

Abstract
Objective. Power Doppler ultrasound (PDUS) has been shown to detect subclinical synovitis in psoriatic arthritis (PsA), but its value is not yet fully understood. The aim of this study was to evaluate PDUS features at joint level in patients with PsA in clinical remission and to investigate its value for predicting short-term flares.
Methods. Consecutive patients with PsA in clinical remission according to the attending rheumatologist and who fulfill minimal disease activity criteria and/or 28-joint Disease Activity Score in remission criteria underwent PDUS examination of 18 joints. All patients were followed up for 6 months. Disease flare was defined as any increase of disease activity generating the need of any of the following changes in therapy with disease-modifying antirheumatic drugs (DMARD) by the attending rheumatologist: dose increase, switch or addition of a different DMARD, and/or switch or addition of biological therapies.
Results. Among 54 patients with PsA in clinical remission, 15 (27.8%) experienced a flare within the next 6 months. Twenty patients had at least 1 joint with PDUS synovitis at baseline, and 13 (65%) of these had a disease flare during the followup period compared with only 2 of the 34 patients (5.9%) without baseline PDUS synovitis (relative risk = 11, 95% CI 2.8–44, p < 0.001). On logistic regression analysis, the only variables associated with short-term flares were baseline PDUS synovitis and the use of nonbiologic DMARD.
Conclusion. Among patients with PsA in clinical remission, PDUS-detected synovitis was a strong predictor of short-term flare of the disease.
Psoriatic arthritis (PsA) is a chronic inflammatory disease associated with cutaneous psoriasis with wide variation in the incidence and prevalence among different regions of the world1,2. PsA frequently has a chronic and progressive course. However, an early diagnosis, tight control of the disease, and the treat-to-target methodology would be effective measures to achieve a better prognosis in these patients3. The European League Against Rheumatism (EULAR) working group and the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis set out recommendations based on evidence for the treatment of PsA4,5. Both recommendations support the concept that treatment should aim for remission, or alternatively, minimal/low disease activity. The concept of remission and of sustained remission as the goal of treatment is shared by most experts around the world6,7,8,9,10,11,12. Flares imply a loss of remission status with return to active inflammatory stages, and ideally should be avoided. Remission criteria are based mainly on clinical evaluation. However, clinical assessment has limitations because of its low sensitivity to detect true synovitis, tenosynovitis, dactylitis, and enthesitis, potentially underestimating the inflammatory process13,14,15,16,17. Imaging techniques, such as ultrasound (US) and magnetic resonance imaging, have the ability to visualize the inflammatory process. US has become increasingly accessible for rheumatologists and is widely used in the evaluation of patients with inflammatory joint diseases. There is evidence of presence of subclinical synovitis (detected by US) in patients with rheumatoid arthritis (RA) in clinical remission and its association with worse clinical and radiological outcomes18,19,20. Similarly, some studies have demonstrated the ability of US to detect subclinical inflammation in patients with PsA, leading both to a disparity between clinical composite scores and US findings17, and also to reclassification of patients with clinical oligoarthritis (< 5 swollen joints) to US polyarthritis (≥ 5 swollen joints)21. The significance of these subclinical findings in patients with PsA in clinical remission is not clear because there is scarce information on the value of US features as predictors of clinical and functional outcomes on followup.
The main aim of our present study was to evaluate power Doppler US (PDUS) features at joint level in patients with PsA in clinical remission and to investigate its value for predicting short-term flares.
MATERIALS AND METHODS
Consecutive patients with a diagnosis of PsA according to the ClASsification for Psoriatic ARthritis criteria (CASPAR)22 and in clinical remission were included. Clinical remission was defined as the absence of disease activity determined by the attending rheumatologist and by fulfilling the minimal disease activity (MDA) criteria23 and/or the Disease Activity Score in 28 joints (DAS28) remission criteria (< 2.6)24, regardless of the treatment received.
The study was conducted according to the Declaration of Helsinki and local regulations. Ethical approval for the study was obtained from the hospital’s local ethics committee (Comite de Etica de Protocolos de Investigacion, approval number: 1955), and informed consent was obtained from all patients.
Baseline clinical assessment
All necessary information to complete MDA and DAS28-erythrocyte sedimentation rate was collected. Demographic characteristics, including age and sex, were assessed. Disease duration and duration of remission was also documented. Type of disease-modifying antirheumatic drugs (DMARD) received at the time of evaluation was recorded. Severity of psoriasis was scored according to the Psoriasis Area and Severity Index. Nails were assessed on each patient and psoriatic nail involvement was graded using the modified Nail Psoriasis Severity Index. Musculoskeletal assessment was performed according to standard clinical procedures and included tender joint count in 68 joints, swollen joint count in 66 joints, visual analog scale with respect to patient’s global perception of disease activity, Leeds Enthesitis Index, and Leeds Dactylitis Index. Function was assessed by the Argentinean version of the Health Assessment Questionnaire-Disability Index25.
Baseline US examination
All US examinations were performed by the same rheumatologist experienced with this imaging technique, blinded to clinical data, on the same day as the clinical assessment. Patients were asked not to talk with the operator during the US examination of their clinical condition. A MyLab 70 machine (Esaote) with 2 different multifrequency linear transducers (4–13 and 6–18 MHz) was used. The following joints were assessed bilaterally: wrist, second and third metacarpophalangeal, second and third interphalangeal, knee, ankle, and second and fifth metatarsophalangeal, giving a total of 18 assessed joints per patient. The standardized scanning method recommended by EULAR was used and joint cavity widening, due to the presence of synovial fluid and/or synovial hypertrophy (greyscale synovitis) according to the Outcome Measures in Rheumatology preliminary definitions, was evaluated at each joint26,27. All joints were evaluated with PD technique to assess the presence of increased abnormal synovial vascularization. Intraarticular PD signal was scored on a semiquantitative scale from 0 to 3 (grade 0 = no intraarticular PD signal; grade 1 = presence of a single PD signal; grade 2 = 2 or more confluent foci of PD signal, but occupying < 50% of intraarticular area; grade 3 = PD signal in > 50% of the intraarticular area). To maximize PD sensitivity and try to avoid the presence of artifacts, the settings of PD were adjusted as follows: low pulse frequency repetition (between 500 Hz and 1000 Hz), dynamic range 20–40 dB, low wall filters (2–3), and PD gain below the level at which color noise appeared in the underlying bone28,29,30,31.
An US score (range 0–54) was constructed by summing PD values of each of the individual joints assessed.
Followup
All patients were followed for 6 months after baseline clinical and US examinations to assess disease flares. A disease flare was defined as any increase of disease activity generating the need for any of the following changes in therapy with DMARD by the attending rheumatologist: dose increase, switch or addition of a different DMARD, and/or switch or addition of biological therapies19,32.
Statistical analysis
Descriptive statistics were used to summarize patients’ characteristics. Continuous variables were expressed as medians and interquartile range (IQR) or as means and SD, and categorical variables were expressed as percentages with their corresponding 95% CI. Comparisons were performed using parametric and nonparametric tests for continuous variables and the chi-square test for categorical variables. Relative risk (RR) and 95% CI for the occurrence of disease flare was calculated between patients with and without baseline PD signal. A multivariate logistic regression analysis using the presence of disease flares as the outcome variable, and the presence of PD signal, demographic characteristics, disease activity, and treatment as independent variables, was also conducted. Sensitivity, specificity, and positive and negative likelihood ratios (LR) of PD signal for detecting short-term flare in patients with PsA in remission were also calculated.
RESULTS
Baseline demographic and clinical features
A total of 54 patients with PsA were included (Table 1). All patients were in clinical remission according to their attending rheumatologist, and all met at least 1 of the remission criteria (MDA and/or DAS28). Forty-seven (87%) were in remission according to MDA criteria, 36 (67%) according to DAS28, and 29 (54%) by both criteria (MDA and DAS28). The median time in remission at baseline was 5.5 months (IQR 2–12). Most patients (n = 40, 74%) had no swollen joints. Of the 14 (26%) remaining patients, 10 had only 1 swollen joint, 3 had 2 swollen joints, and 1 had 3 swollen joints. Thirty-five patients (65%) were treated with DMARD, with most patients receiving methotrexate (31 out of these 35 patients) and 12 (22%) receiving biologic therapy with tumor necrosis factor-α inhibitors (TNFi). All patients receiving DMARD or TNFi continued treatment during the 6-month followup period or until they had a flare. Only 7 patients were in clinical remission and without treatment.
Baseline demographic, clinical, and US features of patients with PsA (n = 54). Values are mean (SD) unless otherwise specified.
Baseline US features
Joint cavity widening, due to the presence of synovial fluid and/or synovial hypertrophy (greyscale synovitis), in at least 1 joint was detected in 30 patients (55.5%). Twenty patients (37%) had synovitis with PD grade ≥ 1 in at least 1 of the examined joints (Table 1). Eight of these 20 patients had only 1 joint with PD signal, while the remaining 12 had 2 or more joints with positive PD. From a total of 972 joints evaluated, 38 (4%) showed increased abnormal vascularization. PD grade 1 was detected in 19/38 joints (50%), PD grade 2 in 17/38 joints (44.7%), and PD grade 3 was seen in only 2/38 joints (5.3%). The most frequently involved joint was the wrist (34.2%, 13/38; Figure 1). The mean (SD) of the US score was 1 (1.9; Table 1).
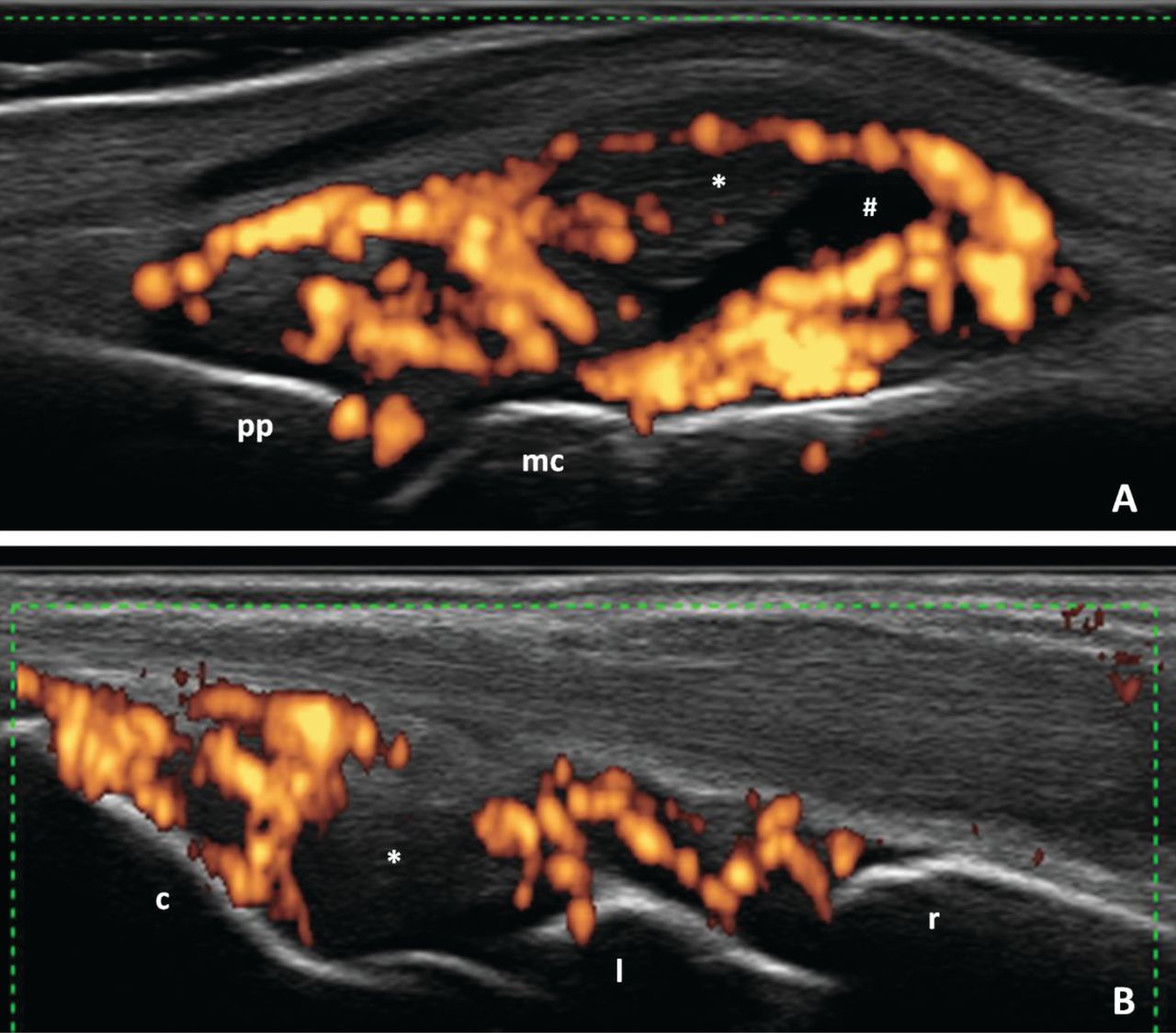
Representative ultrasound images obtained during the study. (A) Metacarpophalangeal joint. Longitudinal dorsal scan. # Joint cavity widening with synovial fluid. * Synovial hypertrophy with increased intraarticular abnormal vascularization by power Doppler. pp: proximal phalanx; mc: metacarpal head. (B) Wrist. Longitudinal dorsal scan. * Joint cavity widening with predominant synovial hypertrophy and increased intraarticular abnormal vascularization by power Doppler. r: radius; l: lunate; c: capitate.
Flares and associated factors
Fifteen of the 54 patients (27.8%) had a disease flare during the followup period of 6 months (Table 2). Eleven out of 15 (73.3%) disease flares were characterized by inflammatory articular involvement, 3/15 (20%) by both inflammatory articular and enthesis involvement, and 1/15 (6.6%) by the presence of dactylitis. Patients who had a flare were significantly older and were more frequently treated with DMARD than those who did not have a flare (p = 0.011 and p = 0.037, respectively; Table 3). Twenty patients (37%) had at least 1 joint with PD grade ≥ 1 at baseline; 13 (65%) of these patients had a disease flare during followup period. Only 2 of the 34 patients (5.9%) without baseline US synovitis with PD grade ≥ 1 had a flare of the disease during followup (RR = 11, 95% CI 2.8–44, p < 0.001). Eleven patients had at least 1 joint with PD grade ≥ 2 at baseline; 8 (72.7%) of these had a disease flare during followup period. Among 43 patients without US synovitis with PD grade ≥ 2, 7 (13.9%) had a disease flare during followup (RR = 4.5, 95% CI 2.0–9.6, p < 0.001; Table 4).
Percentage of disease flares according to the different applied remission criteria. Values are n (%; 95% CI) unless otherwise specified.
Comparative analysis of patients’ baseline features according to the presence of disease flares during the 6-month followup period. Values are mean (SD) unless otherwise specified.
Univariate analysis of baseline PDUS features and their relationship with disease flares during the followup period.
In univariate analysis, no other variable (not even greyscale synovitis) was associated with an increased risk of flare (Table 3).
In multivariate analysis, the only variables that were associated with the occurrence of flares were US synovitis with PD grade ≥ 1 in at least 1 joint (OR 35.5, 95% CI 4.5–283) and the concomitant use of DMARD (OR 12.7, 95% CI 1.03–158).
Diagnostic test properties of the PD signal for detecting flares
Sensitivity and specificity of the presence of intraarticular PD signal at baseline for the detection of flare was 87% (95% CI 59.5–98) and 82% (95% CI 62.5–92.5), respectively. The positive LR was 4.8 (2.4–9.7), while the negative LR was 0.1 (0.4–0.6).
US score and flares
The mean (SD) US score in patients who had a flare was 3 (2.5) and in those without flare was 0.3 (0.9; p < 0.001). The area under the receiver-operating characteristic curve of the US score for the prediction of flare was 0.88 (95% CI 0.77–0.95). An US score ≥ 1 showed the best cutoff point, with a sensitivity of 86.7% and a specificity of 87.2% for predicting flare (positive LR: 6.7, negative LR: 0.1).
DISCUSSION
One of the most important goals in the treatment of patients with PsA is to reach a state of sustained clinical remission. A major challenge is to recognize that patients who are in remission are at an increased risk of experiencing a disease flare. US has been shown to detect subclinical inflammation in patients in clinical remission, but the prognostic value of this feature was not proved until now. Therefore, we evaluated the predictive value of PDUS for short-term flare in patients with PsA in clinical remission.
The percentage of patients with PsA in clinical remission with synovitis detected by PDUS in our cohort (37%) was lower than the one reported by Nguyen, et al from a metaanalysis of patients with RA (44%) in clinical remission20. It was higher than the one reported by Araujo, et al in patients with PsA in clinical remission33. In our cohort of patients with PsA in clinical remission, around a quarter (27.8%) experienced a flare during the 6-month followup period. This was low compared with the high incidence of disease recurrence reported by Araujo, et al (76.9%)33. This difference occurred possibly because in the study by Araujo, et al, the incidence of disease recurrence was evaluated after discontinuation of DMARD treatment, while the majority of patients in our study (47/54) remained with their corresponding DMARD or TNFi therapy during the followup period.
The main result of our study was that US-detected synovitis with PD grade ≥ 1 at baseline in patients with PsA in clinical remission was a strong predictor of flare during short-term followup (RR: 11, 95% CI 2.8–44, p < 0.0001). The presence of US synovitis with positive PD signal despite clinical remission suggests that flares may be related to an incomplete suppression of inflammation, undetectable by the clinical indices used in daily rheumatology practice. Therefore, once the patients have achieved clinical remission, an US examination with PD technique could predict the probability of remaining in remission. A small percentage of patients (5.9%) without PDUS synovitis at baseline showed a flare, so a negative result on PDUS would provide an adequate degree of confidence of sustained remission during short-term followup.
We also found that the use of DMARD was associated with increased risk of disease flares compared with patients not treated with DMARD and with patients receiving biologic therapy. Although there is not a clear explanation for this, our interpretation is that patients not receiving DMARD are patients with mild disease less prone to flare, and patients with biologics are treated more intensively and less likely to flare.
Our study has some limitations. First, the choice of the joints to be evaluated by US was arbitrary and based on only the frequency of joint involvement in PsA and previous studies in patients with RA and PsA. Second, there is no universally accepted definition of flare in PsA. The definition we used was extrapolated from RA and has not been validated in PsA. Third, we did not evaluate by US the presence of enthesitis and/or dactylitis as main features of PsA. This could underestimate the inflammatory involvement detected by PDUS at baseline. Finally, we did not assess the interobserver and intraobserver reliability regarding US findings that could increase the internal validity of our study.
Among patients with PsA in clinical remission, PDUS-detected synovitis was a strong predictor of short-term flare of the disease.
Footnotes
Supported by a PANLAR (Pan-American League of Associations of Rheumatology) Prize and by an investigator-originated study grant from Abbvie.
- Accepted for publication March 22, 2017.








{kind=link}