

Abstract
Objective. The autoinflammatory bone disorder chronic nonbacterial osteomyelitis (CNO) covers a wide clinical spectrum, ranging from mild self-limited presentations to chronically active or recurrent courses, which are then referred to as chronic recurrent multifocal osteomyelitis (CRMO). Little is known about treatment options and longterm outcomes. We investigated treatment responses and outcomes in children with CNO.
Methods. A retrospective chart review was conducted in a tertiary referral center, covering 2004–2015. Disease activity was measured at 0, 3, 6, 12, and 24 months after treatment initiation, and at the last recorded visit.
Results. Fifty-six patients with CNO were identified; 44 had multifocal CNO. Fifty percent of patients relapsed after a median of 2.4 years, and as few as 40% remained relapse-free after 5 years. Nonsteroidal antiinflammatory drugs were used as first-line treatment in 55 patients, inducing remission after 3 months in all individuals with relapse rates of 50% after 2 years. Further treatment included corticosteroids (n = 23), tumor necrosis factor-α (TNF-α) inhibitors (n = 7), and bisphosphonates (n = 8). While 47% of patients with CNO relapsed within 1 year after corticosteroid therapy, favorable outcomes were achieved with TNF-α inhibitors or bisphosphonates (pamidronate).
Conclusion. CNO is a chronic disease with favorable outcomes within the first year, but high relapse rates in longterm followup. Particularly, patients with CRMO with long-lasting, uncontrolled inflammation were at risk for the development of arthritis. Our findings underscore the importance of a timely diagnosis and treatment initiation. Prospective studies are warranted to establish evidence-based diagnostic and therapeutic approaches to CNO.
Chronic nonbacterial osteomyelitis (CNO) is an autoinflammatory bone disorder mostly affecting children and adolescents1,2,3,4. The clinical spectrum ranges from mild, self-limiting monofocal to prolonged, multifocal, recurrent courses, which are referred to as chronic recurrent multifocal osteomyelitis (CRMO). Associations with other inflammatory conditions include palmoplantar pustulosis, psoriasis, and inflammatory bowel disease (IBD)4,5,6. Despite recent advances, we are only beginning to understand the pathophysiology of CNO. The expression of immune-regulatory cytokines interleukin (IL)-10 and IL-19 is altered in monocytes from patients with CNO, resulting in increased inflammasome activation and expression of proinflammatory cytokines IL-1β, IL-6, and tumor necrosis factor-α (TNF-α)4,5,7,8,9,10. Imbalanced expression of pro- and anti-inflammatory cytokines may promote inflammatory bone loss11,12,13.
Based on these observations, antiinflammatory treatment and/or osteoclast inhibition appear justified in CNO12. In the absence of placebo-controlled trials, treatment of CNO relies on personal experience, case collections, and expert opinion. Nonsteroidal antiinflammatory drugs (NSAID) are commonly used as first-line therapy. In patients who are refractory to NSAID or in individuals with vertebral lesions, more aggressive treatment is commonly applied, including corticosteroids, sulfasalazine (SSZ), methotrexate (MTX), bisphosphonates, or TNF-α inhibitors2,3.
Longterm outcomes are generally favorable in CNO14,15,16,17. However, a subset of patients presents with vertebral fractures and/or chronically active or remittent disease with ongoing inflammation over years, and long-lasting, insufficiently controlled inflammation appears a risk factor for the development of arthritis18. Previous studies focused on disease outcomes independent of therapeutic regimens and/or used inconsistent evaluation periods that were mostly defined by the last medical visit (from 0.5–15 yrs)6,15,16,17. We investigated disease activity in children with CNO in response to treatment and demonstrate response to NSAID in the first year in a majority of patients, high relapse rates after prednisolone treatment, and long-lasting antiinflammatory effects of TNF-α inhibitors or bisphosphonates.
MATERIALS AND METHODS
Study design and patients
We evaluated treatment responses in CNO at the Department of Pediatrics, University Medical Center Carl Gustav Carus, Dresden, Germany, a tertiary referral center. Fifty-six children were diagnosed with CNO between January 1, 2004, and December 31, 2015 (Table 1). Data were collected by reviewing electronic medical charts. The study was approved by the ethics committee of Technische Universität Dresden (EK 369102014).
Baseline characteristics of children with CNO (n = 56).
In the absence of evaluated diagnostic tools, CNO was defined using the clinical score from Jansson, et al19, additional laboratory findings, bone biopsies, and magnetic resonance imaging (MRI) studies. Defining CNO by a score of ≥ 39 (“probable CNO”), sensitivity in our cohort was 71% and specificity 98%19. Defining CNO by a cutoff value of 29 (“uncertain diagnosis”), sensitivity was 89% and specificity 86%. For the control group, we used the 56 children with bacterial osteomyelitis published in Schnabel, et al’s study18.
Outcome assessment
The following datasets were collected: (1) clinical characteristics, including sex, age, local inflammatory signs, loss of function, fever (> 38.0°C/100.4°F), number of painful sites, relapses, sequelae (hyperostosis, vertebral fractures, compression of blood vessels, or nerve involvement), extraosseous manifestation, and time of followup; (2) diagnostic tools: complete blood cell count (CBC), C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), liver enzymes, lactate dehydrogenase, alkaline phosphatase, calcium, phosphate, ferritin, immunoglobulins, HLA-B27 status, microbiological cultures, bone biopsies, and findings on imaging (particularly MRI) at presentation and during followup; and (3) treatment: antibiotics, NSAID (ibuprofen, naproxen), corticosteroids, disease-modifying antirheumatic drugs (DMARD; MTX, SSZ), bisphosphonates (pamidronate), or TNF-α inhibitors [etanercept (ETN), adalimumab (ADA)]. Clinical outcomes were assessed at 0, 3, 6, 12, and 24 months after treatment initiation, and at the last visit.
Patients exclusively treated with NSAID were summarized in the NSAID treatment group. In the corticosteroid, bisphosphonate, and TNF-α inhibitor groups, concomitant use of NSAID was tolerated. Because we followed a “step-up strategy,” starting with NSAID and escalating treatment as needed, an individual patient may be included in the subgroup analysis a maximum of 4 times (e.g., NSAID failure and anti-TNF responder). Patients with spinal involvement were treated more aggressively. However, all patients with CNO with vertebral involvement concomitantly received NSAID. DMARD were applied in 2 patients, prednisolone in 7, TNF-α inhibitors in 6, and bisphosphonates in 6 (5/6 at diagnosis secondary to vertebral fractures).
Because no standardized outcome measures are available for CNO, we monitored clinical symptoms (pain, signs of inflammation) and objective measures (blood inflammation markers and number of lesions on imaging). MRI included (1) regional scans using native T1, contrast-enhanced T1 with fat saturation, and turbo-inversion-recovery-magnitude (TIRM) sequences, and (2) coronal whole-body MRI applying TIRM sequences. MRI scans were read by a pediatric radiologist experienced in bone imaging and inflammatory conditions (GH). Partial clinical remission was defined as overall subjective improvement and reduction of inflammatory variables, and full clinical remission by the absence of subjective and objective signs of inflammation. Relapse was defined as new onset of clinical symptoms and new lesions visible on MRI after temporary remission. Inefficacy was defined by the absence of improvement or disease progression resulting in treatment escalation.
Statistical analysis
Statistical analysis was performed using SPSS 21.0 software (SPSS Inc.). Kolmogorov-Smirnov tests were applied to test normal distribution of data. Categorical variables were reported as numbers (percent) and continuous variables as means ± SD or median with ranges, depending on the presence of normal distribution. Kaplan-Meier survival curves indicate the probability of relapse-free survival and the median time to relapse (period from diagnosis to first relapse). Differences between groups were defined as statistically significant by 2-sided p values < 0.05.
RESULTS
Clinical characteristics
Fifty-six children were diagnosed with CNO in our institution between 2004 and 2015. Patients’ characteristics are summarized in Table 1, some of which (49 patients) were included in a recent comparative analysis of CNO versus bacterial osteomyelitis18. Median age at disease onset was 11.1 years (Table 1), with a slight female predominance (1.4:1). Twenty-one children with CNO reported multifocal bone pain at disease onset, most commonly affecting lower extremities (41/56, 73%). A total of 26 patients (46%) presented CNO-related extraosseous symptoms, including arthritis (n = 20/56, 36%), IBD (n = 6/56, 11%), acne fulminans (n = 5/56, 9%), and palmoplantar pustulosis (n = 5/56, 9%). Seven children (13%) developed arthritis distant from CNO lesions a median of 4.9 years after disease onset (range 2.2–6.8 yrs), involving sacroiliac joints (n = 3), temporomandibular joints (n = 3), knees (n = 3), ankles (n = 2), hip (n = 1), and atlanto-occipital/-axial joints (n = 1). Patients affected by arthritis were characterized by delayed diagnosis (median 6.5 mos, range 3–60), relapsing multifocal courses (CRMO, mean 13 ± 4 lesions), persistently active disease, and prolonged treatment (median 5.9 yrs, range 2.3–7.3). Two patients with CNO, whose families rejected antiinflammatory treatment, developed spondyloarthropathy after 6 years. One was a 14-year-old boy (HLA-B27–positive) with enthesitis-associated juvenile idiopathic arthritis. A 9-year-old girl (HLA-B27–negative) developed sacroiliitis, arthritis of the atlanto-axial and atlanto-occipital joints, and IBD (Crohn disease). HLA-B27 was positive in 9/43 tested patients (21%), 5 of whom developed arthritis.
Additional sequelae included spinal involvement in 25% (n = 14/56) with pathological vertebral fractures in 11% (n = 6/56), hyperostosis in 29% (n = 16/56; 4 with persistent mandibular swelling), compression of subclavian vein (n = 1/56), and femoral nerve involvement by paraosseous inflammation (n = 1/56).
Pathological findings and patient stratification
In analogy to the historic classification of bacterial osteomyelitis, we stratified distinct clinical presentations in our CNO cohort: (1) subacute presentations with symptoms of 2 weeks to 3 months (n = 12), (2) chronic presentations with symptoms of 3 months or longer (n = 40), and (3) relapsing, multifocal courses (CRMO; n = 29). In 4 patients, a definite classification to 1 distinct CNO subgroup was not possible.
At diagnosis, CBC was normal in 71% (n = 40/56), while 29% (n = 16/56) of patients with CNO had thrombocytosis. Monocytosis (7%–12%, normal range 1%–6%) was seen in 75% of the patients (8.1 ± 2.1%); CRP (16.9 ± 43 mg/l) and/or ESR (31.7 ± 24.4 mm/h) were elevated in 52% (n = 29/56). The level of inflammatory markers (leukocytosis, CRP, ESR) did not correlate with clinical signs of inflammation, fever, or the number of osseous lesions on MRI. Clinical chemistry, including lactate dehydrogenase, liver enzymes, alkaline phosphatase, calcium, phosphate, immunoglobulin G (IgG), IgA, and IgM, was not significantly altered. Bone biopsies were available in 34/56 patients with CNO (61%), predominantly showing chronic inflammation with lymphoplasmocytoid infiltrates in 27 patients with CNO (79%).
Coronal whole-body MRI studies (TIRM) were available in 42 patients, and regional MRI (native T1, contrast-enhanced T1 with fat saturation, and TIRM sequences) of the most affected area in 13/56 patients with CNO. Forty-four children (79%) developed multifocal bone involvement during followup, while only 12 patients (21%) exhibited monofocal disease. A total of 385 bone lesions were detected, the majority of which were located in the lower extremities (216, 56%). Of the 14 children presenting with vertebral involvement at time of diagnosis, 4 patients exhibited active lesions on MRI (including contrast enhancement in T1 sequences with fat saturation on regional scans, or hyper-intense lesions in TIRM sequences in regional or coronal whole-body MRI) 1 year after diagnosis.
Disease course and treatment response
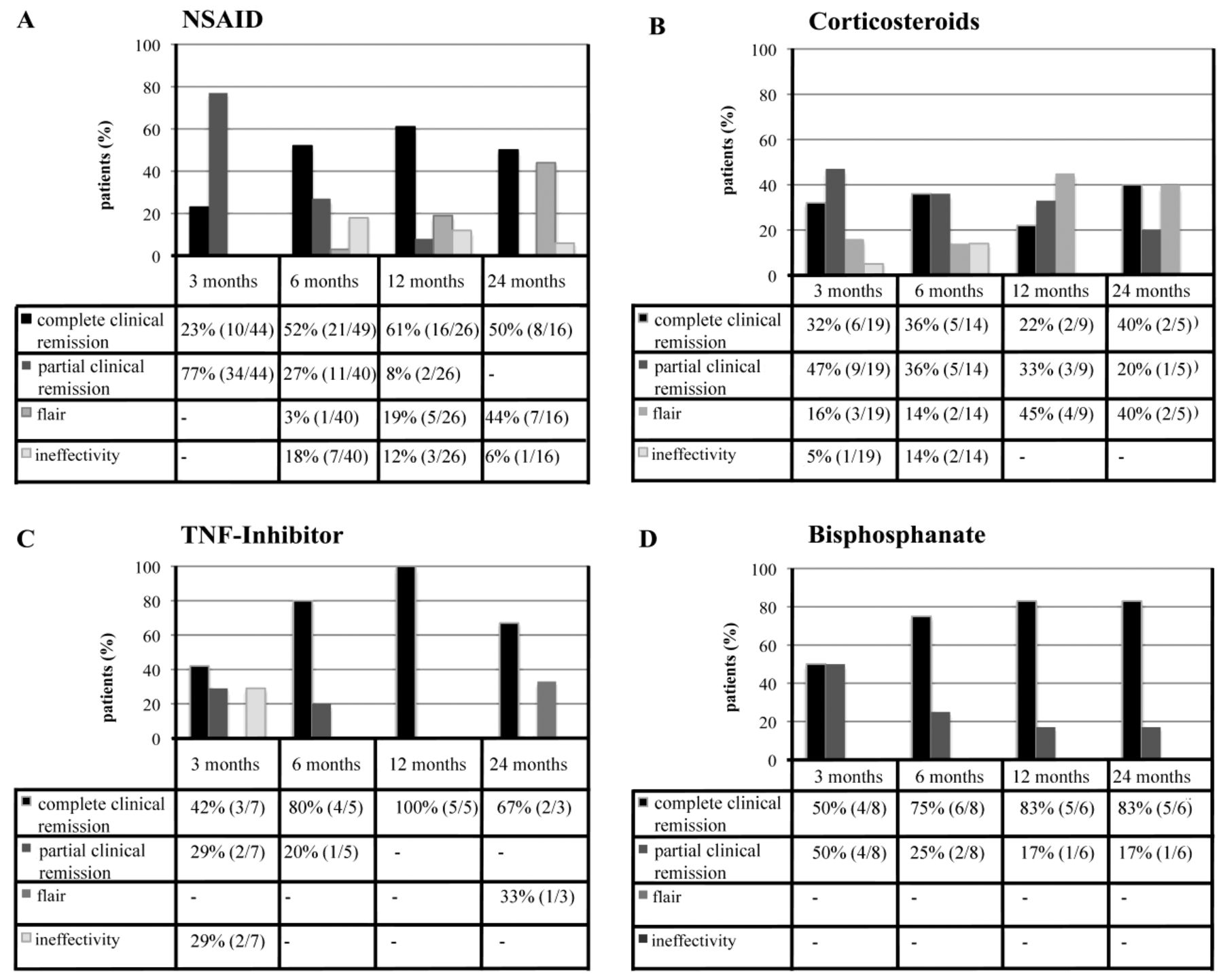
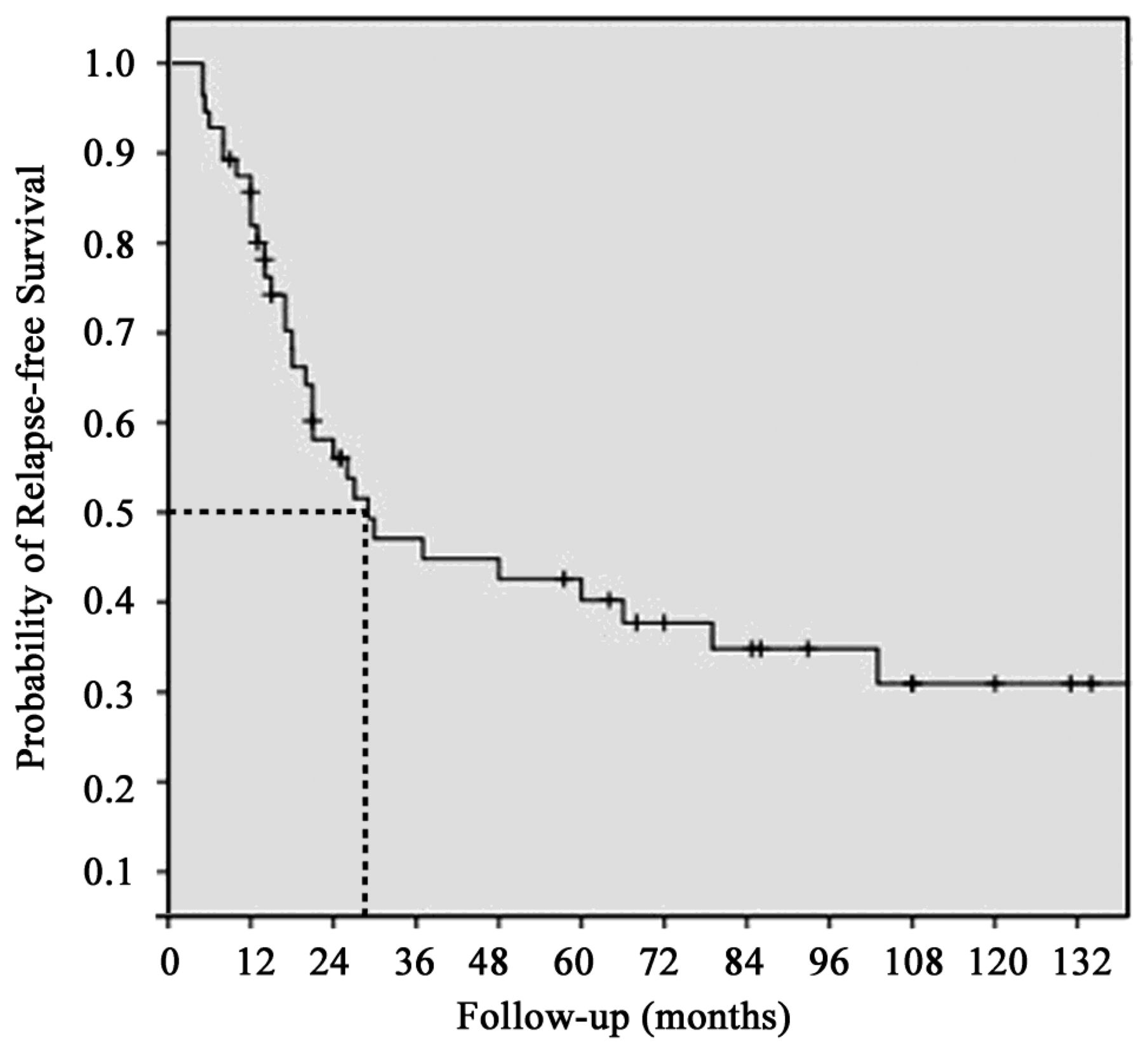
Except for 1 individual with concomitant Crohn disease, all patients with CNO initially received NSAID. Twenty-three patients were treated with prednisolone, 6 with DMARD (2 MTX, 4 SSZ), 7 with TNF-α inhibitors (6 ETN, 1 ADA), and 8 with bisphosphonates (pamidronate). Treatment responses of 56 patients with CNO are provided in Figure 1. Patients with CNO were followed for a median of 2.4 years (range 0.3–9 yrs); of them, 21 were followed for more than 5 years. During followup, 33 patients developed a median of 1 relapse (range 1–6). As determined in the Kaplan-Meier survival analysis, median time from diagnosis to first relapse was 29 months (range 5–103 mos; Figure 2). Most patients with CNO showed favorable courses within the first year with clinical remission in 62% (n = 35/56) and relapse-free survival in 85%, independent of therapy. However, after 5 years, 60% had experienced a minimum of 1 relapse (Figure 2).

Clinical outcome after therapy with (A) NSAID, (B) steroids, (C) TNF-α inhibitor, and (D) bisphosphonates over a followup period of 3 to 24 months. NSAID: nonsteroidal antiinflammatory drugs; TNF-α: tumor necrosis factor-α.

Probability of relapse-free survival in children with CNO, as determined by Kaplan-Meier analysis. Fifty-six children with CNO have been included, from which 33 children had a minimum of 1 relapse during followup. The dotted line indicates the median time from diagnosis to the first relapse (29 mos). CNO: chronic nonbacterial osteomyelitis.
Antibiotics
Twenty patients with CNO (36%) were initially treated with antibiotics for suspected bacterial osteomyelitis. However, the number of patients who received antibiotics in CNO significantly declined over time (1998–2007: 70% and 2008–2015: 18%, p = 0.001). Median duration of intravenous antibiotic therapy was 2 weeks (range 0–5), followed by oral therapy of 12 weeks (range 3–248 weeks). The patient with 248 weeks of antibiotic therapy was treated for suspected skeletal tuberculosis in external institutions. Exclusive antibiotic treatment failed to be effective in all patients with CNO. After 6 months of antibiotic treatment, 12 patients were characterized as nonresponders and were diagnosed with CNO. Eight patients with CNO treated with antibiotics reached partial remission. However, all of 8 patients with CNO and antibiotic treatment received additional NSAID.
NSAID
Generally, NSAID (naproxen 10–15 mg/kg/day, or ibuprofen 30 mg/kg/day) were applied as first-line treatment for a median of 13 months (range 3–90). Forty-four of the 55 patients initially treated with NSAID did not receive concomitant antiinflammatory therapy. NSAID were beneficial in all patients, resulting in either partial (34/44, 77%) or complete remission (10/44, 23%) after 3 months (Figure 1). However, after 1 year 31% and after 2 years 50% of patients exhibited CNO-related symptoms or had relapsed (Figure 1). Patients unresponsive to NSAID treatment were characterized by a high proportion of jaw, clavicular, and vertebral involvement.
Whole-body MRI within the first year of NSAID treatment were available in 27 patients. In children with clinical remission, 18% exhibited new lesions (5/27), 56% had remaining activity (15/27), and 26% had complete “radiological remission” (7/27). Of note, none of the 5 patients who presented new lesions experienced clinical symptoms, and treatment was not escalated (because vertebral bodies were not affected).
Corticosteroids
In patients who failed to respond to NSAID, treatment was escalated, usually with oral prednisolone (2 mg/kg/day for 5–10 days, maximum 60 mg/day). All patients experienced clinical improvement after 2 weeks. However, 21% clinically relapsed or deteriorated after 3 months, and 45% after 1 year. After prednisolone therapy, MRI scans were available in 12 patients and presented no visible lesions in 3 patients (25%), remaining activity in 7 (58%), and new lesions in 2 (17%).
DMARD
Six children receiving DMARD were excluded from analyses: 4 were treated for accompanying arthritis and/or IBD, 1 was treated with SSZ and responded incompletely after 12 months, and 1 discontinued therapy after developing allergic exanthema.
TNF-α inhibitors
Patients who failed to improve under corticosteroid therapy were introduced to TNF-α inhibitors or bisphosphonates. All 7 patients who received TNF-α inhibitors were diagnosed with chronically active disease (CRMO with vertebral involvement in 5, associated arthritis in 4) and exhibited long-lasting disease activity prior to anti-TNF-α treatment (median 48 mos, range 1–65 mos). In all the children treated with TNF-α inhibitors, MRI were available within the first year. Anti-TNF therapy was effective in 5 patients. After 3 months, 2 patients reached partial and 3 patients reached complete remission. In all 5 patients, clinical remission remained stable after 12 months: 4/5 were free of visible lesions on MRI and 1/5 showed minimal activity. Anti-TNF treatment was ineffective in 2 patients, who failed to respond clinically and exhibited new lesions on MRI. Both individuals had developed side effects and discontinued treatment after 3 months (abdominal pain and reduced general condition). To some extent it remains unclear whether these patients reliably applied treatment before discontinuation.
Bisphosphonates
In our cohort, most favorable outcomes were achieved in patients who received pamidronate (Day 1: 0.5 mg/kg, days 2 and 3: 1 mg/kg, repeat after 3 and 6 mos with 1 mg/kg for 3 days; n = 8). During the first cycle, 6 patients developed mild side effects, including fever (n = 4), conjunctivitis (n = 2), and mild hypocalcemia (n = 1). After 6 months, 2/8 individuals reached partial and 6/8 complete remission. Followup data at 24 months were available for 6 patients; 5/6 had reached full and 1/6 had reached partial remission (Figure 1). Patients who received pamidronate were characterized by male sex (6/8, 71%), chronic multifocal disease (7/8, 86%), vertebral involvement with fractures (5/8, 63%), and long-lasting disease activity (median 48 mos). According to imaging techniques, best outcomes were seen in the bisphosphonates group. None of these children exhibited new lesions on MRI after 3 or 4 pamidronate cycles. Four symptom-free children (50%) showed no active lesions and 4 patients exhibited mild remaining activity on MRI.
DISCUSSION
In the absence of randomized placebo-controlled trials, retrospective evaluation of clinical courses is the only available approach to understand treatment responses in CNO. We assessed disease outcomes in response to treatment over a period of 2 years and at the end of followup. The reported cohort underwent standardized diagnostic and therapeutic procedures in a specialized tertiary referral center, largely eliminating a major limitation of retrospective studies. As discussed in previous reports, analysis was complicated by recurrent courses with phases of disease activity and inactivity, which may (in individual cases) be misinterpreted as therapeutic success4,10.
In agreement with other reports, the majority of patients presented with the severe phenotype CRMO and relapsed after a median of 29 months6,14. Of note, most previous reports evaluated disease outcomes at the last medical visit, which ranged between 0.5–15 years after diagnosis, resulting in variable remission rates6,15,16,17. While only 14% of patients with CNO in this cohort exhibited relapses within 1 year, as many as 60% were clinically active after 5 years. We conclude that longterm outcomes in children with CRMO may be less favorable than previously proposed15,16,17,20 with ongoing disease activity and disease-related sequelae in 34%, particularly in children with long-lasting, uncontrolled inflammation18 because of (1) delayed diagnosis, (2) insufficient treatment response, or (3) insufficient adherence, which increases the risk for arthritis. In agreement with other studies, CNO may evolve into spondyloarthropathy, which is supported by HLA-B27 positivity in 21% of the patients as compared with 8% in the general population15,21,22. Borzutzky, et al reported comparable rates of arthritis in a cohort of 70 patients with CNO (36% vs Borzutzky, et al’s 39%)23. Thus, our findings underscore the importance of a timely and correct diagnosis, followed by effective antiinflammatory treatment for the prevention of longterm sequelae.
NSAID (ibuprofen and naproxen) are commonly used as first-line therapy in CNO without vertebral involvement and/or structural damage3,14,16. Indomethacin and meloxicam are not approved for children in Germany and therefore were not prescribed. Antiinflammatory effects of NSAID are achieved through cyclooxygenase inhibition and subsequently reduced prostaglandin production24. Further, variable effects of NSAID on the activity of inflammasomes have been reported25. Proinflammatory monocytes are centrally involved in the pathophysiology of CRMO, potentially contributing to osteoclast differentiation and activation2,8. Because prostaglandins are key mediators during osteoclast activation, and proinflammatory monocytes in CRMO are characterized by increased inflammasome activation7, the inhibition of cyclooxygenase and inflammasome activity appears to be a promising intervention in CNO2,3,4,8,12,26. Indeed, all patients with CNO treated with NSAID improved after 3 months. However, only 50% maintained stable clinical remission without further treatment at later timepoints. These observations agree with data from Kaiser, et al (57%)17. Of note, patients with CNO in Kaiser, et al’s cohort exhibited comparable clinical (61% vs 51%) and “radiological remission” rates (26% vs 27%) after 12 months, when compared with the data of Beck, et al14.
In patients who did not reach remission under NSAID, treatment was escalated with corticosteroids. Like NSAID, corticosteroids reduce prostaglandin synthesis through the inhibition of phospholipase A227,28. Further, corticosteroids inhibit nuclear factor-κB–mediated expression of proinflammatory cytokines (IL-1, IL-6, and TNF-α), which are overexpressed in monocytes from patients with CRMO2,29. Corticosteroids induced short-term improvement in most patients (79%), two-thirds of whom relapsed or progressed within 12 months. Thus, we conclude that repeated oral courses are not beneficial. Corticosteroids may rather be used as bridging therapy during the establishment of DMARD treatment. To our knowledge, other studies did not investigate effects of corticosteroid effects alone, but did explore their potential as bridging agents until second-line DMARD reach effectiveness14,23.
Imbalanced expression of pro- and antiinflammatory cytokines is a hallmark of CNO3,8,26. Because TNF-α is a central contributor to systemic inflammation, activating various immune cells, TNF-α inhibitors appear to be a reasonable therapeutic option2,3,30,31,32,33,34. Several small case series document the induction of clinical and “radiological remission” to TNF-α inhibition in patients who are refractory to other therapy17,23,30,32,33. Here, 7 patients with CNO were treated with TNF-α inhibitors, all of whom were diagnosed with CRMO and had failed to respond to NSAID and/or corticosteroids. Further, patients with concomitant arthritis benefit from anti-TNF-α therapy. Seventy-one percent responded to TNF-α inhibitors after 3 months (Figure 1) and maintained remission after 12 months. Because of a lack of consistent treatment protocols, defined followup measures, and periods throughout the literature, treatment responses from previous studies are hardly comparable with our findings. Owing to the off-label character and high cost, biological therapy should be considered for severe CRMO refractory to other treatment32.
Here, the most promising longterm outcomes were achieved with pamidronate. Bisphosphonates were claimed to exert disease-modifying effects in patients with CNO through the inhibition of osteoclast-mediated bone resorption and the suppression of proinflammatory cytokines7,8,26,35. In concordance with previous reports, all patients treated with pamidronate reached clinical remission after 6 months, and remained stable after 2 years5,35,36,37. Patients treated with pamidronate were characterized by long-lasting disease activity, failure to respond to other medication, multifocal bone lesions, and/or spinal involvement. Though bisphosphonates are highly effective in controlling pain, remaining bone inflammation was detectable on MRI in 43% after 1 year, which agrees with previous reports36. Provided potential side effects, including growth retardation and the fact that bisphosphonates remain in the bone for years, bisphosphonates should be considered only in cases refractory to other treatment or in patients with primary vertebral involvement and structural damage38.
Future therapeutic approaches may target the imbalance between pro- and antiinflammatory cytokine expression. This may be achieved through (1) restoring molecular defects39, (2) blocking proinflammatory cytokines5,30,32, or (3) substituting antiinflammatory proteins40,41,42. Currently, restoring molecular defects is impossible, because the exact molecular defects resulting in CNO are incompletely understood. For blocking proinflammatory cytokines, studies unveiled increased IL-1β activation through inflammasomes in CRMO monocytes as compared with healthy controls7. Thus, blocking IL-1β may be a promising option in a subset of treatment-resistant patients with CRMO. In fact, patients with familial CNO (Majeed syndrome) and individual patients with sporadic CNO have been reported to respond to treatment with recombinant IL-1 receptor antagonist anakinra32,43,44. Provided that in addition to TNF-α, IL-6 is also increased in sera from patients with CRMO and that IL-1β increases not only TNF-α but also IL-6, blocking IL-6 or its receptors may be beneficial26. Finally, insufficiently expressed IL-10 could be delivered to monocytes to restore cytokine imbalance in CNO. However, systemic approaches hold the risk of side effects and targeted cell-specific applications, such as nanolipogels45, and are not established in the human system yet. Thus, future therapeutic approaches remain subject to speculation.
Standardized diagnostic and therapeutic approaches in our institution allowed a comprehensive retrospective analysis of treatment responses and longterm outcomes in patients with CNO. In most cases, CNO follows chronically active or remitting courses that require sufficient treatment. In individuals who are refractory to NSAID and/or corticosteroids, TNF-α inhibitors or bisphosphonates are safe and effective alternatives. Currently, consensus treatment plans and patient registries are about to start collecting prospective data on clinical, radiological, and serological (serum biomarkers) treatment responses. Randomized clinical trials comparing treatment effects of currently applied regimens are warranted to guarantee individually tailored, effective, and safe treatment options for patients with CNO.
Acknowledgment
We thank Professor G. Fitze (Pediatric Surgery), Professor G. Lauer (Oral and Maxillofacial Surgery), and Dr. F. Thielemann (Orthopedic Surgery), and the Pediatric Rheumatology and Immunology Section, Universtitätsklinikum Carl Gustav Carus, Technische Universität Dresden, Dresden, Germany.
- Accepted for publication March 14, 2017.








{kind=link}
{kind=link}