

Abstract
Objective. To compare the clinical characteristics and identify the longterm outcomes of Chinese patients with different antisynthetase antibodies.
Methods. We investigated retrospectively 124 consecutive patients with antisynthetase syndrome. Medical records, laboratory results, and computed tomography images were obtained.
Results. The antisynthetase antibodies we investigated were anti-Jo1 (n = 62), anti-PL7 (n = 31), anti-PL12 (n = 12), and anti-EJ (n = 19). The overall prevalence of interstitial lung disease (ILD) reached 94.4% among study patients. Eleven patients (8.9%) developed rapidly progressive ILD (RP-ILD). Eight patients (6.5%) experienced malignancy. RP-ILD was statistically more prevalent in patients with antisynthetase syndrome with anti-PL7 than those without anti-PL7 (p = 0.028). Anti-Ro52–positive patients with antisynthetase syndrome experienced higher frequency of RP-ILD than those without anti-Ro52 (p = 0.001). Further, anti-PL7–positive patients coexisting with anti-Ro52 exhibited more RP-ILD than those without anti-Ro52 (p = 0.001). Patients with antisynthetase syndrome with RP-ILD had a higher proportion of neutrophils in bronchoalveolar lavage fluid and serum ferritin than those without RP-ILD (p = 0.006 and p = 0.013, respectively). Although no differences were observed between the Kaplan-Meier curves of the 4 antisynthetase antibodies subgroups (p = 0.349), the survival rate of patients with anti-PL7 decreased more rapidly in the early stage of longterm followup compared with those with other antisynthetase antibodies. The presence of RP-ILD, malignancy, and elevated serum ferritin was identified to be associated with poor prognosis in patients with antisynthetase syndrome.
Conclusion. Our study investigates the clinical phenotypes and outcomes of patients with antisynthetase syndrome with distinct antisynthetase antibodies and highlights the link between the anti-PL7 antibody and RP-ILD.
- ANTI-tRNA SYNTHETASE ANTIBODY
- ANTI-Ro52 ANTIBODY
- RAPIDLY PROGRESSIVE INTERSTITIAL LUNG DISEASE
- PROGNOSTIC FACTORS
Antisynthetase syndrome is characterized by the presence of antiaminoacyl-RNA synthetase antibodies, inflammatory myositis, interstitial lung disease (ILD), arthritis, fever, mechanic’s hands, and Raynaud phenomenon (RP). As a hallmark of antisynthetase syndrome, antisynthetase antibodies occur in 15% to 30% of patients with myositis1,2. Anti-Jo1 (anti-histidyl) occurs most frequently in 60%–80% of patients with antisynthetase syndrome. Less frequent antisynthetase antibodies are now routinely detected in clinical practice, being reported in about 5% of patients with antisynthetase syndrome2,3,4, such as anti-PL7 (antianalyl), anti-PL12 (antithreonyl), anti-EJ (antiglycyl), and anti-OJ (anti-isoleucyl). Some antisynthetase antibodies rarely found in patients with myositis are anti-KS (antiasparaginyl), anti-Zo (antiphenylalanyl), anti-SC (antilysyl), anti-JS (antiglutaminyl), and anti-YRS (antityrosyl). Although patients with antisynthetase antibodies share many common clinical features, several investigators have reported on the heterogeneity of antisynthetase syndrome5,6,7.
Antisynthetase syndrome is also an overlapping myositis, often presenting with Sjögren symptoms. The autoantibodies of Sjögren symptoms, including anti-Ro60/52kDa and anti-La/SSB, were commonly observed in antisynthetase syndrome. Anti-Ro52 autoantibody can be detected in 59% of patients with antisynthetase syndrome in a previous report8. Moreover, anti-Ro52 has been shown to participate in the pathogenesis of myositis9 and associated closely with pulmonary manifestations10. Previous studies also observed that the presence of anti-Ro52 causes more severe ILD in anti-Jo1–positive patients11,12,13,14.
We conducted this study to determine the differences between the clinical manifestations and the longterm outcomes of Chinese patients with distinct antisynthetase antibodies.
MATERIALS AND METHODS
Patients
Our study involved patients with antisynthetase syndrome referred to the Rheumatology Department of the China-Japan Friendship Hospital from January 1994 to September 2016. All patients’ data were used anonymously. This study was approved by the Research Review Committee and the Ethical Review Committee of the China-Japan Friendship Hospital (approval number 2013-6).
Data collection
Clinical data and laboratory results were obtained retrospectively from medical records. The data obtained were age of onset, sex, duration, presence or absence of muscle weakness, myalgia, dysphagia, ILD, rapidly progressive ILD (RP-ILD), mechanic’s hands, RP, Gottron papules, heliotrope rash, arthritis/arthralgia, malignancy, and pericarditis. Laboratory test results were recorded. Survival status was confirmed by telephone or hospital records.
Definition
Idiopathic inflammatory myopathy (IIM) was defined by a clinical presentation with skeletal muscle weakness, elevated serum levels of muscle enzymes, and electromyography together with characteristic histopathological changes on muscle biopsy15. Diagnosis of antisynthetase syndrome was based on criteria proposed by Solomon, et al16. The presence of ILD was evaluated by computed tomography (CT) and abnormal pulmonary function test17. CT scan patterns were classified as usual interstitial pneumonia (UIP), nonspecific interstitial pneumonia (NSIP), and organizing pneumonia (OP) by 2 experienced radiologists. RP-ILD was defined as a worsening of radiologic interstitial changes with progressive dyspnea and hypoxemia within 3 months after the onset of respiratory symptoms18. Pericardial effusion was assessed by CT and/or echocardiography examination.
Antisynthetase antibodies analysis
The antisynthetase antibodies were identified using EUROIMMUN immunoblot according to the manufacturer’s instructions, including the anti-Jo1, anti-PL7, anti-PL12, anti-EJ, and anti-OJ antibodies. The results were considered positive if the bands showed moderate or strong reaction.
Statistical analysis
Statistical analysis was performed using SPSS software version 21.0. Chi-square and Fisher’s exact tests were used to compare the frequencies of the antisynthetase antibodies subgroups. Comparisons involving continuous variables among groups were performed using ANOVA. Pairwise comparisons were carried out if the overall p value was < 0.05. Survival curves were drawn using the Kaplan-Meier method. The log-rank test was used to compare survival rates. Cox proportional hazards regression analysis was used to assess prognostic factors. Results were regarded as significant when p values were < 0.05.
RESULTS
Prevalence of antisynthetase antibodies
Of 639 patients with IIM, 124 antisynthetase antibodies–positive patients (19.4%) were identified. Among the 124 patients with antisynthetase syndrome, 62 patients (50.0%) were anti-Jo1–positive, 31 (25.0%) were anti-PL7–positive, 12 (9.7%) were anti-PL12–positive, and 19 (15.3%) were anti-EJ–positive. Interestingly, we found anti-SRP and anti-MDA5 antibodies in 2 patients with antisynthetase syndrome with anti-Jo1. To avoid the bias resulting from other myositis-specific antibodies, we excluded those 2 patients.
Demographic features
The general clinical characteristics and comparisons between the 4 groups are shown in Table 1. The mean followup time was 47.6 ± 45.9 months. The mean age at onset was 50.4 ± 11.8 years. The majority of patients were women (M:F = 15:47). The mean duration of disease was 12.9 ± 31.2 months. No differences were observed between the demographic features of the 4 groups.
Comparisons of clinical characteristics in antisynthetase antibody–positive patients with idiopathic inflammatory myopathy. Pairwise comparisons were further analyzed when overall p value was < 0.05. Data are presented as n (%) or mean ± SD.
Comparisons of clinical characteristics
As the most common manifestation of antisynthetase syndrome, the frequency of ILD reached 94.4% in our cohort. Among the patients with ILD, 11 (8.9%) were identified with RP-ILD. Muscle weakness was present in 63.7% of patients, followed by arthritis/arthralgia in 54.0%, mechanic’s hands in 46.0%, Gottron papules in 44.4%, myalgia in 36.3%, heliotrope rash in 21.8%, dysphagia in 11.3%, pericarditis in 10.5%, and RP in 9.7%. There were statistical differences in the frequencies of heliotrope rash and arthritis/arthralgia among the 4 subgroups (overall p = 0.001 for both characteristics). Patients with anti-PL7 had a higher frequency of heliotrope rash than those with anti-Jo1 or anti-EJ (p < 0.001 and p = 0.02, respectively). Arthritis/arthralgia was more frequently observed in patients with anti-Jo1 than those with anti-PL7 and anti-EJ (p = 0.007 and p = 0.001, respectively).
Notably, 6 of the 31 patients with anti-PL7 developed RP-ILD, but there was no significant difference between the 4 groups in frequency of RP-ILD (overall p = 0.127). However, RP-ILD was statistically more prevalent in patients with antisynthetase syndrome with anti-PL7 than those without anti-PL7 (p = 0.028). The frequencies of the other clinical characteristics varied among the subgroups, but no significant differences were observed.
Complications of malignancy
During the followup period, 8 patients (6.5%) developed malignancies. The malignancies involved the breast (n = 3), stomach (n = 1), cervix (n = 1), nasopharynx (n = 1), salivary duct (n = 1), and thyroid (n = 1) of the patients.
Three patients suffered from malignancy within 3 years prior to IIM diagnosis and 1 patient experienced malignancy within 3 years after IIM diagnosis. The interval time of malignancy and IIM was more than 3 years in the remaining 4 patients. Seven of 8 patients also experienced ILD. The patient with salivary duct carcinoma suffered from RP-ILD.
Prevalence of myositis-associated antibodies
Antinuclear antibodies (ANA), anti-Ro60, anti-Ro52, and anti-RNP antibodies were found in 55.6%, 30.6%, 29.0%, and 4.0% of patients with antisynthetase syndrome, respectively. Differences were observed in the occurrence of ANA and anti-Ro52 among the subgroups (overall p = 0.001 and p < 0.000, respectively). Intragroup comparisons showed that patients with anti-Jo1 were less likely to have ANA and anti-Ro52 antibodies than patients with anti-PL7, anti-PL12, and anti-EJ (all p < 0.05). Of note, RP-ILD was more frequently observed in patients with antisynthetase syndrome with anti-Ro52 than those without anti-Ro52 (p = 0.001). Further, anti-PL7–positive patients with anti-Ro52 experienced more RP-ILD than those without anti-Ro52 (p = 0.001). But there was no significant difference in RP-ILD occurrence related to the presence or absence of anti-Jo1, anti-PL7, and anti-EJ. No difference was found in the prevalence of malignancy in patients with antisynthetase syndrome with anti-Ro52 compared with those without anti-Ro52 (p = 0.436).
Laboratory results
No differences were found in the serum ferritin, creatine kinase, C-reactive protein, and lymphocyte subset levels among the subgroups, but the overall mean serum ferritin level was higher than normal (11–306.8 ng/ml). The increase in the lymphocyte subset 1 (B1) and B2 cells was observed in all subgroups.
Comparisons of ILD features between antisynthetase antibodies subgroups
The median values of DLCO of patients with anti-Jo1, anti-PL7, anti-PL12, and anti-EJ were 55.5%, 53.7%, 42.5%, and 52.5%, respectively. Median values of forced vital capacity (FVC) of patients with anti-Jo1, anti-PL7, anti-PL12, and anti-EJ were 75.7%, 81.2%, 68.3%, and 75.0%, respectively. There were no differences in DLCO and FVC between the subgroups (p = 0.402 and p = 0.247, respectively). According to the patterns displayed on pulmonary CT scans, patients were divided into 3 groups: NSIP (n = 58), OP (n = 18), and UIP (n = 4). Obviously, the predominant CT pattern of ILD in patients with antisynthetase syndrome was NSIP (72.5%). No differences were found in the prevalence of these 3 CT patterns between the 4 groups.
Clinical features of patients with antisynthetase syndrome with RP-ILD
The distributions of different antisynthetase antibodies in patients with antisynthetase syndrome complicated with RP-ILD are shown in Table 2. More than half of the patients with antisynthetase syndrome with RP-ILD (6/11) were anti-PL7–positive. Nine patients received methylprednisolone pulse treatment, 8 received cyclophosphamide (CYC), and 7 received intravenous immunoglobulin. Six patients showed no response to therapy and died of respiratory failure. Of the 11 patients with antisynthetase syndrome who developed RP-ILD, the male:female ratio was 3:8. Notably, the 3 male patients with RP-ILD all had poor prognosis and 5 of 8 female patients experienced gradual improvement. Patients with antisynthetase syndrome with RP-ILD had higher proportions of neutrophils in their bronchoalveolar lavage fluid than those without RP-ILD (66.9% vs 29.1%, p = 0.006). The mean value of serum ferritin levels in patients with antisynthetase syndrome with RP-ILD was significantly higher than those without RP-ILD (1003.9 ng/ml vs 372.9 ng/ml, p = 0.013). Interestingly, the non-Jo1–positive patients with RP-ILD were all anti-Ro52 antibody–positive. CT patterns did not differ between RP-ILD and chronic ILD in patients with antisynthetase syndrome.
Characteristics of the 11 patients with antisynthetase syndrome complicated with rapidly progressive interstitial lung disease.
Survival analysis
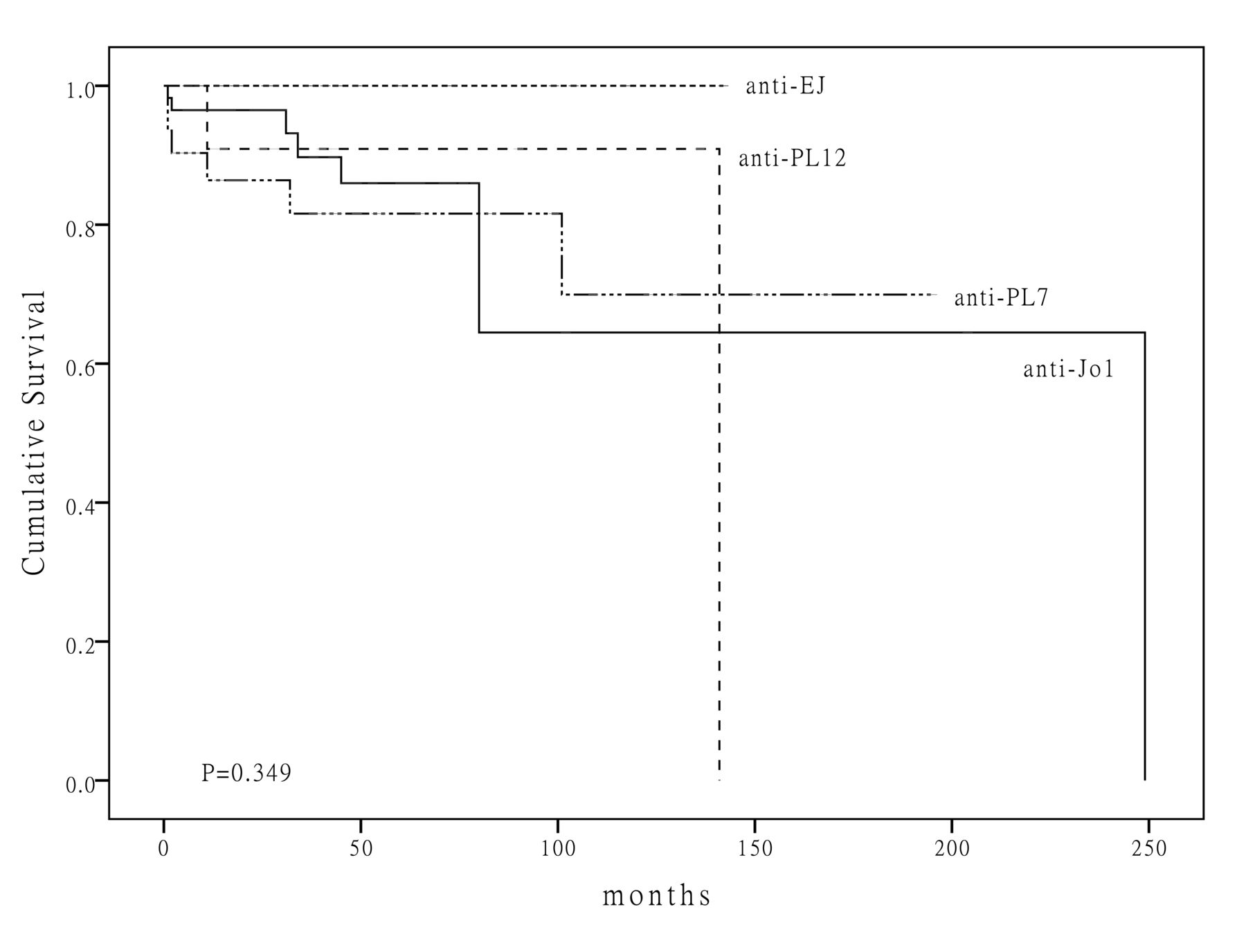
The followup duration ranged from 1 month to 249 months. The median followup time was 32.5 months. The cumulative 10-year survival rate of the cohort overall was 76.8%. The 1-year survival rates of patients with anti-Jo1, anti-PL7, anti-PL12, and anti-EJ were 96.5%, 86.4%, 90.9%, and 100%, respectively. The 5-year survival rates of patients with anti-Jo1, anti-PL7, anti-PL12, and anti-EJ were 86.0%, 81.6%, 90.9%, and 100%, respectively. The 10-year survival rates of patients with anti-Jo1, anti-PL7, anti-PL12, and anti-EJ were 64.5%, 69.9%, 90.9%, and 100%, respectively. Obviously, patients with anti-PL7 had the highest mortality within the first year of onset. The comparison of the Kaplan-Meier curves between the 4 antisynthetase antibodies subgroups, calculated by using the log-rank test, did not significantly differ (p = 0.349; Figure 1).
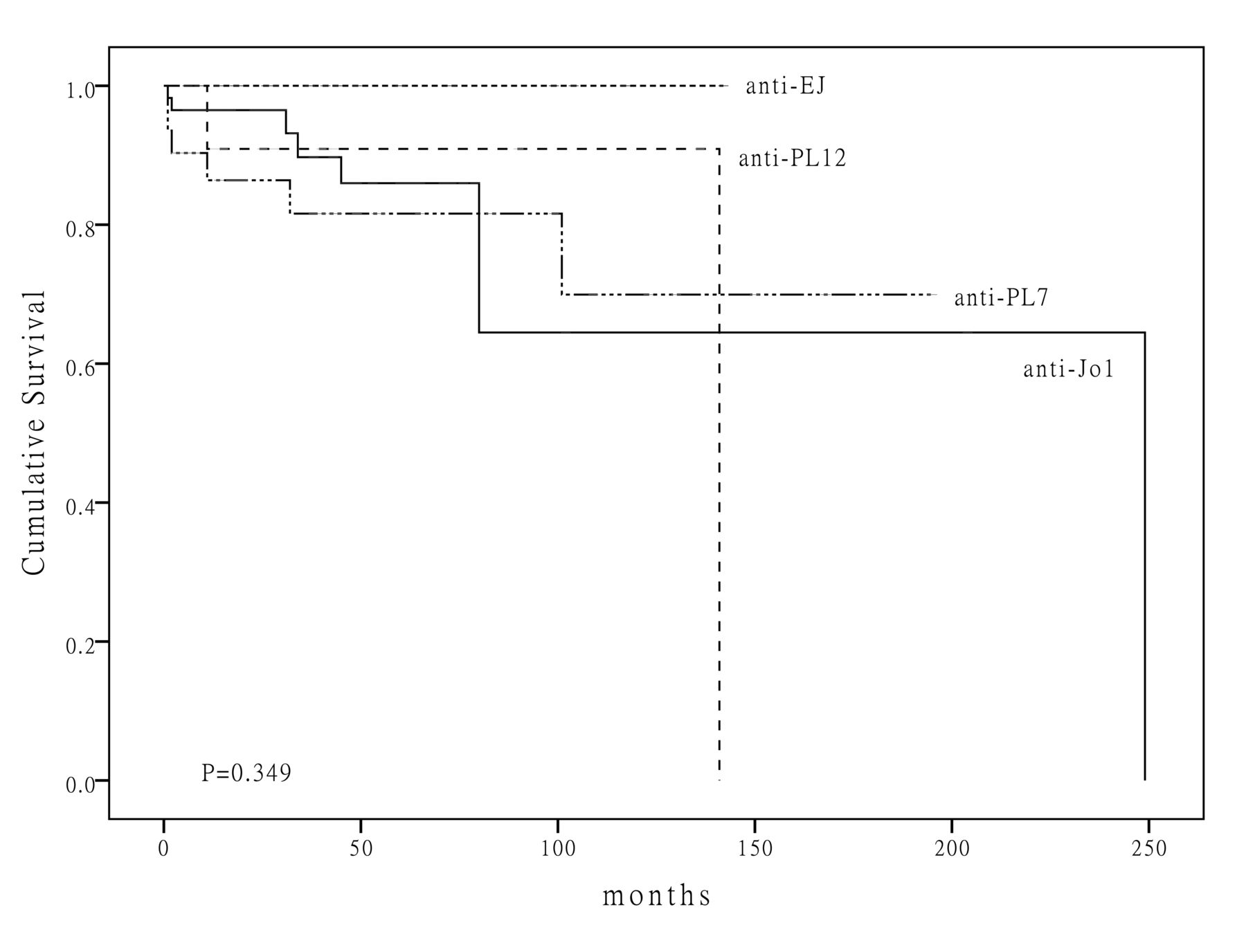
Survival curves in patients with polymyositis/dermatomyositis with 4 different antisynthetase antibodies.
Prognostic factors
To identify indicators of poor outcomes in patients with antisynthetase syndrome, multivariate Cox regression analysis was performed. The results of univariate analysis revealed that older age, presence of RP-ILD, malignancy, and elevated serum ferritin were significantly associated with poor outcomes in patients with antisynthetase syndrome (p = 0.005, p < 0.001, p = 0.001, and p = 0.018, respectively). The above factors were included in a multivariate analysis to identify prognostic factors. As shown in Table 3, RP-ILD, malignancy, and elevated serum ferritin were independent risk factors for poor prognosis in patients with antisynthetase syndrome. The 4 different antisynthetase antibodies were not predictive factors in the long term (all p > 0.05).
Multivariate Cox regression analysis of prognostic factors in patients with antisynthetase syndrome.
DISCUSSION
In our study, we compared the differences of patients with IIM with distinct antisynthetase antibodies in terms of clinical, serological, and radiological aspects, and the analysis especially focused on the association between antisynthetase antibodies and ILD. Further, longterm outcomes and prognostic factors were identified in patients with antisynthetase syndrome.
The presence of ILD usually contributes to mortality and morbidity in patients with myositis. In our cohort, the overall prevalence of ILD was 94.4% and even reached 100% in patients with anti-PL12 and anti-EJ antibodies, higher than published reports5,19,20. Similarly to other ethnic groups21,22, no differences were detected in pulmonary function variables and ILD pattern based on antisynthetase antibodies subtype.
The main cause of mortality in our cohort was ILD-associated respiratory failure, particularly respiratory failure associated with RP-ILD. Several published reports have stated that severe acute lung injury occurs in patients with anti-Jo123,24,25. It also has been described that anti-PL7 and anti-PL12 are closely associated with severe ILD26,27,28,29. In our cohort, patients with antisynthetase syndrome with anti-Jo1 and anti-PL12 did not experience more RP-ILD than other patients with antisynthetase syndrome. In contrast, patients with anti-PL7–positive antibodies have markedly higher incidence of RP-ILD compared with patients with antisynthetase syndrome without anti-PL7. Our study shows that anti-PL7–positive patients have higher mortality rates in the early stages of survival curves in comparison with other patients with antisynthetase syndrome. In accordance with a previous study5, heliotrope rash was more prevalent in anti-PL7–positive patients than other clinical manifestations. Labirua-Iturburu, et al found that anti-PL7 was related to pericarditis30; the high prevalence of pericarditis is also observed in our cohort. These findings may indicate that patients with anti-PL7 exhibit a distinct clinical phenotype.
Further, our results confirm that the coincidence of anti-Ro52 in antisynthetase syndrome predicts RP-ILD. The frequency of anti-Ro52 in patients with anti-Jo1 reached 65% in 1 published report19. Nevertheless, our study demonstrates that anti-Ro52 is more prevalent in patients with non-Jo1 antibodies and associated with RP-ILD, particularly in anti-PL7–positive patients. Thus, it is indicative that the combination of anti-PL7 and anti-Ro52 is a predictive marker of RP-ILD. But whether the anti-PL7 and anti-Ro52 antibodies are directly involved in the development of RP-ILD has not been determined.
Obviously, RP-ILD contributes to increased mortality rates. Regarding therapy responsiveness, fewer than half of the patients with antisynthetase syndrome with RP-ILD in our study responded well to high-dose steroid and immunosuppressive therapy. The first-line therapeutic regimen is to initiate steroid pulse and CYC treatments in patients with antisynthetase syndrome with RP-ILD in our cohort. Effective treatments using rituximab, cyclosporine, and tacrolimus have been reported in severe ILD cases13,31,32,33,34,35. However, to date, there have been no reported controlled clinical trials to validate any 1 therapy for RP-ILD as optimal.
Regarding the association between the antisynthetase antibodies with prognosis, previous reports showed that the presence of antisynthetase antibodies predicts favorable outcomes36. The survival rates decreased more rapidly in patients with anti-PL7 in the early longterm followup; patients with anti-PL7 had the highest mortality within first year of onset, but patients with anti-Jo1 had the lowest 10-year survival rate. Patients with antisynthetase syndrome with anti-EJ had better outcomes than other patients with antisynthetase syndrome in the long term. Despite these differences, in the survival analysis, the antisynthetase antibodies did not significantly affect patients’ longterm outcomes. In multivariate analysis, the antisynthetase antibodies also did not affect prognosis. Two possible reasons why the differences observed in survival analysis were not significant may be the relatively short followup time and a relatively small sample size.
Regarding ILD patterns in antisynthetase antibodies-positive patients, CT scans were routinely performed in clinical practice. Radiologically, NSIP was the most common pattern seen upon initial diagnosis, followed by OP and UIP. However, no relationship was found between the CT patterns of ILD and the therapeutic response of patients complicated with RP-ILD. Because lung biopsy is infrequently performed, histological features cannot be obtained and the differences cannot be compared between the patients with distinct antisynthetase antibodies. Yousem, et al found the nonconformity of radiological and biopsy results, and UIP was the dominant ILD pattern in patients with anti-PL737. Thus, biopsy confirmation is still needed in clinical settings. Further, the mechanism behind the association between the severity of ILD and pathological patterns also requires more research to determine.
Apart from RP-ILD, our results show that hyperferritinemia is also an indicator of worse outcomes in patients with antisynthetase syndrome according to survival analysis. Hyperferritinemia has been described as closely associated with RP-ILD in patients who are antimelanoma differentiation-associated protein 5 antibody–positive18,38,39. Our results also show that serum ferritin is dramatically elevated in patients with antisynthetase syndrome complicated with RP-ILD. Therefore, serum ferritin not only confers a poor outcome, but also can be used to monitor antisynthetase syndrome disease activity.
IIM has been demonstrated to be closely associated with malignancy. Chinoy, et al reported that traditional routinely assayed myositis antibodies (including anti-Jo1) have a significantly lower cancer risk than dermatomyositis patients without antibodies40. Our finding that malignancy occurs in 6.5% of patients with antisynthetase syndrome is consistent with the observation by Chinoy, et al. Marie, et al also reported that anti-Jo1–positive patients with anti-Ro52 antibody experienced more malignancy than those without anti-Ro5214. However, we did not find any association between anti-Ro52 antibody and malignancy in patients with antisynthetase syndrome.
Taken together, our results suggest the distinctiveness of the anti-PL7 antibody despite the homogeneity of different antisynthetase antibodies and confirm the link between anti-PL7 and RP-ILD. In addition, we found that the presence of anti-Ro52 in patients with antisynthetase syndrome also predicts RP-ILD. Other prognostic indicators for poor outcomes of patients with antisynthetase syndrome include malignancy and hyperferritinemia. Further studies are required to elucidate the differences between distinct antisynthetase antibodies.
Footnotes
Supported by the National Natural Science Foundation of China (91542121, 81571603), the Capital Foundation of Medical Developments (No: 2016-2-4063), and the Science and Technology Commission Foundation of Beijing (Z151100004015143).
- Accepted for publication March 23, 2017.








{kind=link}