

Diagnosis of primary angiitis of the central nervous system (PACNS) is a challenge for clinicians owing to the rarity of the disease and the lack of specific tests1. A targeted biopsy is recommended to maximize diagnostic potential2.
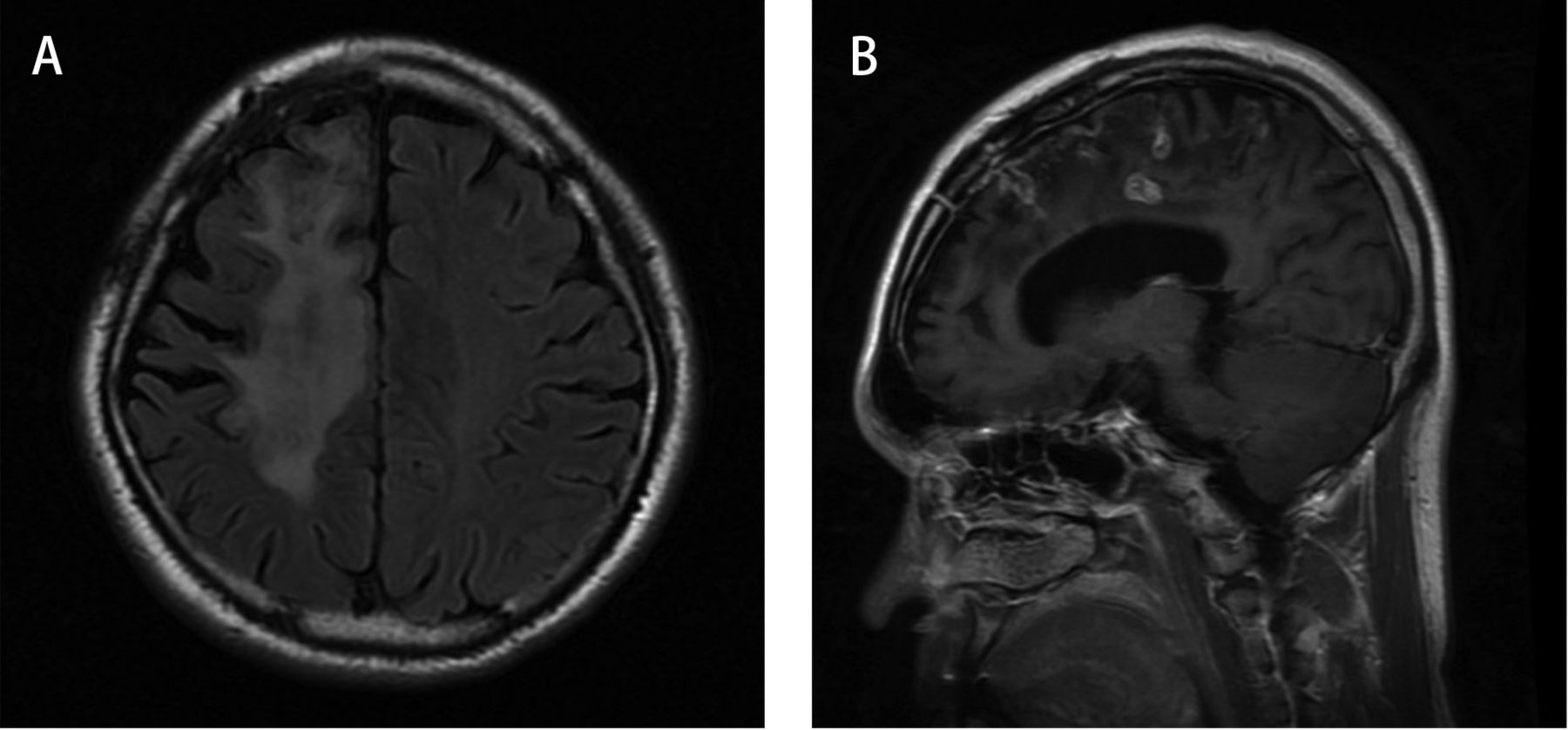
A 31-year-old worker from South China was admitted with a 7-year history of paroxysmal seizures with loss of consciousness and limb convulsions. He had a habit of eating lamb kebabs and reported no contact with pets. Laboratory findings showed a slightly elevated erythrocyte sedimentation rate (28 mm/h) and negative results from tests for human immunodeficiency virus, antinuclear antibody, and antineutrophil cytoplasmic antibodies. Magnetic resonance imaging of the brain demonstrated multifocal and migrate lesions constricted in the unilateral hemisphere and ring enhancement on T1 postcontrast imaging (Figure 1). The angiography was negative. A targeted resection of the temporal lobe lesions revealed destructive vasculitis with lymphocytic inflammation and fibrinoid necrosis. PACNS was suspected. However, a large dose of prednisone did not result in complete remission. A repeat examination of the biopsy specimen using both H&E and Gomori methenamine-silver stain identified many cysts containing small oval to round objects consistent with toxoplasmosis. Plasma cell infiltration was seen around vessel walls (Figure 2). Toxoplasma-specific IgG was detected in both serum and cerebrospinal fluid. A diagnosis of CNS vasculitis in association with toxoplasmosis was made and the patient responded well to antibiotic therapy.
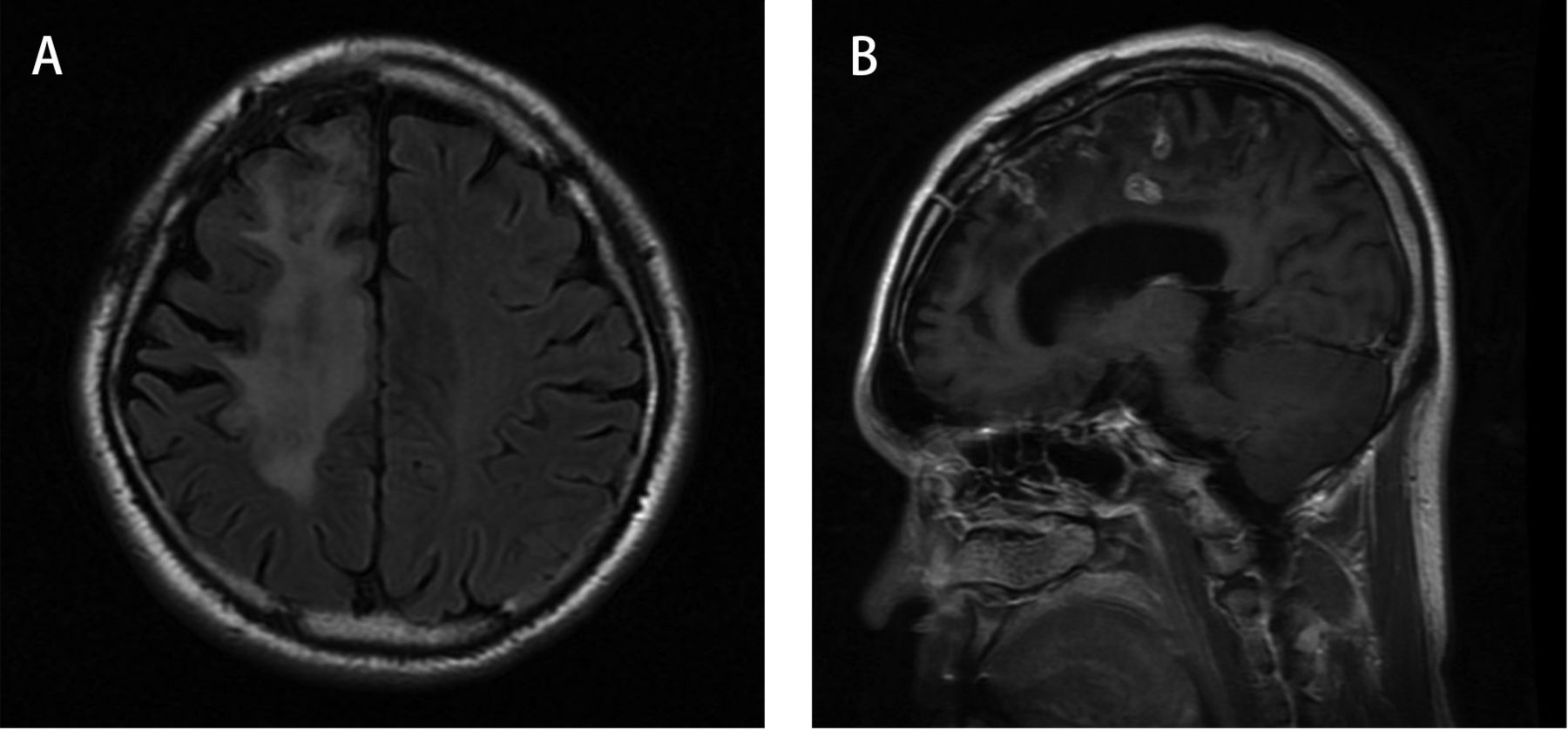
Brain magnetic resonance imaging. A. Extensive lesions restricted to the right cerebral hemisphere on fluid attenuated inversion recovery. B. Multiple foci of nodular and ring enhancement on T1 postcontrast imaging.

Vasculitis and Toxoplasma gondii in the brain tissue. A. Vasculitis: infiltration of lymphocytic inflammation in and around the vessel wall with large amounts of plasma cells in the brain (H&E). B. T. gondii: thin-walled cysts containing numerous black and oval to round particles (arrows; black dots, Gomori methenamine-silver staining).
We report the first documented case, to our knowledge, of CNS vasculitis associated with toxoplasmosis, in a patient with no known immunocompromise. Toxoplasmosis needs to be considered even in non-immunocompromised patients.








{kind=link}
{kind=link}