

Abstract
Objective. For patients with rheumatoid arthritis (RA) who have an inadequate response to methotrexate (MTX), the relative effectiveness of the combination of conventional disease-modifying antirheumatic drugs (DMARD) compared with the combination of tumor necrosis factor (TNF) inhibitors and MTX, as second-line therapy, is uncertain. The aim of this study was to compare the efficacy and tolerance of triple oral DMARD therapy versus anti-TNF agents associated with MTX in patients with RA after MTX failure.
Methods. We performed a systematic search of the literature up to November 2015 in MEDLINE, Embase, the Cochrane library, and abstracts from the American College of Rheumatology (ACR) and the European League Against Rheumatism (EULAR) meetings from 2006 to 2015. Articles were included if they were of randomized controlled trials of patients receiving triple oral combination therapy (TT; MTX + sulfasalazine + hydroxychloroquine) compared with anti-TNF agents plus MTX. Treatment effects were examined by disease activity [Disease Activity Score in 28 joints (DAS28)], ACR and EULAR response criteria, structural damage by the modified total Sharp score, and functional disability by the Health Assessment Questionnaire (HAQ).
Results. Our search identified 263 articles; only 5 fulfilled the selection criteria. Analysis of ACR and EULAR response criteria, DAS28, and modified Sharp scores favored anti-TNF agents combined with MTX. Functional disability (HAQ) and rates of adverse events did not differ between treatments.
Conclusion. In patients with RA in whom MTX has failed, the addition of a TNF antagonist to MTX may be a valid option, with better clinical outcomes and better radiographic results in the presence of poor prognostic factors. In the absence of poor prognostic factors and/or with contraindications to biologic agents, TT retains its place in the therapeutic strategy for RA in a currently restricted economic context.
Rheumatoid arthritis (RA) outcome has greatly improved in recent years because of earlier diagnosis, treatment targeting low disease activity or remission, early use of disease-modifying antirheumatic drugs (DMARD) alone or in combination, and the availability of biologic agents1.
DMARD have long been the cornerstone of RA therapy2,3, and among conventional synthetic DMARD (csDMARD), methotrexate (MTX) has emerged as the preferred first-line agent4,5. However, only 30% of patients will have low disease activity with MTX alone6,7,8,9. Patients with an incomplete or no response to MTX often require tumor necrosis factor (TNF) antagonists, although combining csDMARD could be a reasonable alternative.
Individual randomized controlled trials (RCT) and systematic reviews of RCT suggested that combination therapies were more effective than DMARD monotherapy in RA7,10,11,12,13,14. However, the relative effectiveness of combinations of csDMARD and MTX compared with combinations of TNF inhibitors and MTX is uncertain. The direct cost of treating RA has also increased, largely because of the increased use of biologic agents. For patients without an adequate response to MTX, an important question is whether the addition of an anti-TNF agent to MTX will provide better clinical and structural efficacy than the addition of other csDMARD.
We systematically reviewed RCT results of the efficacy and tolerance of csDMARD [sulfasalazine (SSZ) and hydroxychloroquine (HCQ)] with MTX versus TNF inhibitors with MTX in patients with RA.
MATERIALS AND METHODS
Our systematic literature review involved a search for articles published up to November 2015 in the MEDLINE, Embase, and Cochrane databases, as well as abstracts from the American College of Rheumatology (ACR) and European League Against Rheumatism (EULAR) annual meetings (2013 to 2015) by 2 independent investigators. The key words were “rheumatoid arthritis,” “methotrexate,” “hydroxychloroquine,” “sulfasalazine,” and “clinical trial.” We also manually searched references lists of articles. The selected studies had to be clinical RCT, and patients included had to meet the ACR criteria for the diagnosis of RA. The first arm included patients receiving a triple oral combination therapy (TT) of csDMARD (MTX, SSZ, and HCQ). The comparator arm included patients receiving an anti-TNF-α agent combined with MTX. The outcomes were the EULAR and ACR response criteria, change in Disease Activity Score in 28 joints (DAS28) score, radiographic progression assessed by the van der Heijde-modified total Sharp score (modified Sharp score), and evolution of functional disability by the Health Assessment Questionnaire (HAQ). Timepoints for outcome assessment were 6 months [Comparative Active Therapies (RACAT) study], from weeks 48 to 102 [Treatment of Early Rheumatoid Arthritis (TEAR) trial], 12 and 24 months [Swedish Farmacotherapy (SWEFOT) studies], and 4 months [Induction therapy with MTX and Prednisone in Rheumatoid Or Very Early arthritic Disease (IMPROVED) study] after randomization. The methodological quality of included trials was independently assessed using the Cochrane Collaboration’s tool for assessing risk of bias. Studies were graded as having a “low risk,” “high risk,” or “unclear risk” of bias across the 7 specified domains15 (Supplementary Table 1, available from the authors on request). Ethical approval for our study was not required.
RESULTS
Literature search
The preliminary search identified 262 items. Manual search revealed an additional article. After a reading of titles and abstracts, we considered 11 studies potentially relevant. Finally, only 5 articles (4 trials) that met our objectives were used for the review (Figure 1). Figure 26,16,17,18 and Table 16,8,16,17,18 summarize the study design and characteristics of included studies.

Flow diagram of study identification and selection. RA: rheumatoid arthritis; TT: triple oral combination therapy; TNF: tumor necrosis factor; MTX: methotrexate; IFX: infliximab; DMARD: disease-modifying antirheumatic drugs.

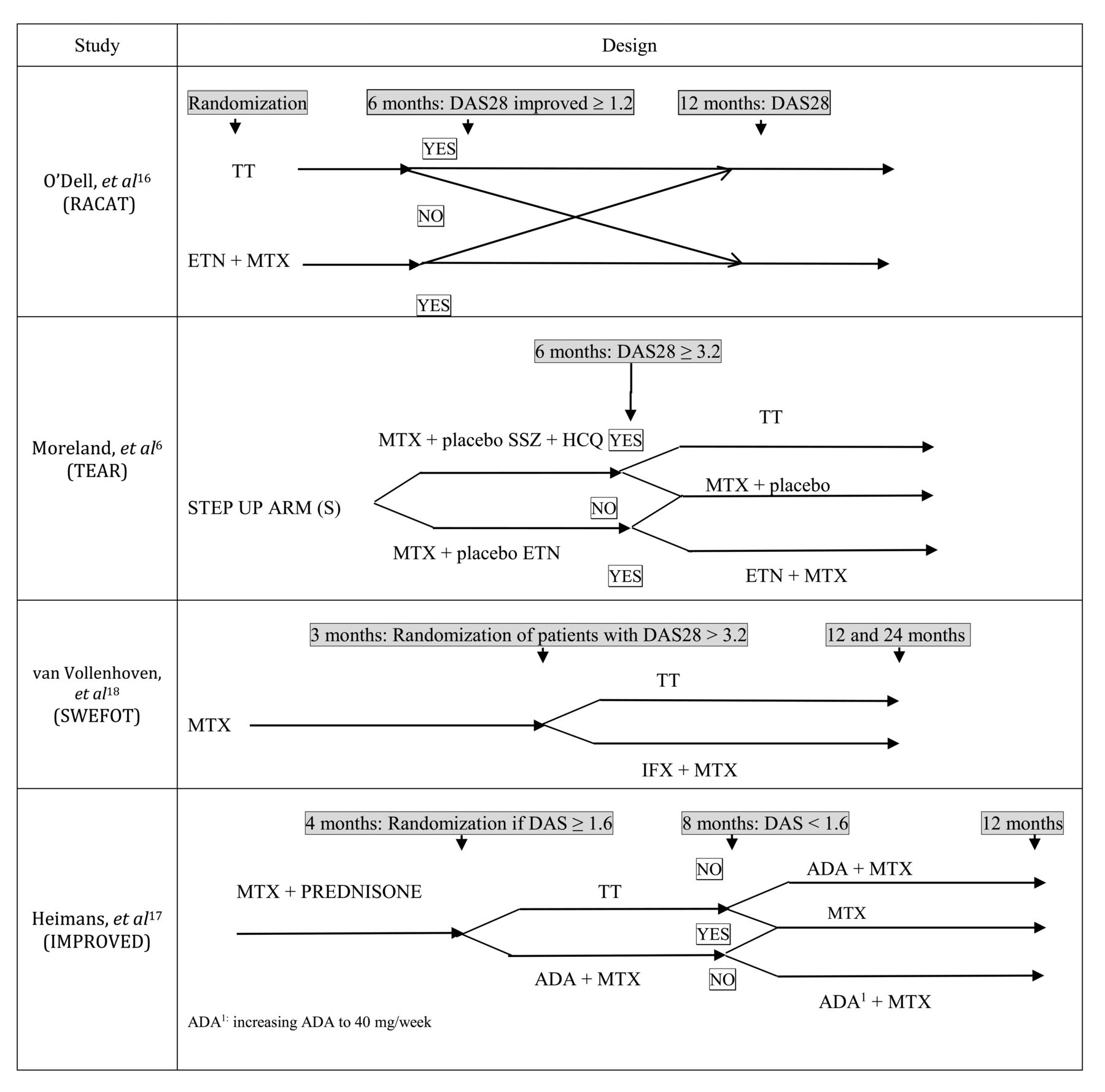
Design of studies included in the systematic review. ADA1: Increasing ADA to 40 mg/week. RACAT: Comparative Active Therapies; TEAR: Treatment of Early Rheumatoid Arthritis; SWEFOT: Swedish Farmacotherapy; IMPROVED: Induction therapy with MTX and Prednisone in Rheumatoid Or Very Early arthritic Disease; DAS28: Disease Activity Score in 28 joints; TT: triple oral combination therapy; ETN: etanercept; MTX: methotrexate; SSZ: sulfasalazine; HCQ: hydroxychloroquine; IFX: infliximab; ADA: adalimumab.
Characteristics of included randomized controlled trials.
Patient characteristics
Within each trial, baseline characteristics of patients did not differ between the 2 treatment arms (Table 2). The study by O’Dell, et al16 had a male predominance, with 56.7% men in the TT arm and 51.4% in the etanercept (ETN)–MTX arm. All included studies analyzed patients with recent RA of < 1-year duration, with the exception of the study by O’Dell, et al16 (mean 5.5 ± 9.3 yrs of disease evolution in the TT arm and 4.9 ± 8.0 yrs in the biotherapy arm).
Baseline characteristics of participants. For readability, the SD are not specified. Within each study, patient characteristics at baseline did not differ between the 2 treatment groups. There were differences between cohorts: the RACAT cohort included older men with RA and a higher percentage of seropositive patients with RA in the TEAR cohort.
Treatments and regimens
Treatments corresponded to the usually recommended dose. Only the study of Heimans, et al17 used a high dose of prednisone (60 mg/day) with progressive decrease within 7 weeks to a stable dose of 7.5 mg/day.
ACR20, 50, and 70 responses (Table 3)
ACR response criteria.
At Week 24, O’Dell, et al16 found ACR70 response more frequent in the ETN–MTX than TT arm (16% vs 5%, p = 0.001).
At Week 48, in the van Vollenhoven, et al8 study, ACR20 response was more frequent in the infliximab (IFX)–MTX than TT arm (42% vs 28%, p = 0.03), as was ACR50 (25% vs 15%, p = 0.04).
At 2 years, van Vollenhoven, et al18 did not find a significant advantage in ACR20, 50, or 70 responses in favor of IFX–MTX, but it was a secondary endpoint and the trial may have been underpowered. Moreland, et al6 showed a significant difference in favor of the anti-TNF than TT group for ACR70 response (p = 0.01).
Good or moderate response according to the EULAR criteria
Only van Vollenhoven, et al8,18 in the SWEFOT trial used the EULAR response criteria, which was the primary endpoint at 1 year (Supplementary Table 2, available from the authors on request). At Year 1, 25% of patients in the TT arm and 39% in the IFX–MTX arm achieved a good EULAR response, with significant difference (p = 0.016). In Year 2, the authors did not find any significant difference between the groups.
DAS28 score
In the RACAT trial16, the 2 treatment arms conferred a significant improvement in DAS28 at Week 24 compared with baseline (p = 0.0001). DAS28 change at 24 weeks did not differ between the 2 groups. In contrast, achieving a low disease activity state was more frequent in the anti-TNF than TT arm (34.8% vs 24.8%, p = 0.05; Supplementary Table 3, available from the authors on request). Similarly, significantly more patients in the ETN–MTX group were in clinical remission (DAS28 < 2.6) than in the conventional therapy group (21.7% vs 12.7%, p = 0.03). In the TEAR trial6, DAS28 remission between weeks 48 and 102 was achieved by 56.6% of patients in the initial biological therapy arm versus 59.1% in the TT arm, with no significant difference, but only the completers were reported. In the IMPROVED study17, 36% of patients receiving TT and prednisone (7.5 mg/day) and 35% of patients receiving adalimumab (ADA)–MTX achieved DAS remission at 4 months after randomization, with no significant difference between treatments. However, patients not in remission at 4 months had a treatment optimization with ADA–MTX in arm 1 and increased ADA dose in arm 2; at 8 months after randomization, the rate of remission was significantly higher in the initial ADA–MTX group versus the TT and prednisone group (41% vs 25%).
Structural damage
In the RACAT study16, the treatment groups did not differ in structural damage at Week 24. The mean increase in modified Sharp score was 0.42 for the TT arm and 0.003 units for the ETN–MTX arm (p = 0.2; Table 4). In the study by Moreland, et al6, the modified Sharp score differed between the ETN–MTX and TT groups. In the SWEFOT study18, both groups showed radiographic progression at 12 and 24 months compared with baseline. The increase in modified Sharp score was greater for the TT than IFX–MTX group (difference 3.23 points, 95% CI 0.14–6.32, p = 0.009) at 2 years. In the study by Heimans, et al17, the progression in median Sharp score was 0 in both groups.
Radiographic progression in 4 trials.
HAQ functional score
In the RACAT study16, the HAQ II score19 improved from Week 24 in both groups: mean decrease of −0.44 ± 0.77 points in the TT arm and −0.51 ± 0.84 in the ETN–MTX arm, with no significant difference between the 2 arms (p = 0.46). Similarly, in the TEAR study6, the modified HAQ score20 decreased in both treatment groups at 2 years with no significant difference between groups (Supplementary Table 4, available from the authors on request).
Safety
Adverse reactions were equally distributed between the 2 treatment groups, with no noticeable significant differences in all studies. Observed side effects were also consistent with the usual side effects described with these drugs in clinical trials and known therapeutic use. Nevertheless, hematological adverse reactions and gastrointestinal side effects were more frequent in patients in the TT group, and infections and skin/allergic reactions prevailed in the biologic agent group (Supplementary Table 5, available from the authors on request).
DISCUSSION
The results of our systematic literature review suggest a better efficacy of the combination of a TNF inhibitor and MTX versus the combination of synthetic DMARD plus MTX as second-line treatment in patients with RA with inadequate response to MTX monotherapy, both on clinical and structural outcome. TT did not differ from a biologic agent plus MTX in functional improvement or occurrence of adverse effects.
In the RACAT trial16, the primary endpoint was changed during the study to increase the power. In addition, randomization was from 16 veterans’ hospitals with a large percentage of male patients (54%); therefore, the results are difficult to extrapolate to the usual population of patients with RA. Among the 4 retrieved studies, the RACAT trial was the only one including patients with established RA. The mean duration of illness was 4.9 to 5.5 years versus 2.9 to 6.3 months in other studies. Patients without an improvement at 24 weeks (DAS28 decrease by < 1.6) were switched in a blinded fashion to the other arm. This switch affected 27% of patients in the TT group and 26.7% in the ETN–MTX group. In this trial, the 48-week results (primary outcome) evaluated 2 strategies and not 2 treatment arms: TT or ETN–MTX during 24 weeks, then a switch in case of inadequate response. Therefore, we cannot compare the efficacy between TT and biotherapy at 48 weeks and we did not include this 1-year analysis in our analysis.
The study by Moreland, et al6 included a large number of patients lost to followup and only 67.9% of participants completed the 2-year trial. The primary endpoint was minor because it concerned only the change in DAS28 from weeks 48 to 102. Analyses of the primary endpoint, functional disability, and radiographic progression were performed only for “completers.” The intent-to-treat method may be in doubt even if additional analyses with several different approaches for missing data showed no difference in results. In addition, the primary outcome measure was changed during the study. This change was not reported in the article, but was available at ClinicalTrials.gov. Finally, 32.1% of patients withdrew from the trial and did not seem to be analyzed for the primary evaluation.
In the van Vollenhoven, et al study8,18, the main bias was that it was an open-label study that may have been under-powered.
In the IMPROVED study17, patients with undifferentiated arthritis were included and represented 20% of the sample. At 4 months after randomization, the 2 arms did not differ in outcome. However, evaluation of clinical remission after only 4 months of therapy is rather early. Indeed, the time of action of these molecules is variable (between 2 weeks and up to 6 mos)21. By contrast, the analyses of the other studies’ results were made at 6 and 12 months. Further, the 4-month results are difficult to interpret with the combination with low-dose prednisone (7.5 mg/day). Patients not in remission at 4 months had treatment optimization with ADA–MTX in arm 1 and increased ADA dose in arm 2; at 8 months after randomization, the rate of remission was significantly higher in the initial ADA–MTX group (41%) versus the TT and prednisone group (25%). Therefore, the initial ADA–MTX strategy provided a better remission rate.
Moreover, the IMPROVED study included patients with relatively low disease activity compared with patients in the other studies (Table 2). It is also possible that some patients with undifferentiated arthritis or even classified as RA might have had a self-limiting type of arthritis. This might suggest that in the absence of poor prognostic factors, change to another csDMARD strategy should be considered5.
A recent systematic review and network metaanalysis compared MTX and all currently used combinations of DMARD with MTX22. It did not find any statistical benefit for MTX plus biologic therapy compared with triple therapy. The conclusion is not in agreement with our results for several reasons. First, of the 158 included trials, only 4 trials compared MTX plus biologic therapy against MTX plus csDMARD. The study of one of these 4 trials compared leflunomide versus TNF-α inhibitors. The IMPROVED study was not included in these 4 trials. Second, the quality of the evidence for triple therapy was judged to be moderate with some inconsistencies existing in the findings of the 2 trials that compared triple therapy with MTX plus ETN.
The heterogeneity of the results and the large number of patients lost to followup were severe limitations for our preliminary network metaanalysis and consequently may have provided questionable results. Therefore, we present only the results of the systematic review. The other limitation is the link to many methodological biases in many of these trials that were already mentioned in previous reports23.
Insufficient response to MTX has been defined subjectively in these studies and that may explain some variance in trial results. However, the overarching principles used considered patients responding insufficiently to MTX if there was no improvement by at most 3 months after treatment start or the target had not been reached by 6 months.
The TT is less costly than treatment with biologic agents. Biologic agents, because of their high efficiency, can lead to reduced medium- and longterm costs, for example, through reduced absenteeism because of illness and surgical procedures24,25. Effective treatment has positive effects on maintaining employment and reducing absences because of illness26. The 2013 EULAR recommendations5 did not take into account the cost of RA treatment, and in a restricted economy TT retains its place as second-line treatment in the therapeutic strategy for RA in the absence of poor prognostic factors.
Finally, TT per se has some additional limitations, with a higher rate of treatment noncompliance and poor maintenance of drugs27,28. In addition, its superiority compared with monotherapy as first-line treatment has not been clearly established29,30.
The results of this systematic review support the 2013 EULAR recommendations for RA5, which considered that biologic DMARD is the treatment of choice in cases of inadequate response to MTX and in the presence of poor prognostic factors. In the absence of poor prognostic factors and/or with contraindications to biologic agents, TT retains its place in the therapeutic strategy for RA in a currently restricted economic context.
Acknowledgment
We thank Abbvie for its contributions.
- Accepted for publication February 17, 2017.








{kind=link}
{kind=link}