

To the Editor:
Calcium pyrophosphate (CPP) deposition in articular tissue causes a spectrum of clinical presentations including asymptomatic chondrocalcinosis, acute CPP crystal arthritis (pseudogout), and chronic CPP inflammatory arthritis1. Known risk factors include older age, osteoarthritis, prior joint injury, metabolic disease, and rarely, family history2. Myelodysplastic syndromes (MDS) are a clinically and genetically heterogeneous group of stem cell disorders generally characterized by hypercellular bone marrow and peripheral cytopenias3. Prognosis depends on comorbidities and disease factors including number of cytopenias, specific chromosomal abnormalities, and degree of marrow blast infiltration [5%–9%, 10%–19%, and ≥ 20% represent refractory anemia with excess blasts (RAEB)-1, RAEB-2, and acute myeloid leukemia (AML), respectively]4.
The patient died before our case report was prepared, and thus we were not able to obtain his written consent to publish the material; however, while he was alive we discussed our plan to prepare this case report and he was in agreement.
Our patient was a 75-year-old man who developed dyspnea in October 2015. Anemia and leukopenia were noted, and bone marrow biopsy revealed hypercellular marrow with 10% blasts consistent with RAEB-2. A very complex/monosomal karyotype including loss of chromosome 17 was noted. In December, he developed left ankle pain and swelling. In January 2016, 3 days after starting decitabine, he developed fever (103°F) and worsened ankle pain. Laboratory results were notable for neutropenia, erythrocyte sedimentation rate 115 mm/h, C-reactive protein 191 mg/l, and uric acid 3.9 mg/dl. Decitabine was stopped and antibiotics were started. Aspiration of the tibiotalar joint yielded turbid fluid [white blood cell count (WBC) 53,060, 97% neutrophils] and few intracellular CPP crystals. Monosodium urate crystals were absent; bacterial, fungal, and mycobacterial synovial fluid cultures were negative. Naproxen was started for acute CPP crystal arthritis, and he was discharged on antibiotics for presumed concurrent septic arthritis.
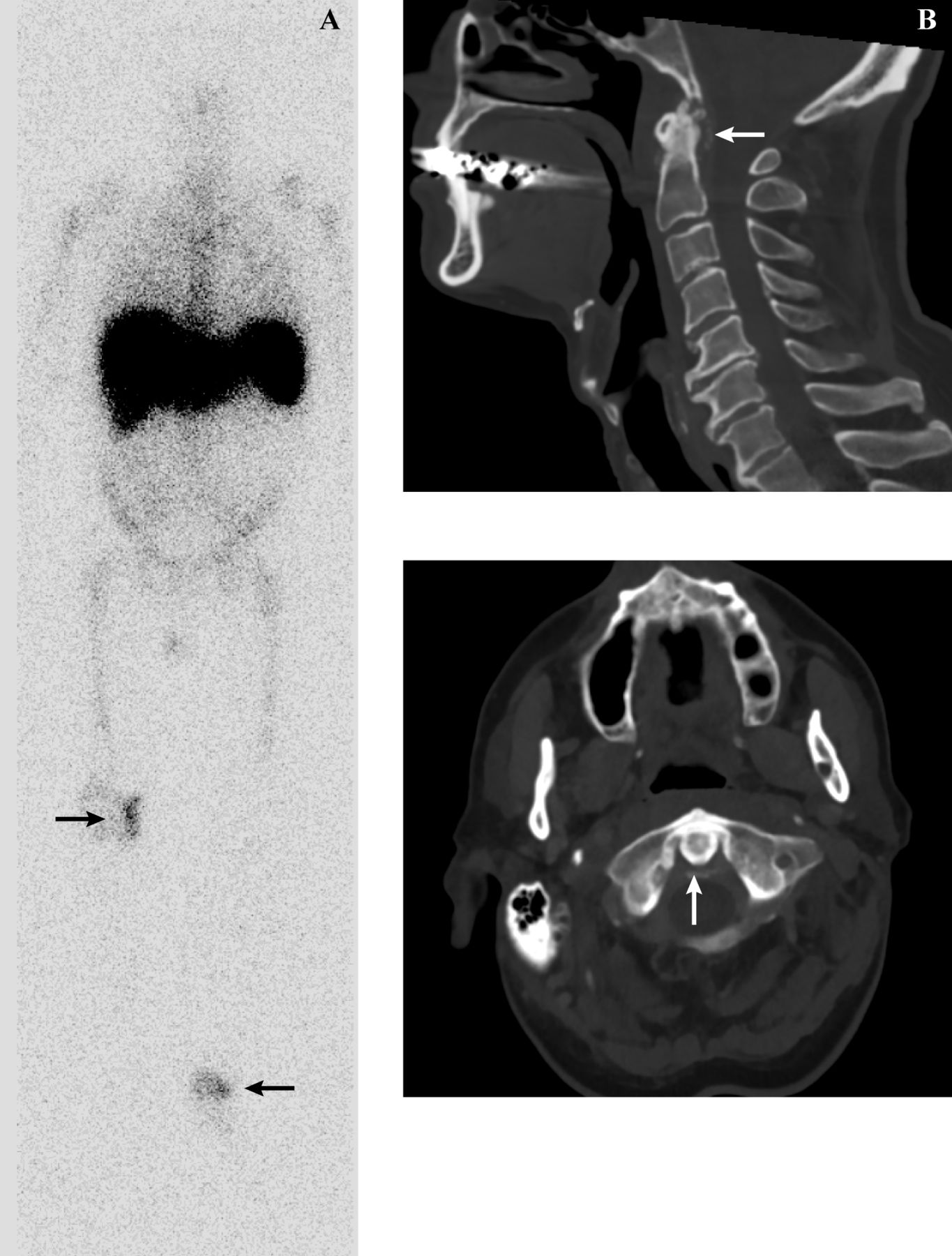
One week later he developed severe neck stiffness, odynophagia, and recurrent, severe left ankle pain/swelling. Temperature was 99.9°F and neurologic examination was normal. Neck range of motion was extremely limited; the left ankle appeared inflamed. Tibiotalar synovial fluid was again inflammatory (WBC 39,500, 93% neutrophils), with intracellular CPP crystals and negative cultures. Computed tomography of the neck showed calcific deposits around the dens in the transverse ligament of the atlas and alar ligaments, consistent with crowned dens syndrome in this context (Figure 1). Tagged WBC scan showed WBC localization in the left ankle and right knee synovial spaces without bony uptake (Figure 1). Two days later the right knee became inflamed. Methylprednisolone 24 mg twice daily was started for crowned dens syndrome and presumed right knee acute CPP crystal arthritis. His neck, ankle, and knee began improving within 1 day. Metabolic workup included normal iron, parathyroid hormone, calcium, alkaline phosphatase, and magnesium. He was discharged on methylprednisolone 16 mg twice daily.
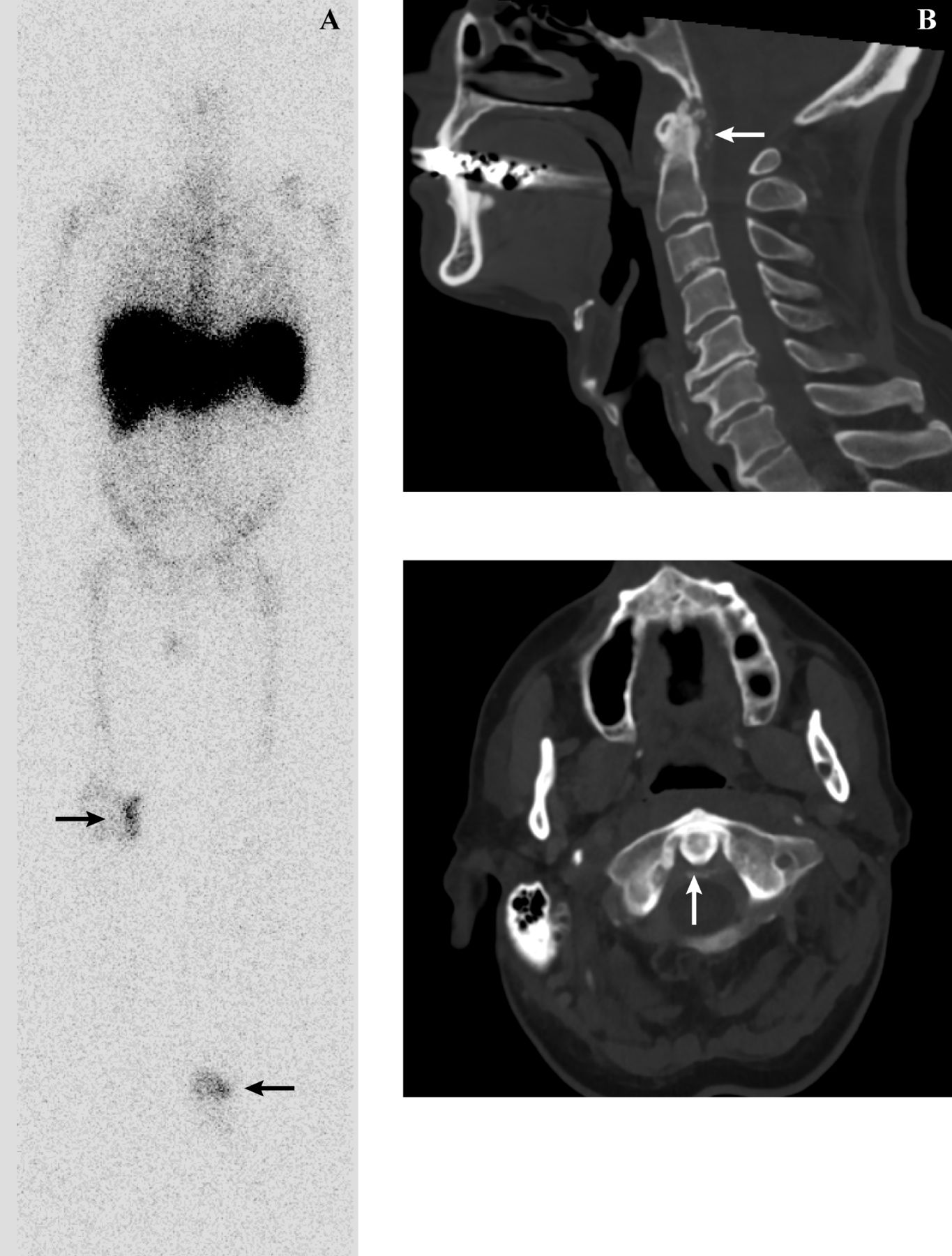
(A) Tagged WBC scan showing WBC (arrows) localized around the right knee (asymptomatic at time of scan) and left ankle (symptomatic at time of scan). (B) Computed tomography scans of the neck performed in the setting of acute neck pain, low-grade fever, and odynophagia. Calcific deposits (arrows) are present around the dens in the transverse ligament of the atlas and alar ligaments. WBC: white blood cell.
One week later, severe left ankle pain/swelling recurred; intraarticular corticosteroid injection provided complete relief. He continued methylprednisolone 16 mg twice daily but the next week, meningismus recurred. Magnetic resonance imaging of the neck confirmed changes consistent with crowned dens syndrome, including pannus formation and edema around the dens. The neck symptoms resolved with increasing methylprednisolone to 20 mg twice daily.
Azacitadine was started for MDS in April. (The patient never received granulocyte-monocyte colony stimulating factor, which has been associated with CPP arthritis5.) Within weeks, nonsteroidal antiinflammatory drugs (NSAID) were contraindicated because of severe thrombocytopenia. Colchicine 0.6 mg every other day was started, but his counts dropped further (WBC 0.7 K/μl, hemoglobin 7.5 g/dl, platelets 12 K/μl); thus colchicine was discontinued. A second bone marrow biopsy revealed no evidence of transformation to AML. Addition of anakinra (interleukin 1 receptor antagonist) was considered, but was not started given the extremely limited data on its use in MDS and concern for triggering AML transformation.
Over the next 2 months, attempts to taper methylprednisolone below 12 mg twice daily resulted in severe neck stiffness/pain or severe right knee swelling/pain. The right knee was aspirated on 3 occasions, each time revealing intracellular CPP crystals and negative cultures. Intraarticular corticosteroid injections provided excellent relief, but lasted only 4 weeks.
A third bone marrow biopsy in July showed stability (5%–10% blasts). Anakinra was offered to the patient for refractory chronic CPP inflammatory arthritis while taking high-dose systemic corticosteroids with contraindications to NSAID, colchicine, and methotrexate2,6. The patient declined anakinra because of concerns about potential side effects. In August, he developed a progressive pneumonia, experienced multiorgan failure, and died.
We propose that our patient’s refractory chronic CPP inflammatory arthritis was a paraneoplastic process secondary to MDS, given near-simultaneous onset of cytopenias and CPP inflammatory arthritis, severe flares occurring on high-dose corticosteroids, and persistent, severe arthritis for 6 months. We were unable to find prior reported cases of paraneoplastic pseudogout or pseudogout related to MDS. New-onset autoimmune or inflammatory conditions, including inflammatory arthritis, occur in up to 25% of patients with MDS7. Inflammatory arthritis in MDS is typically polyarticular, symmetric, and nonerosive8. Treatment is challenging because of cytopenias, increasing the risks of infection and bleeding.
Acute illness, joint trauma, and postoperative state can trigger CPP crystal arthritis2; systemic inflammation from MDS was a potential trigger for our patient. Further investigation into CPP inflammatory arthritis as a paraneoplastic manifestation of MDS is needed.
Acknowledgment
The authors thank Ilene Galinsky, NP, Sarah Hammond, MD, and Varand Ghazikhanian, MD, MS, for their assistance in caring for this patient.
Footnotes
Dr. Tedeschi’s work on this project was supported by the US National Institutes of Health–National Institute of Arthritis and Musculoskeletal and Skin Diseases T32AR007530 and L30AR070514.








{kind=link}