrated between falls in CD4+ T cells and CD68+ sublining macrophages and MRI synovitis. Finally, Vordenbäumen, et al35 reported results from 6 patients who underwent sequential metacarpophalangeal (MCP) joint biopsy and MRI and found no significant association between change in sublining macrophage number and RAMRIS synovitis score, although given the small sample size the significance of the results is unclear.
The data identified within our review provides an initial basis for the use of MRI as a surrogate measure of histological synovitis. Of particular importance is the relatively consistent demonstration of a significant relationship between CD68+ sublining macrophage number and MRI synovitis, the only current synovial biomarker validated as a measure of disease activity43. However, it is also important to consider a number of limitations when interpreting results from these studies21,22,23,25,26,27,28,29,30,35,37. First, it is now recommended that to overcome significant synovial pathological heterogeneity, 6 synovial samples from different sites should be analyzed for large joint procedures44 and 4 for small joints45. Although 10 studies reported number of synovial samples retrieved per procedure21,22,23,26,28,30,33,35,37,38, only 4 cohorts reported retrieving 6 or more biopsies30,31,33,35. Further, only a selected number of studies specified a biopsy site predetermined by the MRI21,22,23,28,30,37 and so were able to directly compare local synovial pathology. Synovial pathology is also influenced by disease course as well as therapeutic intervention46,47,48 factors that were not routinely controlled for in a number of studies21,22,23,28,30,32 because a wide variability in time from MRI assessment to synovial sampling was reported. In addition, only 2 studies21,29 reported that intraarticular steroid injections were not permitted in this period and only 3 studies29,33,37 controlled doses of steroids and DMARD prior to study inclusion. It should also be noted that the majority of studies identified harvested synovial tissue from arthroplastic knee joint procedures21,22,23,27,28,30,32, which restricts sampling of tissue to endstage joints. Indeed, there were only limited data evaluating pathobiology at distinct disease stages from homogeneous cohorts, with only 1 study29 including patients specifically with disease duration of less than 1 year and only 2 studies26,38 including patients with disease duration of less than 2 years26,38. Importantly, of the 18 studies identified, 13 sampled knee joints, with only 426,31,32,35 examining the relationship in small joints.
Bone marrow edema
MRI is unique among currently available imaging modalities in its ability to detect BME (Figure 2C) and although outside the remit of our systematic review, it is worth noting that BME has been shown to equate to histological osteitis49. Importantly, the occurrence of BME has been tightly correlated with the presence of synovitis50; however, whether BME is driven and/or maintained by synovial pathobiological signals is unknown and very limited data examining this relationship were identified. Takase, et al27 report that in a cohort of 15 patients with RA, no significant relationship between histopathological changes of inflammation (neoangiogenesis, inflammatory cell infiltrates, and lining layer thickness) and MRI BME were found. In a further cohort of 7 patients in clinical remission32, no correlation between MRI BME and histological synovitis was reported; this is likely to be explained by the small number of patients within the study. Finally, in a cohort of 10 patients, Vordenbäumen, et al35 reported that synovial staining for VEGF significantly correlated with RAMRIS BME scores in MCP joints. Certainly, more complex synovial analysis in larger cohorts at different stages of disease will be required to fully interpret whether synovial signals are involved or required in the initiation and/or maintenance of BME.
Bone erosion
MRI has been increasingly recognized as a more sensitive marker of erosions (Figure 2D) than plain radiography51. The validation of the OMERACT-RAMRIS MRI score40 as a robust and sensitive tool to document presence and/or erosive progression in patients with RA suggests that incorporating MRI progression data with synovial pathobiology may reveal important signatures of disease. In 2 cross-sectional cohorts, Andarajah, et al32 reported in 7 patients with established RA no clear association between histological synovitis and erosions32, and Vordenbäumen, et al35 reported a significant relationship between synovial VEGF staining and the RAMRIS erosive score in MCP joints in 10 patients. Interpretation of the significance of these results is complicated by the small numbers, the cross-sectional approach, and the lack of validated MRI erosion score in the former report. However, in a prospective study of 60 patients, Kirkham, et al38 aimed to examine whether synovial pathobiology could explain joint damage progression, as assessed by progression in the OMERACT-RAMRIS score52. Although the authors identified no specific synovial histological features, using multivariate analysis of gene expression they identified interleukin (IL)-1, TNF-α, IL-17, and IL-10 as predictive of joint damage progression. The study had a number of limitations: (1) a wide range of disease durations in patients recruited to the study, (2) lack of control of concomitant disease-modifying therapies, and (3) joint damage progression in the small joints of the hands was related to distant synovial sampling sites in the knee. Notwithstanding this, the report is highly instructive in identifying synovial mediators of joint damage progression and it remains important, therefore, to validate the results in further larger cohorts of therapy-naive patients with early RA.
Cartilage loss
Cartilage loss in RA can be assessed by documenting joint space narrowing (JSN) on plain radiographs as well as MRI (Figure 2E). However, no data were identified within this systematic review to examine the relationship between cartilage loss and synovial pathobiology.
DISCUSSION
MRI has significant advantages over other imaging techniques for patients with RA; it does not expose patients to ionizing radiation, it can sensitively detect synovitis, erosions, and JSN, and is unique in its capacity to detect BME. This differentiates MRI from ultrasound, which, although it is a sensitive measure of histological synovitis53, cannot detect BME and does not have validated outcome measures for cartilage loss or bone erosion. The clinical studies identified in this review indicate a significant relationship between histological and MRI evident synovitis, which is important to validate MRI as a tool to reliably assess synovitis without the need for invasive biopsy. Further, from the limited data available, a critical role for synovial pathways at least in driving joint damage38 seems likely but requires more extensive validation. However, overall the data provide limited information on the specific synovial pathobiological processes driving MRI abnormalities in RA.
Although the past decade has seen tremendous advances in the care of patients with RA, considerable challenges remain. These include (1) specificity/sensitivity of current diagnostic/classification criteria for RA, (2) prediction of prognosis following diagnosis of RA, and (3) limited biomarkers of response/resistance to biologic drugs. What is required is a move toward an era of personalized medicine for patients with RA with targeted treatment pathways from diagnosis, but this is only possible if critical pathways mediating both disease pathogenesis and clinical response to therapy are further elucidated. What our review highlights is the need to validate the relationship between synovial pathobiology and MRI abnormalities at the single joint level both in well-defined early and established RA cohorts and within clinical trial protocols of established and novel biologic drugs. This is particularly important because historical limitations such as the lack of sensitivity of clinical examination and radiographic assessment to detect synovitis and joint damage progression/cartilage loss, respectively, are largely overcome by the advent of a robust validated MRI score capable of assessing synovitis and erosion40 and potentially BME and cartilage loss54. Further, the advent of techniques such as ultrasound-guided synovial biopsy (Figure 3) that provide a technically simple, minimally invasive approach to tissue acquisition from small as well as large joints55, and more recent techniques to rapidly and simultaneously examine the expression of multiple genes, are likely to overcome challenges in sampling tissue from previously inaccessible joints and variability in histological assessment of synovial tissue.
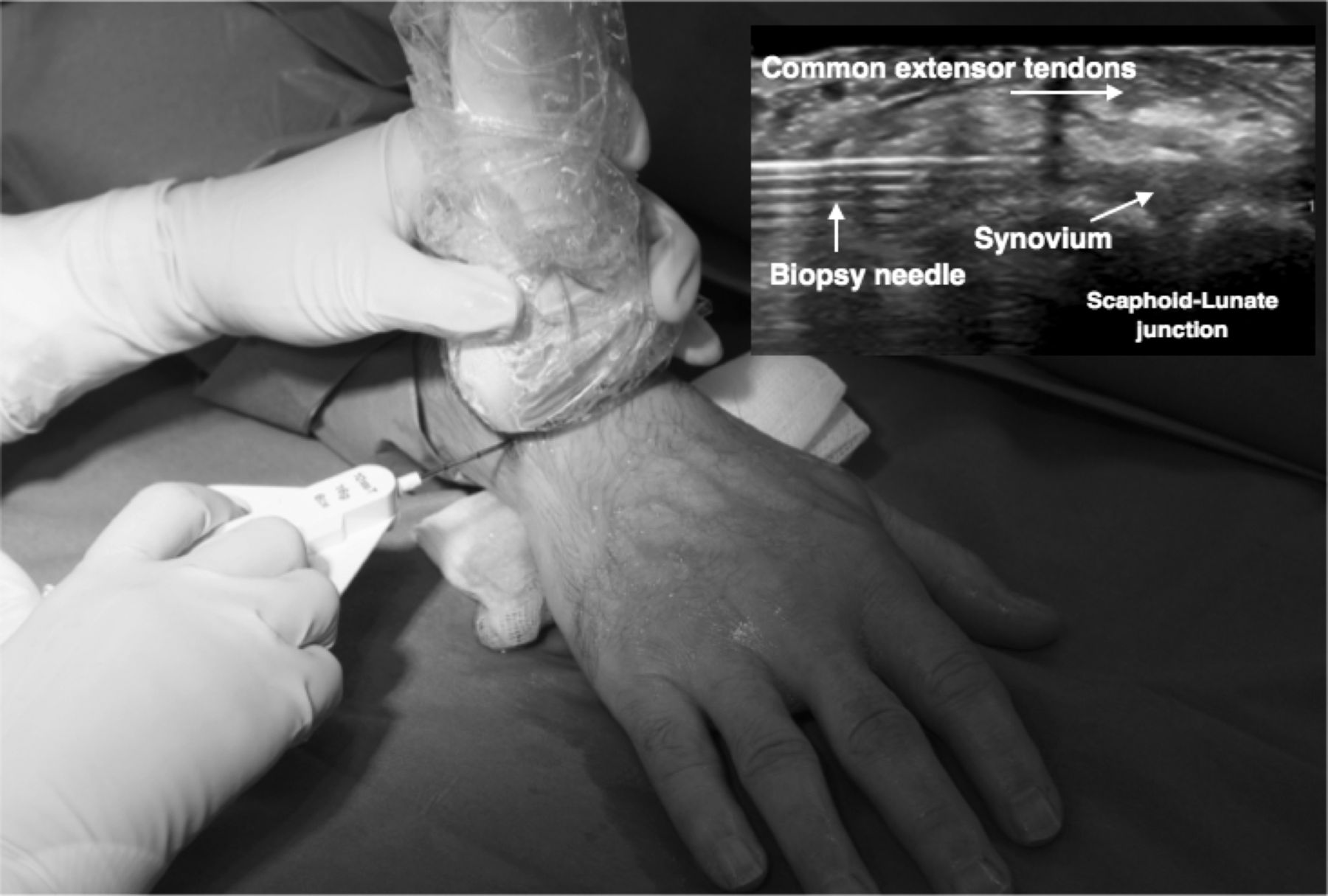
Minimally invasive technique of US-guided synovial biopsy of wrist joint. Inset depicts corresponding greyscale US image of biopsy needle inserted into wrist joint under extensor tendon complex. US: ultrasound.
Overall, the data identified within our systematic review validate MRI as a tool to assess synovitis, but very limited data directly examining the link between synovial pathobiology and joint damage/cartilage loss and BME were identified. Future research should focus on clinical trial protocols integrating synovial sampling with MRI imaging at different stages of disease to dissect critical synovial pathways mediating RA pathogenesis. Although understanding the interrelationship of these disease biomarkers offers the potential to enhance the predictive validity of modern imaging with concomitant synovial pathobiological analysis, further studies integrating MRI with synovial tissue analysis in well-controlled cohorts before and after therapeutic intervention are required to achieve this.
Footnotes
AB, MB, and PGC are supported in part by the NIHR Leeds Musculoskeletal Biomedical Research Centre.
- Accepted for publication May 11, 2017.








{kind=link}
{kind=link}
{kind=link}