

Abstract
Objective. To compare systemic disease activity by validated tools, i.e., the European League Against Rheumatism Sjögren Syndrome Disease Activity Index (ESSDAI) and the Clinical ESSDAI (ClinESSDAI) scores, between primary Sjögren syndrome (pSS) with positive serum cryoglobulins and pSS without serum cryoglobulins.
Methods. There were 825 consecutive patients with pSS who were retrospectively evaluated.
Results. The ESSDAI and the ClinESSDAI scores were significantly higher in cryoglobulin-positive patients (p < 0.0001, for both scores). Cryoglobulinemia was significantly associated with these domains: constitutional (p = 0.003), lymphadenopathy (p = 0.007), glandular (p = 0.0002), cutaneous (p < 0.0001), peripheral nervous system (p < 0.0001), hematological (p = 0.004), and biological (p < 0.0001).
Conclusion. Cryoglobulin-positive patients show the highest systemic activity in pSS.
Primary Sjögren syndrome (pSS) is a chronic inflammatory autoimmune disease characterized by a chronic infiltration of exocrine glands, mainly salivary glands1. Disease spectrum is broad2. A subset of patients with extraglandular involvement, vasculitis, hypocomplementemia, and cryoglobulinemia may be at increased risk of lymphoma and mortality, thus requiring a close followup3,4.
Symptomatic cryoglobulinemic vasculitis is observed in about 3%–4% of pSS and it is closely linked to lymphoma5,6. In particular, cryoglobulinemia appears to be linked to mucosa-associated lymphoid tissue (MALT) lymphoproliferation in pSS, which is different from hepatitis C virus (HCV)–related cryoglobulinemic vasculitis. However, some key pathogenetic events are shared, e.g., the expansion of rheumatoid factor (RF)–positive B cell clones preferentially using definite heavy and light chain genes7.
Finally, cryoglobulins are often type II cryoglobulins and persistently positive in pSS with cryoglobulinemic vasculitis or lymphoma8. Overall, a heavier B cell commitment to cryoglobulin production appears to be linked to a higher risk of malignancy in pSS.
The objective of our study is to evaluate the clinical, histological, and biological differences between pSS with positive serum cryoglobulins and pSS without serum cryoglobulins. The new tools of European League Against Rheumatism Sjögren Syndrome Disease Activity Index (ESSDAI) and the Clinical ESSDAI (ClinESSDAI), recently introduced to standardize the evaluation of disease activity in pSS, have been herein applied.
MATERIALS AND METHODS
We retrospectively evaluated 825 consecutive patients with pSS from 5 centers, all fulfilling the American-European Consensus Group (AECG) criteria. Data were collected regarding sex, age at diagnosis, fulfillment of each item of the AECG criteria, antinuclear antibodies (ANA), RF, low complement factor 3 (C3), low C4, cryoglobulins, ESSDAI, and ClinESSDAI. Determination of laboratory variables was described elsewhere5. The patients were negative for anti-HCV antibody and were tested for serum cryoglobulins at least twice9. This group of patients corresponded to 83.1% of the whole population. In each center, once the diagnosis of pSS had been made, serum cryoglobulins were routinely tested and then in the followup according to clinical judgment to stratify the patient risk profile to lymphoma development. Cryoglobulin-positive patients with pSS were defined if they presented persistent positivity of serum cryoglobulins (i.e., if they showed 2 consecutive positive results). Disease activity at diagnosis was identified by the ESSDAI10 and ClinESSDAI scores11.
There were 786 women (95.3%), and the cohort had a mean age of 52 ± 14 years. The focus score, defined as the number of inflammatory infiltrates of at least 50 cells present in 4 mm2 of gland surface unit12, was available in 258 patients (31.3%) and was 2.4 ± 1.9. Median ESSDAI was 6 (range 0–63) and median ClinESSDAI was 6 (range 0–60).
Descriptions of the single ESSDAI domains involved are reported in Table 1.
Clinical, histological, and serological features. Values are n (%) unless otherwise specified.
Missing data accounted for < 1%. No differences regarding the number of laboratory tests or lip biopsies were observed between cryoglobulin-positive and cryoglobulin-negative patients (data not shown).
Comparisons between cryoglobulin-positive and cryoglobulin-negative groups were performed by applying parametric or nonparametric tests for independent samples after verifying the assumption.
Approval for data collection and sharing was obtained by informed consent in each center. To protect patient privacy, anonymizing was guaranteed by using only numeric symbols in the database to identify each patient. Approval by the local ethics committee was not required in accordance with the policies of our institutions.
RESULTS
Seventy-three patients were positive for serum cryoglobulins (8.8%). No differences were observed regarding age at diagnosis and sex (Table 1).
Global systemic disease activity
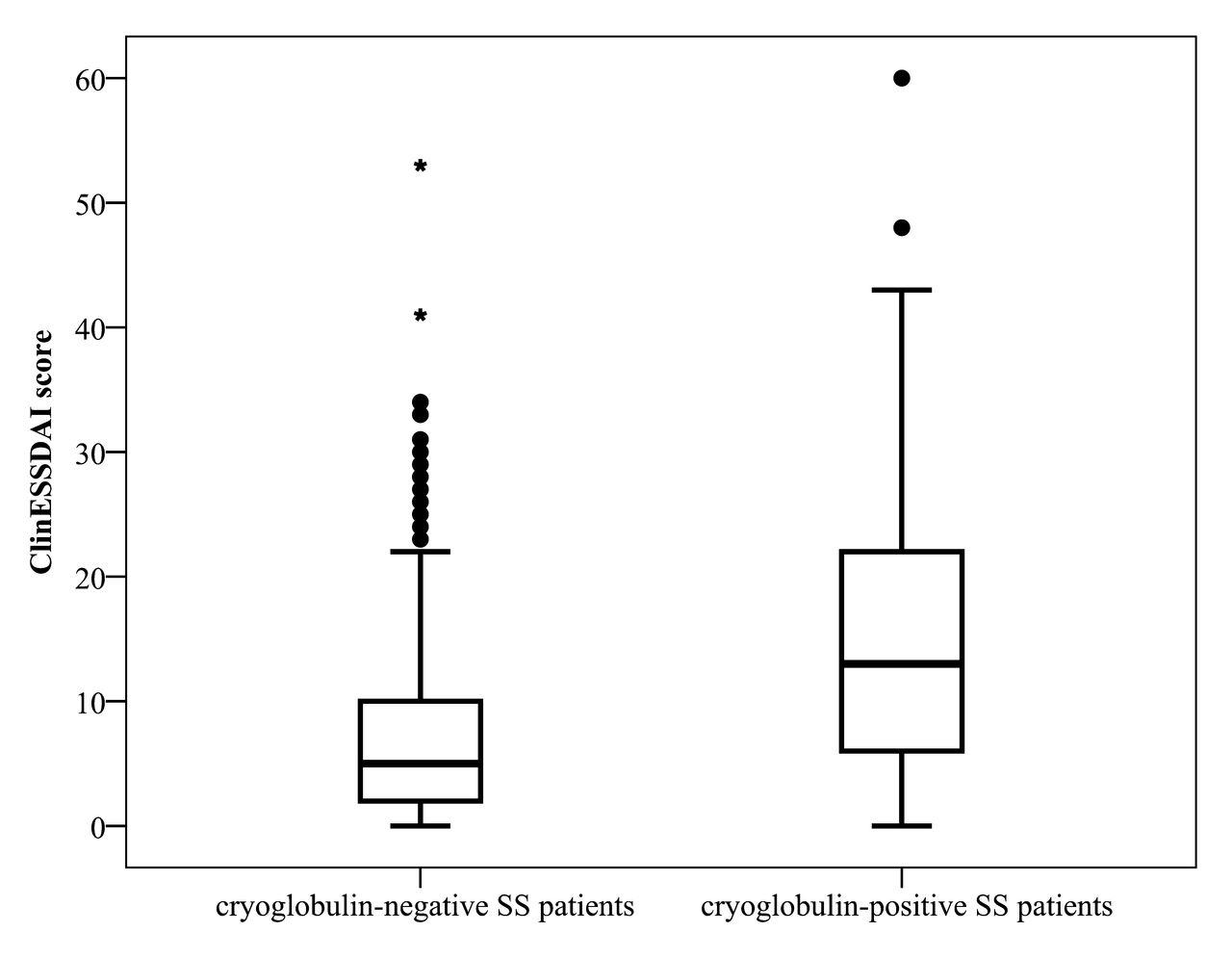
The ESSDAI score and the ClinESSDAI score were significantly higher in cryoglobulin-positive patients (p < 0.0001 for both scores by Mann-Whitney U test; Table 1 and Figure 1).
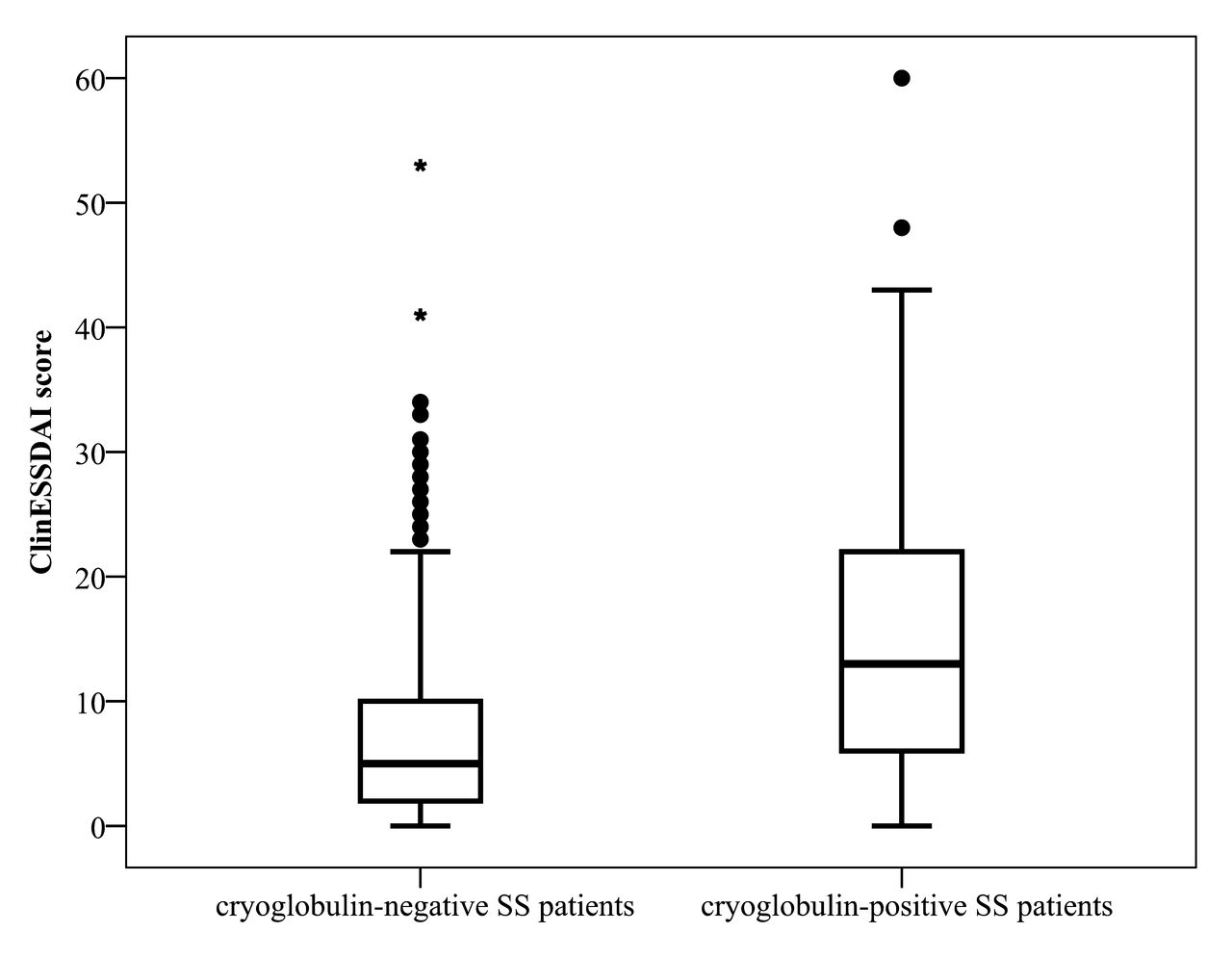
The ClinESSDAI score comparison between SS with or without cryoglobulinemia. EULAR: European League Against Rheumatism; ClinESSDAI: Clinical EULAR Sjögren Syndrome Disease Activity Index; SS: Sjögren syndrome.
Single ESSDAI domain involvement
Cryoglobulin-positive patients showed a higher rate of involvement in the following ESSDAI domains: constitutional (p = 0.003 by Pearson chi-square), lymphadenopathy (p = 0.007 by Pearson chi-square), glandular (p = 0.0002 by Pearson chi-square), cutaneous (p < 0.0001 by Pearson chi-square), peripheral nervous system (p < 0.0001 by Fisher’s exact test), hematological (p = 0.004 by Pearson chi-square), and biological (p < 0.0001 by Pearson chi-square; Table 1).
Because the single domains of the ESSDAI score may not be independent of one another, an analytical multivariate analysis was performed by considering the presence of serum cryoglobulins as the independent variable, while the following clinical domains selected from the univariate analyses were the dependent variables: constitutional, lymphadenopathy, glandular, cutaneous, and peripheral nervous system. Notably, besides the cutaneous domain (as expected by the presence of purpura, a typical sign of cryoglobulinemia), the glandular domain was also selected (OR 7.4, 95% CI 4.3–12.5, p < 0.0001, and OR 2.4, 95% CI 1.4–4.0, p = 0.002, respectively).
Histologic infiltrate in the minor salivary glands
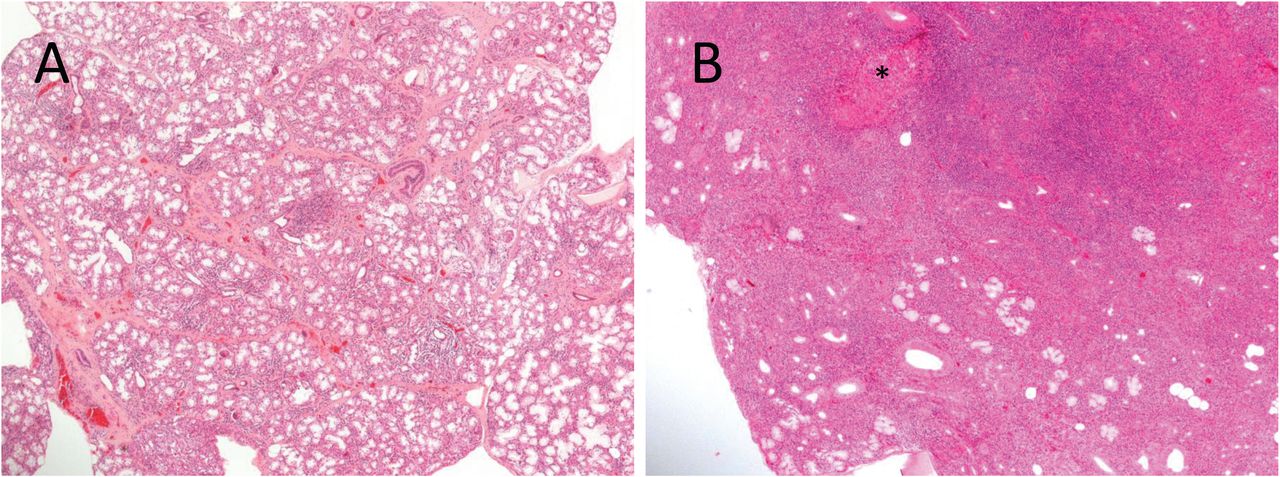
Focus score was significantly higher in cryoglobulin-positive patients (p = 0.022 by Mann-Whitney U test; Table 1, Figure 2A, and Figure 2B).
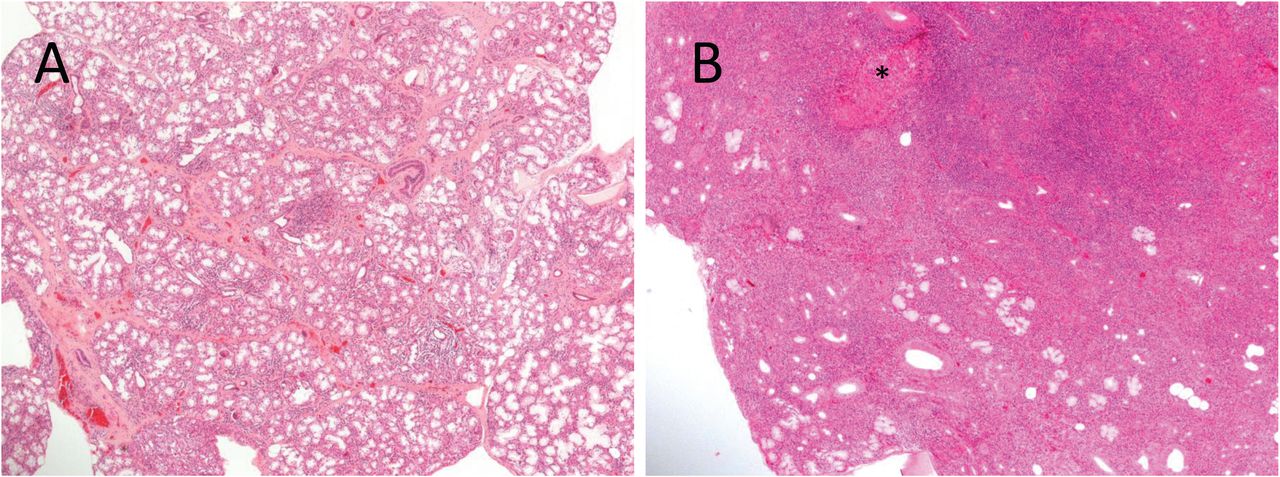
(A) Example of lip biopsy showing a low focus score in a patient with SS without cryoglobulinemia (H&E staining, 40× magnification). (B) Example of lip biopsy showing a high focus score in a patient with SS with cryoglobulinemia. * A myoepithelial island is highlighted (H&E staining, 40× magnification). SS: Sjögren syndrome.
Serologic profile
Interestingly, cryoglobulin-positive patients showed a significantly higher rate of positivity of anti-SSB/La antibody (p < 0.0001 by Pearson chi-square), while positivity for anti-SSA/Ro was slightly higher (p = 0.02 by Pearson chi-square). Additionally, in cryoglobulin-positive patients, ANA positivity (> 1:40) was significantly higher (p = 0.005 by Pearson chi-square), as well as RF (p < 0.0001 by Pearson chi-square), low C3 (p < 0.0001 by Pearson chi-square), and low C4 (p < 0.0001 by Pearson chi-square), as largely expected for these last 3 variables given the presence of serum cryoglobulins (Table 1).
DISCUSSION
Primary SS is usually considered an indolent systemic autoimmune disease, affecting quality of life rather than mortality4. However, a subset of patients requires a closer followup owing to a higher risk of complications5. This subgroup of patients is clearly identified by some serological hallmarks, such as hypocomplementemia, lymphopenia, anti-SSB/La autoantibody, monoclonal gammopathy, increased titers of RF, and cryoglobulinemia13,14. In particular, cryoglobulinemia can help the clinician to identify patients with pSS at high risk of extraglandular manifestations and lymphoma15,16. Because many targeting therapies would be available for pSS, defining different subsets of disease is very important, and serological markers might help in the early identification of patients who are candidates to receive treatments to prevent the development of complications14.
The aim of our study was to compare patients with pSS with or without serum cryoglobulins by using validated tools to assess disease activity in pSS (i.e., ESSDAI and ClinESSDAI).
Our data demonstrated that systemic disease activity was higher in pSS with serum cryoglobulins. Importantly, it was confirmed by also applying the ClinESSDAI score, which was derived from the ESSDAI score after excluding the biological domain, where cryoglobulinemia is present11, thus avoiding redundancy. Notably, the ESSDAI domains significantly linked to the presence of cryoglobulinemia were not only those obviously related to the clinical appearance of cryoglobulinemic vasculitis (i.e., constitutional, cutaneous, peripheral nervous system), but also those domains that represent local proliferation of MALT in pSS (i.e., glandular). This feature was even noted at the multivariate level of significance. Thus, a link between B cell expansion in MALT tissue, presence of serum cryoglobulins, and systemic disease activity may be highlighted, supporting the hypothesis that the biologic background of cryoglobulinemia in pSS is lymphoproliferation of MALT17. The herein reported observation of a higher focus score in cryoglobulin-positive patients with pSS can support this conclusion. This is not surprising, since ectopic germinal center-like structures in the minor salivary glands have been associated with lymphoma development in pSS18 and the focus score appeared to be independently associated with lymphoma19. Finally, cryoglobulin-positive patients explained the highest level of systemic biologic activity. Thus the key prognostic value of cryoglobulins in pSS suggests that all patients should be tested for serum cryoglobulins at least at the time of pSS diagnosis, and the test should be repeated during the followup in all patients presenting a suspicion of vasculitis or lymphoma. Moreover, anti-SSB/La autoantibodies were significantly linked to cryoglobulinemia. Thus, the positivity of anti-SSA/Ro and anti-SSB/La antibodies may have a greater prognostic significance as a hallmark of a more aggressive pSS subset with more pronounced B cell proliferation20, and physicians should be alert for possible cryoglobulinemia in pSS.
Practically, given that difficulties may arise in real-world settings with the measurement of serum cryoglobulins, patients with pSS could be removed from this analysis if they are at low risk of cryoglobulin positivity, i.e., RF-negative with normal levels of serum complement fractions, or RF-negative and anti-SSA/Ro and anti-SSB/La–negative.
Because our study was retrospective, a selection bias may have occurred. Patients with cryoglobulins would have had deeper and more extensive laboratory testing and clinical evaluation because of the known association of cryoglobulins with extraglandular manifestations and lymphoma in pSS. However, the frequency of serum cryoglobulins in the whole cohort was almost 9%, consistent with previous data2, and the number of patients who had a lip biopsy, as well as an extensive laboratory evaluation, did not differ between cryoglobulin-positive and cryoglobulin-negative patients.
Cryoglobulinemia in pSS is a clear red flag for a possible progression of the disease from an indolent to an aggressive state. The test should be done for all patients at diagnosis and possibly repeated in the followup according to the clinical indication. Glandular swelling and lymphadenopathy are linked to cryoglobulinemia, thus the need is reinforced to target MALT to prevent lymphoma and extraglandular manifestations in pSS14.
Acknowledgment
We thank our pathologist Cathryn Anne Scott, MD, for providing the histopathologic images, and Professor Miriam Isola for her support in the statistical analyses.
- Accepted for publication April 4, 2017.








{kind=link}
{kind=link}