

Abstract
Objective. Magnetic resonance imaging (MRI) is involved in the assessment of axial spondyloarthritis (axSpA); however, anecdotal evidence suggests diverse practice among radiologists. The objective of this study was to describe current practice in the use of MRI for assessment of axSpA by UK radiologists.
Methods. Six hundred ninety-nine UK radiologists were invited to complete an online survey. Availability of MR scanners, familiarity with axSpA disease-specific lesions, and MRI protocols and definitions of positive sacroiliac joint (SIJ) or spinal MRI were assessed.
Results. Two-hundred sixty-nine radiologists (38%) from 131/180 (73%) acute UK National Health Service trusts/health boards responded. MRI waiting times < 2 months were reported by 90% of radiologists. Twenty-nine radiologists (11%) used contrast as standard, 256 (91%) used T1 and short-tau inversion recovery, and 172 (64%) also used T2 sequences. Five percent scanned only SIJ, 33% scanned SIJ and lumbar spine, 29% scanned SIJ and thoracolumbar spine, and 30% scanned SIJ and the whole spine. Mean scan time was 34 min. Eighteen percent did not use the subchondral bone marrow edema of the SIJ to help diagnose axSpA and 18% did not use the inflammatory vertebral corner lesions to assist diagnosis. Awareness of axSpA was reported by 75% of radiologists, and awareness of definitions for positive MRI of SIJ and spine by 31% and 25%, respectively.
Conclusion. These data highlight the need for better rheumatology-radiology collaboration on the identification of diagnostic axSpA MRI lesions and support the need for a consensus on the most appropriate MRI protocols for the assessment of axSpA.
The use of magnetic resonance imaging (MRI) has been instrumental in the early recognition of axial spondyloarthritis (axSpA). Indeed, the superior capability of MRI to identify active inflammatory lesions has allowed for the identification of an earlier phase of the disease, which was not possible using conventional radiography. The 2009 Assessment of Spondyloarthritis international Society (ASAS) classification criteria1 refer to this disease stage as “nonradiographic” (nr-axSpA), where axial inflammation is often detectable on MRI but not on conventional radiography. Patients with nr-axSpA have pain and disease activity similar to that of those patients with established ankylosing spondylitis (AS). Therapies are now available for symptom control2 that potentially modify disease activity, emphasizing the importance of early diagnosis.
According to the ASAS criteria, nr-axSpA can be identified using either a clinical or imaging arm1. The latter is defined by the presence of sacroiliitis by either radiograph or MRI, in addition to 1 other feature of axSpA. It is, however, recognized that spinal disease may occur early and in isolation from sacroiliitis in 23% to 49% of cases3,4, and may help support a diagnosis of axSpA in appropriate clinical presentations5,6. It is also useful in predicting spinal outcome7 and may help to determine treatment response to antitumor necrosis factor (TNF) therapy4. The ASAS group published a consensus document defining a positive spinal MRI for axSpA8. Most recently, the newly published UK National Institute for Health and Care Excellence (NICE) final appraisal determination for the use of anti-TNF therapy for AS and nr-axSpA9 suggests that inflammation in either the sacroiliac or spine as determined by MRI is one of the prerequisites for the treatment of nr-axSpA with anti-TNF therapy, emphasizing the importance of the correct use and interpretation of MRI in the assessment of axSpA.
Anecdotal evidence suggests that variations may exist in access to services, treatment, availability of imaging, and expertise of those interpreting the images of patients with axSpA within the United Kingdom. A survey by Hamilton, et al10 indicated that whereas 93.1% of rheumatology departments (109/117) had access to an MRI scanner on site, only 78.6% (92/117) had a dedicated musculoskeletal radiologist, with only a small percentage of musculoskeletal radiologists specializing in inflammatory rheumatology. This survey also indicated that a variety of different MRI protocols were being used to investigate axSpA. The majority of rheumatologists are dependent on the radiologist for interpreting complex imaging investigations such as MRI. A survey of ASAS international members with a specialist interest in axSpA identified that < 25% of rheumatology members were comfortable interpreting MRI scans in patients with axSpA11.
The aim of our study was to investigate the level of awareness of axSpA and to formally establish current common practice and knowledge in the use of MRI in the assessment of axSpA among UK-based radiologists.
MATERIALS AND METHODS
Six hundred ninety-nine consultant radiologists currently working within a UK National Health Service (NHS) trust (England) or health board (Scotland, Wales, or Northern Ireland) were approached and invited to participate in a 15-min online survey (Supplementary Data, available with the online version of this article). The survey was completed anonymously and did not include any patient data; therefore, ethical review and approval were not required in accordance with local ethics committee guidance. The survey analyzed the availability of local MRI services, collaboration between rheumatologists and radiologists, knowledge of axSpA, and standard MRI protocols and sequences used in assessing patients with probable axSpA. The knowledge of radiologists on diagnostic MRI lesions and standard definitions of a positive MRI for the sacroiliac joint (SIJ) and the spine in axSpA was also assessed. Data were analyzed using descriptive statistics and are presented as n (%) or mean (range).
RESULTS
Of the 699 consultant radiologists who were contacted, 269 (38%) completed the questionnaire, with respondents covering 73% (131 of 180) of acute NHS trusts and health boards in the United Kingdom. Fifty-two responding radiologists (40%) worked in university teaching hospitals and 79 (60%) worked in district general hospitals. All but 1 unit reported access to an MRI scanner, with a median of 2 MRI scanners available for each responding radiologist. Waiting times of < 2 months were reported by 90% of radiologists (n = 242). Regular meetings with rheumatology colleagues were reported by 65% of radiologists (n = 174), 23% (n = 61) reported meeting as required, and 13% (n = 34) reported never meeting with local rheumatologists.
Use of MRI in the diagnosis of axSpA
Of the 269 radiologists who completed the survey, 175 (65%) reported using MRI in the diagnosis of axSpA only when specifically requested to do so by rheumatologists. Eighteen percent of radiologists (n = 48) routinely used MRI instead of radiographs of the SIJ and spine, and 12% (n = 32) used MRI only if radiographs were not diagnostic. The mean reported time to perform an MRI for axSpA was 34 min (range 14–90 min, n = 269).
MRI protocols
Five percent of radiologists reported scanning the SIJ alone, 33% scanned the SIJ and lumbar spine, 29% scanned the SIJ and the thoracolumbar spine, and 30% scanned the SIJ and whole spine (Figure 1A) as part of their standard axSpA MRI protocol. Of those radiologists who did not routinely scan any of the spine, 12% reported this was because of scan times taking too long, 9% reported that it was too costly to scan the spine, and 8% reported that either there were no specific MRI spinal features of axSpA or spinal lesions were not used in the diagnosis of axSpA.

Routine use of MRI by UK radiologists when investigating for axial spondyloarthritis. (A) Regions of the axial skeleton scanned. (B) MRI sequences performed for scanning the spine. (C) MRI sequence protocols performed for scanning the axial skeleton. MRI: magnetic resonance imaging; SIJ: sacroiliac joint; STIR: short-tau inversion recovery.
MRI sequences and use of contrast
When scanning the spine, 54% of radiologists reported performing sagittal and axial sequences of the spine, 26% performed sagittal, axial, and coronal sequences, and 16% performed sagittal slices only (Figure 1B).
Use of T1 protocols with either short-tau inversion recovery or other fat-suppressed sequences was reported by 91% of radiologists, with 23% performing these sequences in isolation. Inclusion of additional T2 sequences was reported by 64% of radiologists and 11% reported using contrast and performing T1 post-gadolinium sequences (Figure 1C).
Knowledge of axSpA and MRI lesions and definitions
Awareness of the term axSpA was reported by 75% of radiologists (n = 202). Awareness of the ASAS definitions of a positive MRI for axSpA for the SIJ and for the spine was reported by 31% (n = 84) and 25% (n = 67) of radiologists, respectively.
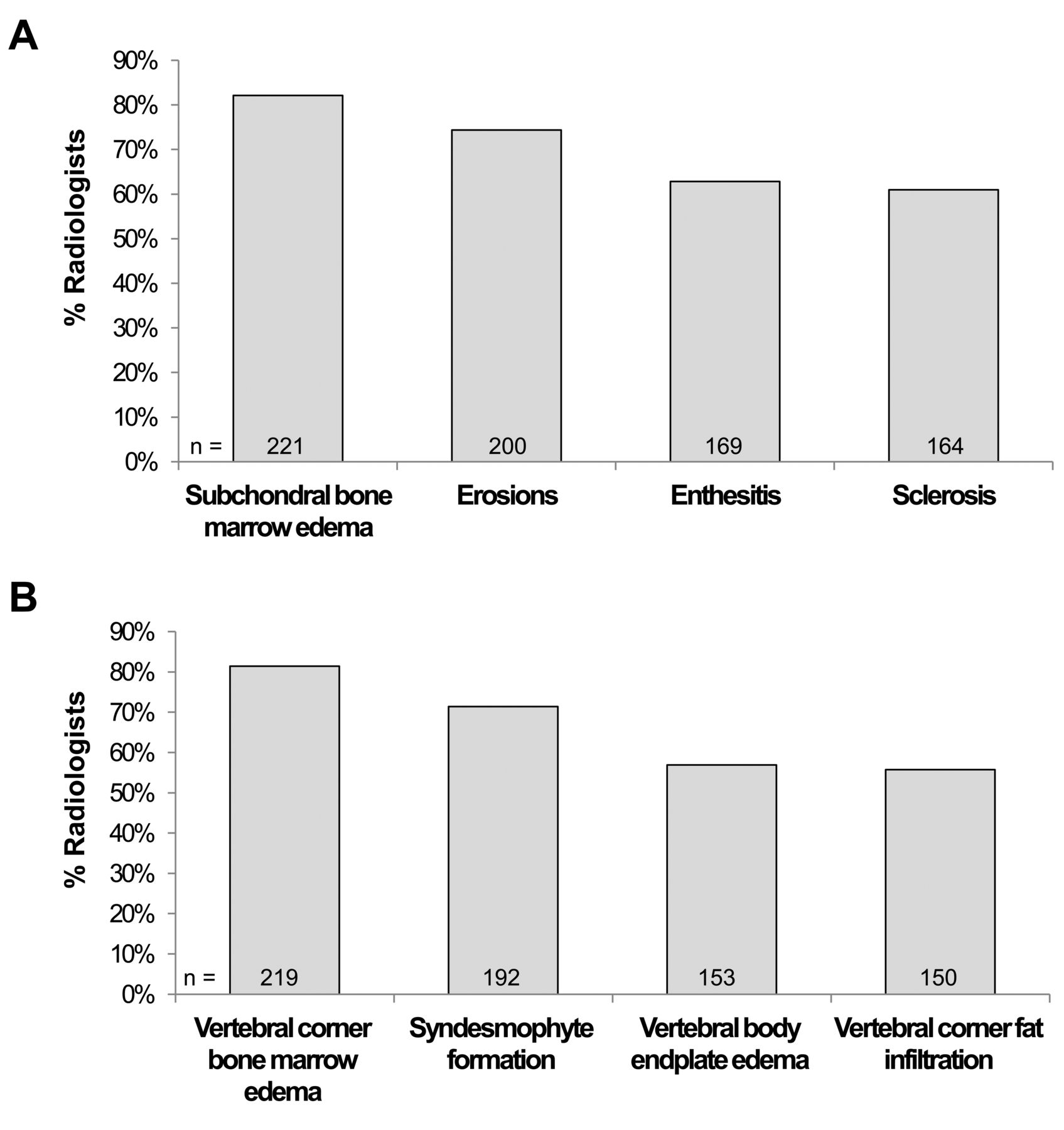
The lesions most frequently used to diagnose axSpA in the SIJ were reported to be subchondral bone marrow edema (82%), erosions (74%), enthesitis (63%), and sclerosis (61%, not mutually exclusive; Figure 2A). In the spine, the lesions used most frequently to diagnose axSpA were reported to be vertebral corner bone marrow edema (81%), syndesmophyte formation (71%), vertebral body endplate edema (57%), and vertebral corner fat infiltration (56%, not mutually exclusive; Figure 2B). For both SIJ and spinal MRI, 96% of responding radiologists used a combination of the above lesions to assist in making a diagnosis of axSpA.
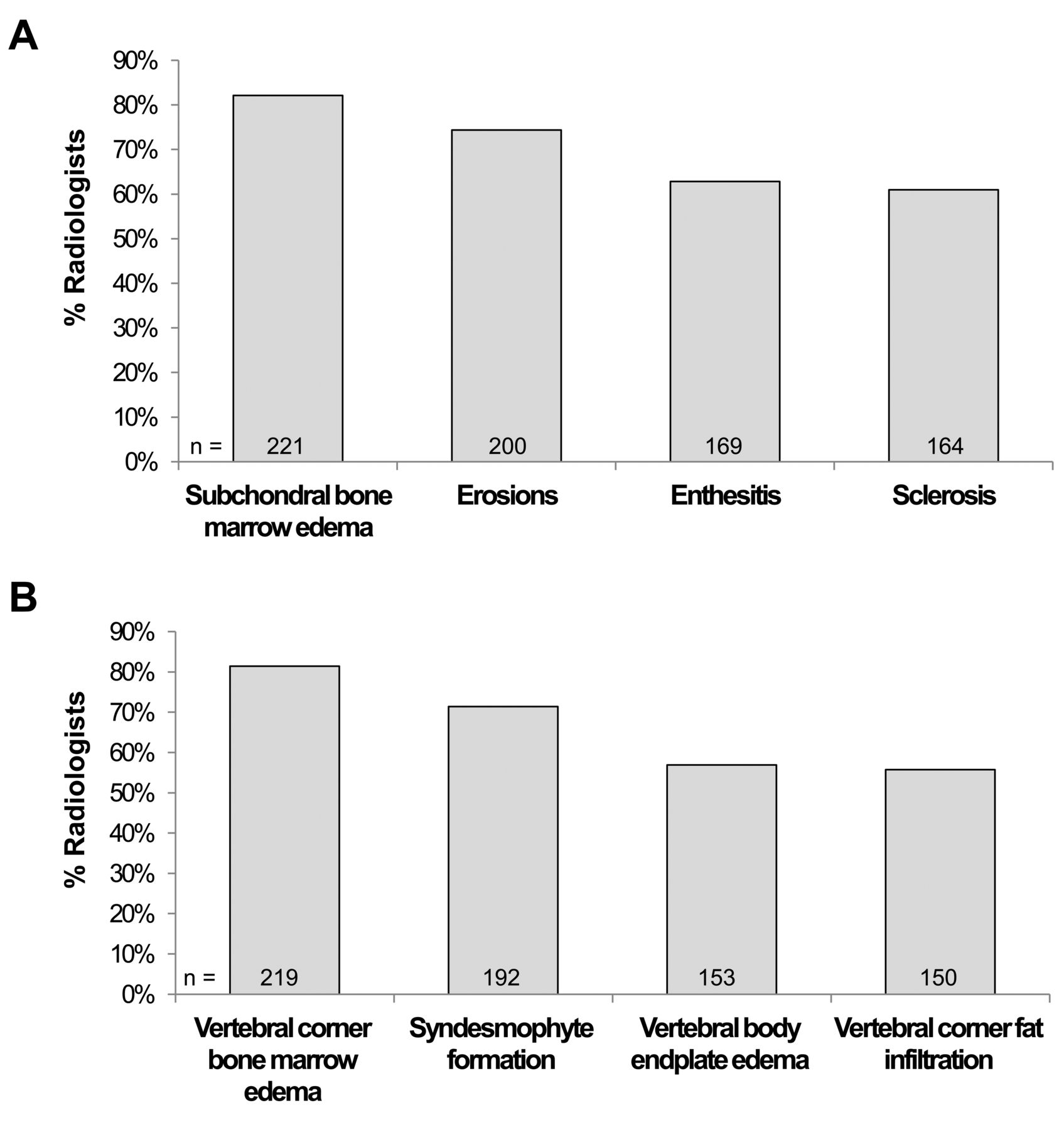
Lesions most frequently used by UK radiologists to diagnose axial spondyloarthritis. (A) Sacroiliac joint lesions. (B) Spine lesions.
DISCUSSION
Data from our study show that among UK radiologists, the awareness of axSpA is variable, there is relatively poor knowledge of positive MRI definitions of axSpA, and there is diverse use of MRI in the diagnosis of axSpA. The concept of SpA is not new, dating back to Wright and Moll in 197612; however, the use of MRI to diagnose and classify axSpA is relatively recent. The ASAS classification criteria published in 20091 were the first to formalize the involvement of MRI in the diagnosis of axSpA. Subsequently, definitions of a positive MRI for the SIJ13 and the spine8 that indicate the presence of axSpA have been published, aiming to standardize implementation of the criteria. The European Society of Skeletal Radiology (ESSR) consensus publication on the imaging and interpretation of MRI in axSpA stated that in the cases of suspected axSpA with normal radiographs, MRI is mandatory14. Further, combined scanning of the whole spine and the SIJ, rather than the SIJ alone, was recommended to enhance confidence in diagnosing nr-axSpA, and specific MRI protocols are provided for scanning the spine and SIJ in the diagnosis of axSpA. These modified whole-spine and SIJ protocols are cost-and time-effective, and can be performed in a standard 30-min MRI slot14,15. Yet, despite these internationally published recommendations, our current study indicates that only 30% of radiologists scanned the whole spine and SIJ. Indeed, methods for using MRI in the diagnosis of axSpA across the United Kingdom were diverse and generally did not follow the ESSR protocol.
Our study indicates that, although MRI is readily available to the majority of radiologists, with waiting times of generally < 2 months, there is a lack of consistency in the MRI protocols and sequences used to investigate axSpA. This diversity and inconsistency of practice across the United Kingdom, with different areas of the spine being scanned and different sequences being used despite clear recommendations from the international ESSR consensus publication, is of concern because it highlights potential inequalities in the diagnosis and assessment of affected individuals14. Further, our data indicate that > 10% of UK radiologists are using intravenous contrast (with the subsequent potential risk to patients16,17 and increased cost and time of the investigation), going against published guidance14,18,19.
AxSpA is a condition that often has little objective evidence of disease, both clinically and on investigation. Unlike rheumatoid arthritis, which will frequently present with obvious diagnostic signs and symptoms [clinical synovitis of hand joints, inflammatory findings on ultrasound scan, erosion or other characteristic signs on radiographs, raised C-reactive protein (CRP) levels, and the presence of characteristic antibodies], axSpA can be more difficult to recognize, especially in the early phase of the disease. In fact, the clinical history of the disease may not always be classic, CRP may be well within the normal range despite active disease, and radiographs are often normal for the first 10 years of disease20; therefore, the involvement of MRI, in particular to identify potentially diagnostic inflammatory lesions, is critical. Clinical rheumatologists are not specifically trained to analyze and interpret MRI scans and are therefore dependent on radiologists to advise on the most appropriate protocols and sequences to perform and to identify and report diagnostic lesions. However, the results of our present survey indicate generally low levels of knowledge and understanding of axSpA among radiologists.
Moreover, recognition of the specific term axSpA was as low as 75% among radiologists. Of even more concern was that only 31% and 25% were aware of “positive,” and in the correct clinical context, “diagnostic” definitions of MRI findings of the SIJ and spine, respectively, for axSpA. These definitions were formulated by a working party composed of radiology and rheumatology experts; however, 18% of radiologists in this survey did not use subchondral bone marrow edema of the SIJ and 18% did not use inflammatory vertebral corner lesions to assist in diagnosis. These findings suggest that published definitions have not yet entered mainstream radiology practice in the United Kingdom. These findings are even more relevant now because recent NICE guidance9 for the use of anti-TNF therapies in nr-axSpA hinge largely on the presence of axial inflammation as noted on MRI. With these guidelines, it is expected in due course that pelvic radiographs will no longer be done as a diagnostic investigation in axSpA. Given the high dose of radiation and poor interobserver reliability, this is a positive step.
This low level of understanding of axSpA among radiologists may exist partially because rheumatology–radiology interdisciplinary meetings are not standard practice, with only two-thirds of radiologists having regular meetings with their rheumatology colleagues. These findings emphasize the need for agreed-upon best-practice guidelines.
One of the main limitations of our study is the low response rate (38%). However, the responding radiologists covered 73% of the hospital trusts and health boards in the United Kingdom, suggesting that the results of our present study are generalizable to current practice among UK radiologists. The other possible limitation is potential bias in the results. Radiologists, unfamiliar with axSpA classification criteria and MRI definitions, could have been less likely to respond to the survey. If that is true, the data emphasize even more the requirement for further collaboration and guidance in this field.
There is diverse practice in the use of MRI and limited knowledge of the features defining a diagnostic MRI for axSpA among radiologists in the United Kingdom, suggesting international guidance has not widely infiltrated national practice. We propose that this gap should be bridged by a joint rheumatology and radiology consensus statement on the use of MRI in the assessment of axSpA to help standardize practices, ensuring prompt and effective patient management in the diagnosis and treatment of axSpA.
ONLINE SUPPLEMENT
Supplementary material accompanies the online version of this article.
Acknowledgment
This is a British Society for Spondyloarthritis (BRITSpA) study. The authors thank pH Associates (Marlow, UK), a company specializing in real-world evaluation, for providing medical writing support in the preparation and revision of this manuscript, with funding provided by AbbVie. Kantar Health (Epsom, UK) performed the survey and data collection.
Footnotes
Supported by AbbVie Ltd., Maidenhead, UK.
- Accepted for publication February 4, 2017.








{kind=link}
{kind=link}