

Abstract
Objective. To ascertain whether strategies of treatment with a biological disease-modifying antirheumatic drug (bDMARD) are cost-effective in an English setting. Results are presented for those patients with moderate to severe rheumatoid arthritis (RA) and those with severe RA.
Methods. An economic model to assess the cost-effectiveness of 7 bDMARD was developed. A systematic literature review and network metaanalysis was undertaken to establish relative clinical effectiveness. The results were used to populate the model, together with estimates of Health Assessment Questionnaire (HAQ) score following European League Against Rheumatism response; annual costs, and utility, per HAQ band; trajectory of HAQ for patients taking bDMARD; and trajectory of HAQ for patients using nonbiologic therapy (NBT). Results were presented as those associated with the strategy with the median cost-effectiveness. Supplementary analyses were undertaken assessing the change in cost-effectiveness when only patients with the most severe prognoses taking NBT were provided with bDMARD treatment. The costs per quality-adjusted life-year (QALY) values were compared with reported thresholds from the UK National Institute for Health and Care Excellence of £20,000 to £30,000 (US$24,700 to US$37,000).
Results. In the primary analyses, the cost per QALY of a bDMARD strategy was £41,600 for patients with severe RA and £51,100 for those with moderate to severe RA. Under the supplementary analyses, the cost per QALY fell to £25,300 for those with severe RA and to £28,500 for those with moderate to severe RA.
Conclusion. The cost-effectiveness of bDMARD in RA in England is questionable and only meets current accepted levels in subsets of patients with the worst prognoses.
Rheumatoid arthritis (RA) is a chronic inflammatory disease characterized by progressive and irreversible joint damage, impaired joint function, pain and tenderness caused by swelling of the synovial lining of joints, and is manifested with increasing disability and reduced quality of life1. RA is associated with substantial costs both directly (drug acquisition and hospitalization) and indirectly because of reduced productivity2. RA has long been reported as being associated with increased mortality3,4 particularly as a result of cardiovascular events5. A range of biological disease-modifying antirheumatic drugs (bDMARD) is available with proven efficacy compared with conventional DMARD (cDMARD). However, these are expensive treatments, costing around £9000 per annum (US$11,120), so that decisions based on cost-effectiveness are particularly important. In England, the National Institute for Health and Care Excellence (NICE) makes recommendations on the use of new and existing medicines and treatments within the National Health Service (NHS). NICE guidance restricts the use of bDMARD to patients who have failed at least 2 cDMARD and who have a Disease Activity Score in 28 joints (DAS28) > 5.1. For treatment to be continued, patients need to demonstrate at least a moderate European League Against Rheumatism (EULAR) response by 6 months.
NICE reviewed guidance on the use of bDMARD to allow a comparison between interventions and to consider extending existing guidance to patients with less severe RA. This article reports the economic model structure, variable inputs, and estimated cost-effectiveness of sequences of bDMARD compared with no use of bDMARD undertaken by the Assessment Group. This work formed part of the evidence base used by NICE to form the guidance for Technology Appraisal 3756. The economic model differs from previously published models by other researchers in that it is based on EULAR response rather than American College of Rheumatology (ACR) responses, which are not used in UK clinical practice; it used nonlinear, Health Assessment Questionnaire (HAQ) score progression while taking cDMARD based on a comprehensive review and analysis of HAQ progression; it assesses the cost-effectiveness in moderate to severe and severe RA cases independently; and it allows fully incremental analyses of treatment strategies using different first-line bDMARD. This paper concentrates on the cost-effectiveness results for those patients who can tolerate methotrexate (MTX), with the results for strategies without MTX provided elsewhere7,8.
MATERIALS AND METHODS
Economic model
An economic model was developed to estimate the cost-effectiveness within England of sequences of bDMARD. The model is used to synthesize evidence from a range of sources, including clinical trials, to estimate the costs and health benefits of different treatments over patients’ lifetimes. The ratio of additional cost to additional health benefits, measured in quality-adjusted life-years (QALY), is the incremental cost-effectiveness ratio (ICER). The ICER is compared with a published threshold (£20,000 to £30,000 per QALY in this instance for NICE) to help determine whether new treatments will add more to population health than will be lost from the withdrawal of other NHS services. The conceptual model is depicted in Figure 1 and took an NHS and Personal Social Services perspective. The model used an individual patient, time-to-event approach with a lifetime time horizon with both costs and benefits discounted at 3.5% per annum, in accordance with NICE recommendations9. Individual patients were sampled with characteristics resembling those in the British Society for Rheumatology Biologics Register (BSRBR). An outline of the methods is provided here; Stevenson, et al7 has full technical details.

Conceptual simplified schematic drawing of the modeling process. EULAR: European League Against Rheumatism; NMA: network metaanalysis; NBT: nonbiologic therapy; HAQ: Health Assessment Questionnaire; DMARD: disease-modifying antirheumatic drug; bDMARD: biological DMARD; cDMARD: conventional DMARD; BSRBR: British Society for Rheumatology Biologics Register; ERAS: Early Rheumatoid Arthritis Study.
The population evaluated
Analyses were conducted separately for patients with moderate to severe RA (defined as those with a DAS28 score > 3.2 and ≤ 5.1) and for patients with severe RA (DAS28 > 5.1). Patients with prior experience of MTX were sampled using patient characteristics from the BSRBR for those receiving their first bDMARD, which allowed correlation to be maintained among the following characteristics: age, sex, disease duration, DAS28, previous DMARD, HAQ score, and weight. Details of the midpoint values and distributions are provided elsewhere7.
Strategies evaluated within the economic model
The focus of the NICE appraisal was on the cost-effectiveness of the initial bDMARD, which was 1 of adalimumab (ADA), etanercept (ETN), infliximab (IFX), certolizumab pegol (CTZ), golimumab (GOL), tocilizumab (TCZ), and abatacept (ABA). ABA was available in both subcutaneous (SC) and intravenous (IV) formulations. The remaining treatments after all first-line bDMARD were assumed to follow NICE guidance and were rituximab (RTX) + MTX, then TCZ + MTX (if TCZ + MTX was not used first-line), followed by a range of nonbiologic therapies (NBT), a term defined to encompass a selection of nonbiological treatments that clinicians may consider appropriate for individual patients, typically MTX and sulfasalazine10. All 7 bDMARD strategies were compared against each other, and with a strategy of cDMARD (MTX) followed by NBT. It was assumed that in accordance with NICE guidance, patients would have received at least 2 cDMARD before considering the use of a bDMARD11.
Efficacy of bDMARD, cDMARD, and NBT
Literature searching was performed with a cutoff date of July 2013, because the Assessment Group report was submitted to NICE in August 2013. For inclusion in the network metaanalysis (NMA), a study needed to present information on ACR and/or EULAR response between 22 and 30 weeks inclusive and needed to recruit patients with moderate to severe RA or severe RA. These studies were deemed generalizable to the patients modeled.
This article provides the results for studies conducted in patients without previous bDMARD experience: results including studies with a small proportion of bDMARD-experienced people are provided elsewhere7. An NMA, implemented within a Bayesian framework, was undertaken to synthesize both direct and indirect evidence on relative EULAR responses produced by each intervention and assuming that cDMARD could be grouped together. The analyses conducted for those with moderate to severe or severe RA were based on 16 randomized controlled trials12–20,21–29. Point estimates from the NMA for the interventions within the decision problem are shown in Figure 2. As expected, bDMARD are more efficacious than NBT. No EULAR data were available for ABA SC. Based on work undertaken by Malottki, et al30 the efficacy of RTX + MTX was set equal to that of ABA IV + MTX. It was assumed that NBT provided no EULAR response.

Proportions of patients with each EULAR response associated with each intervention. EULAR: European League Against Rheumatism; cDMARD: conventional disease-modifying antirheumatic drug; ABA IV: abatacept intravenous; ADA: adalimumab; CTZ: certolizumab pegol; ETN: etanercept; GOL: golimumab; IFX: infliximab; TCZ: tocilizumab; MTX: methotrexate.
The change in HAQ related to EULAR response
The change in HAQ score conditional on EULAR response was calculated using data from the BSRBR (2417 good EULAR responses and 5492 moderate EULAR responses). The average reductions in HAQ score were estimated to be 0.317 (SE 0.048) for moderate responders and 0.672 for good responders (SE 0.112).
The trajectory of HAQ while taking bDMARD or NBT
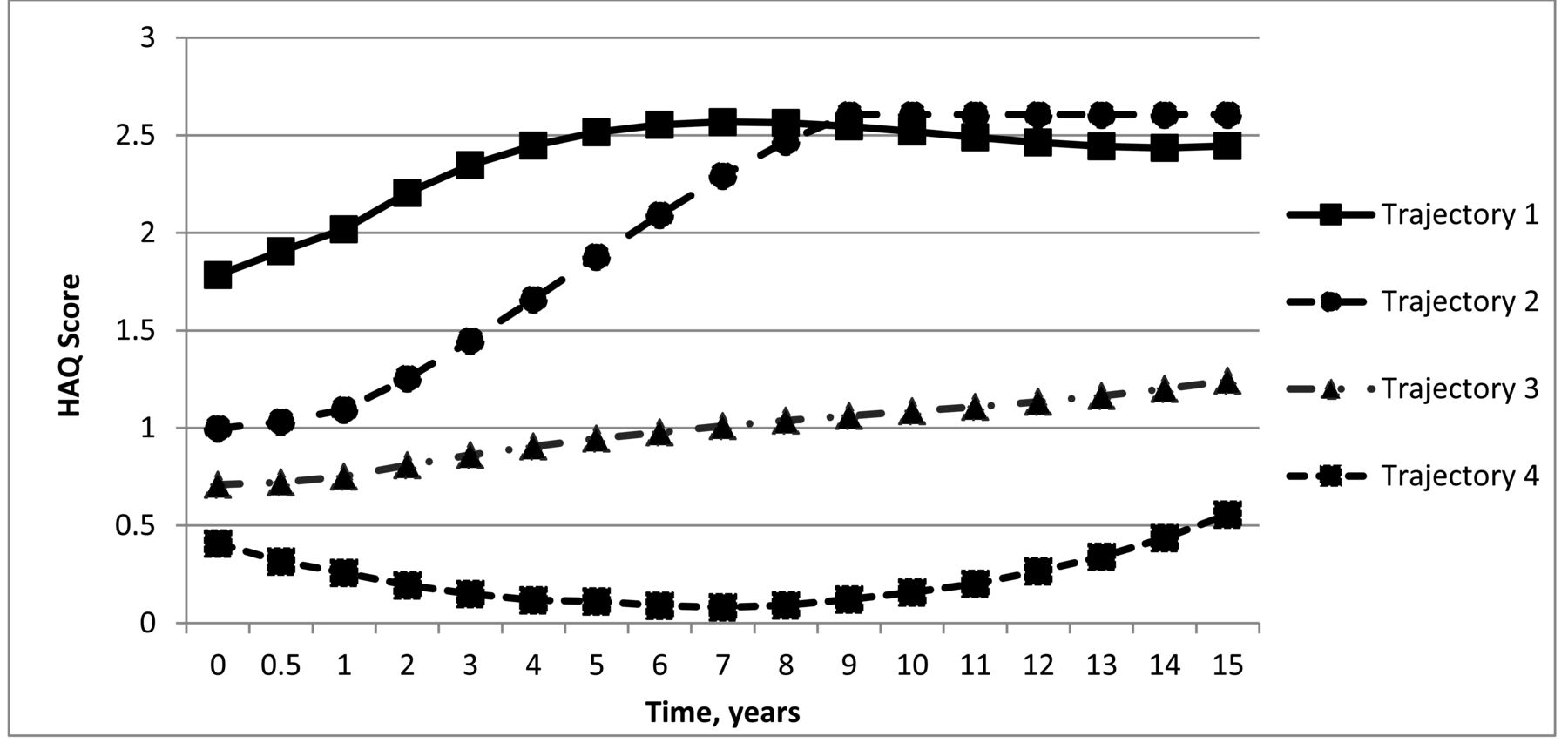
Three-year data from the BSRBR showed no evidence to challenge previous assumptions of no HAQ progression while a patient was taking a bDMARD. For those patients taking NBT, we used estimates from previous work by Norton, et al31. This work identified 4 distinct trajectories of HAQ in the Early Rheumatoid Arthritis Study (ERAS) and showed that the rate of HAQ worsening decreases over time. These analyses were re-run to incorporate covariates for patient characteristics (age, sex, disease duration, DAS28 score, and number of previous cDMARD); the results are shown in Figure 3. For each individual patient the probabilities of belonging to each trajectory were calculated, with the predicted HAQ progression being the weighted average of the 4 trajectories.

The trajectories used in the base case analyses for patients taking nonbiologic therapy. HAQ: Health Assessment Questionnaire.
Alternative analyses were also undertaken to evaluate the ICER if faster rates of HAQ progression were used. These analyses are described in detail in Gibson, et al32, which extended the approach of Norton, et al to assess the potential effect of patient dropout from the ERAS dataset on the 4 trajectories. We used the estimates that had the greatest rate of HAQ worsening over 15 years to illustrate a lower limit of the ICER. The HAQ trajectories for the Gibson, et al analysis are shown in Figure 4. There was a delay between the Assessment Group being submitted to NICE and the final appraisal decision because the NICE appraisal process was suspended until these additional analyses were completed. In both the base case and supplementary analyses, it was assumed that there was no further progression beyond 15 years, although a scenario was evaluated that allowed the rate of progression seen between years 12 and 15 in trajectories 3 and 4 to be continued until 40 years. While the data to inform HAQ progression were relatively dated and do not reflect current first-line cDMARD treatment, they were considered appropriate to represent NBT in a population who had received at least 2 prior cDMARD, and in the intervention strategy, bDMARD.
The trajectories used in the supplementary analyses for patients taking nonbiologic therapy. HAQ: Health Assessment Questionnaire.
The time to discontinuation of treatment and the assumed change in HAQ score post-discontinuation
The time to discontinuation of bDMARD treatment was estimated using the BSRBR. Separate analyses were undertaken for those with a good and moderate EULAR response with the γ-distribution providing the best fit from the parametric models considered (Weibull, exponential, log-logistic, log-normal, γ, Gompertz, and Weibull frailty models). The individual patient characteristics were used as covariates.
The median time to discontinuation was 1523 days for moderate responders and 3363 days for good responders. It was assumed that the distribution of time to discontinuation was equal for all bDMARD and also that this was applicable for cDMARD. Patients were not assumed to discontinue NBT. Further details are provided in Stevenson, et al7.
For all analyses it was assumed that any reduction in HAQ score provided by the initial response would be lost (commonly referred to as a rebound effect) once treatment was stopped.
Costs associated with treatment
The costs of each bDMARD and of MTX were taken from the British National Formulary33. The cost of MTX was assumed to approximate that of NBT. Both public (CTZ and GOL) and confidential (ABA and TCZ) Patient Access Schemes (PAS) were taken into consideration. In these PAS the first 12 weeks of CTZ treatment are provided free of charge, and 100 mg of GOL is provided at the same cost as 50 mg, while ABA and TCZ are provided at a discount from the list price. Monitoring and administration costs were also included as detailed in Stevenson, et al7.
Hospitalization costs and patient utility
The hospitalization cost data used in the model, conditional on HAQ score, are shown in Table 1. These data were taken from the AbbVie company submission34 and were derived from the Norfolk Arthritis Register database for Roche35. To calculate a patient’s utility, the mixture model proposed by Hernandez-Alava, et al was used36,37, which required the pain score for each individual to be simulated from the HAQ score. This method uses a much larger sample size including patients who span the entire range of disease; other published papers use methods that have been shown to lead to biased utility estimates.
The assumed annual hospitalization costs and the assumed hazard rate for mortality conditional on HAQ score. HR for mortality is applied to age and sex mortality rates.
Indirect costs
In line with the NICE reference case9, indirect costs such as lost productivity due to not working were not included in our analysis.
Assumptions regarding mortality
It was assumed that bDMARD treatment would not influence the rate of mortality. This assumption was based on Michaud, et al38, who concluded that changes in HAQ score did not contribute substantially to predictive values of mortality over and above the baseline values. The model assumes an increased hazard for mortality, compared with age and sex mortality rates39, associated with baseline HAQ score category. These HR are provided in Table 1.
Adverse events associated with bDMARD
A simple approach to estimating the effect of adverse events (AE) associated with bDMARD was taken. A review of AE associated with bDMARD estimated a serious infection was observed in 35 per 1000 patients (95% CI 27–46) compared with 26 per 1000 patients (no CI presented) in patients receiving placebo40. Therefore it was assumed that 9 people per 1000 would have a serious infection that was associated with a cost of £1479 per episode and a QALY loss of 0.012 as detailed in Pfizer’s submission to NICE41.
Ethical approval
Ethical approval was not required in accordance with the policy of the institutions concerned.
RESULTS
Because there were only small differences in the discounted costs and discounted QALY among many of the bDMARD sequences, the incremental cost-effectiveness ratio can be misleadingly volatile: accordingly, we present the average (median and mean) cost-effectiveness of the 7 bDMARD sequences compared with NBT. Unfortunately, the absolute discounted costs and QALY cannot be presented because of the risk of back calculation of commercial-in-confidence discounts. However, incremental QALY gains were between 1.5 and 2.0 and incremental costs were between £60,000 and £100,000. The ranges in the mean ICER of the individual bDMARD strategies were relatively small, spanning £39,100 to £42,200 for patients with severe RA and from £48,800 to £52,300 for patients with moderate to severe RA. The deterministic base case ICER (the median of the 7 mean ICER produced by the bDMARD strategies) for patients with severe RA is estimated to be £41,600 per QALY gained: for patients with moderate to severe RA the value is estimated to be £51,100. The mean ICER (assuming equal use of all potential first-line bDMARD and weighting the individual cost and QALY gains for the 7 strategies equally) were marginally lower, being £41,100 for patients with severe RA and £50,300 for patients with moderate to severe RA. Probabilistic results were similar to the deterministic results: the median (mean) ICER for patients with severe RA were £41,300 (£40,700) and £52,000 (£51,100) for patients with moderate to severe RA. All sensitivity analyses were run deterministically to reduce computational time required. The absolute costs and QALY gained for the TCZ first strategy differed from the remaining strategies because TCZ cannot be used after RTX, if TCZ was used as the first bDMARD.
Additional deterministic results are presented alongside the base case results in Table 2. Assuming that only those patients with fastest HAQ progression would be treated with bDMARD, the cost per QALY was reduced to below £30,000. This value is particularly important because it is a reported upper limit for cost-effectiveness by NICE for treatments that are not classed as “end of life” treatments6.
The estimated deterministic ICER for bDMARD strategies compared with a cDMARD strategy. All numbers rounded to the nearest £100 (US$122). Data are median (mean).
DISCUSSION
The results from our primary analysis indicate that the ICER of a bDMARD strategy is in excess of £40,000 per QALY for those patients with severe RA and more than £50,000 for those patients with moderate to severe RA. Data presented elsewhere show that the values for monotherapy and for using bDMARD before cDMARD are greater than for our base case analyses7. All these values are greater than the threshold typically used by NICE for determining whether treatments should be recommended. However, there may be a number of factors that could reduce the ICER. These include the emergence of biosimilars — 2 biosimilars for IFX and 1 for ETN have already entered the UK market at prices below that of the branded equivalent; intensive treatment with cDMARD may prevent those with the least severe prognosis, in terms of HAQ increase, being provided with bDMARD as argued by clinical experts in the appraisal process; the possible reduction in the dose of bDMARD for those in low disease activity or remission as summarized by Kuijper, et al42 and Simpson, et al43; and any potential mortality benefit associated with bDMARD treatment. Factors that could increase the ICER include the possibility that second-line and third-line bDMARD treatments are less efficacious than if they were used as a first-line bDMARD; there may be HAQ increases while taking bDMARD; and the duration of treatment of people with no EULAR response (analysis of BSRBR data shows that a quarter of nonresponders had more than 4 years of treatment)7. Exploratory analyses indicate that if the price of bDMARD (excluding RTX) were reduced by 50%, the mean ICER would decline to £24,500 for patients with severe RA and £31,500 for patients with moderate to severe RA. Assuming that the efficacy of RTX and TCZ following a previous bDMARD was reduced by reallocating 10% of the patients with a good EULAR response to having no EULAR response increased the mean ICER to £41,600 and £52,100 for patients with severe RA and moderate to severe RA, respectively. Assuming that those with no EULAR response did not cease bDMARD treatment at 6 months but incurred an additional 12 months’ treatment cost increased the mean ICER to £42,200 and £51,400 for patients with severe RA and moderate to severe RA, respectively.
Limitations with this research are that it includes only studies with EULAR endpoints and that the literature search was completed in 2013; however, neither factor is expected to change the conclusions. Analyses contained in Stevenson, et al7 showed that the results were similar to those produced by EULAR data alone when all studies providing ACR data were synthesized and then mapped onto EULAR responses using data from the Veterans Affairs Rheumatoid Arthritis registry. A literature search of relevant clinical papers published since our review identified only 2 with data for the moderate to severe and the severe disease populations44,45 and it is unlikely that these will change the broad conclusion regarding the cost-effectiveness of bDMARD as a group at current market prices. MTX was costed as oral tablets rather than as an injection, which underestimates the cost of this treatment. This is unlikely to markedly affect the ICER because the use of MTX would be similar in both arms. The adopted method for generating utility estimates does not distinguish between reversible and irreversible damage within the HAQ score.
Despite the different modeling approach used within this research, it is noted that the conclusions are similar to those of Joensuu, et al46: that tumor necrosis factor inhibitors do not seem to be cost-effective at a threshold of €35,000 per QALY (US$37,360).
The supplementary analyses undertaken indicated that there may be subsets of patients in whom the use of bDMARD may be cost-effective. Currently there are no agreed algorithms for identifying those patients who will have the worst prognoses while taking NBT. Research regarding prognostic factors in patients with RA could help identify those patients who could be treated cost-effectively with bDMARD.
The estimate of the ICER for a bDMARD strategy in patients with severe and moderate to severe RA suggests that the use of bDMARD has a greater cost per QALY than published NICE thresholds. However, the bDMARD strategies assessed in this research fall within NICE’s thresholds if it is assumed that only those patients with the worst prognoses while taking NBT are treated with bDMARD.
Acknowledgment
The BSRBR is acknowledged for providing access to its data, and for expert advice on how to use it, in particular Rebecca Davies, Xuejuan Fan, Kath Watson, and Kimme Hyrich; and Sam Norton for providing data and expert analyses from the ERAS dataset.
Footnotes
Funding provided by the UK Health Technology Assessment (HTA) Programme of the National Institute for Health Research (NIHR), and the National Institute for Health and Care Excellence. The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, the NIHR Evaluation, Trials and Studies Coordinating Centre, the HTA Programme, or the Department of Health.
- Accepted for publication December 16, 2016.








{kind=link}
{kind=link}
{kind=link}
{kind=link}