

Abstract
Objective. To assess trends in cardiovascular (CV) mortality in patients with incident rheumatoid arthritis (RA) in 2000–07 versus the previous decades, compared with non-RA subjects.
Methods. The study population consisted of Olmsted County, Minnesota, USA residents with incident RA (age ≥ 18 yrs, 1987 American College of Rheumatology criteria was met in 1980–2007) and non-RA subjects from the same underlying population with similar age, sex, and calendar year of index. All subjects were followed until death, migration, or December 31, 2014. Followup was truncated for comparability. Aalen-Johansen methods were used to estimate CV mortality rates, adjusting for competing risk of other causes. Cox proportional hazards models were used to compare CV mortality by decade.
Results. The study included 813 patients with RA and 813 non-RA subjects (mean age 55.9 yrs; 68% women for both groups). Patients with incident RA in 2000–07 had markedly lower 10-year overall CV mortality (2.7%, 95% CI 0.6–4.9%) and coronary heart disease (CHD) mortality (1.1%, 95% CI 0.0–2.7%) than patients diagnosed in 1990–99 (7.1%, 95% CI 3.9–10.1% and 4.5%, 95% CI 1.9–7.1%, respectively; HR for overall CV death: 0.43, 95% CI 0.19–0.94; CHD death: HR 0.21, 95% CI 0.05–0.95). This improvement in CV mortality persisted after accounting for CV risk factors. Ten-year overall CV mortality and CHD mortality in 2000–07 RA incidence cohort was similar to non-RA subjects (p = 0.95 and p = 0.79, respectively).
Conclusion. Our findings suggest significantly improved overall CV mortality, particularly CHD mortality, in patients with RA in recent years. Further studies are needed to examine the reasons for this improvement.
Rheumatoid arthritis (RA) is associated with increased cardiovascular (CV) morbidity and mortality compared with the general population1,2,3,4,5. CV death has been recognized as a leading cause of premature mortality in RA, accounting for about 40%–50% of all deaths, and is an important contributor to a mortality gap between RA and the general population6,7,8. Metaanalyses estimated a 50%–60% increase in the risk of CV death in patients with RA versus the general population, with lack of evidence for decrease in CV mortality up to the mid-2000s1,9. More recently published studies, including cohorts from the United Kingdom and the Netherlands, suggest a potentially improving trend in CV mortality in patients with RA onset in the 2000s10,11. No excess relative CV mortality in patients with recent-onset RA versus the general population was reported in a nationwide study from Finland12. However, large longitudinal studies comparing CV mortality trends in successive incidence cohorts of patients with RA are lacking, and trends in the relative excess CV mortality in RA versus the general population in the era of advanced therapeutics and intensive treatment strategies are not fully understood.
In our study, we aimed to assess CV mortality following RA onset in patients with incident RA in 2000–07 versus the previous decades, compared with non-RA subjects.
MATERIALS AND METHODS
The study consisted of a population-based inception cohort of Olmsted County, Minnesota, USA residents aged ≥ 18 years [1987 American College of Rheumatology (ACR) criteria for RA met between January 1, 1980, and December 31, 2007]. Patient ascertainment was performed using the Rochester Epidemiology Project, a population-based medical records linkage system with access to the complete (inpatient and outpatient) medical records from all medical providers in the community13,14,15,16. For each patient, RA incidence date was defined as the earliest date of fulfillment of ≥ 4 1987 ACR criteria for RA. Comparison cohort included Olmsted County residents without RA chosen by random selection of a subject of similar age, sex, and calendar year of index for each patient with RA. Each non-RA subject was assigned an index date corresponding to the incidence date of a patient with RA.
All study subjects were followed through medical record review until death, migration, or December 31, 2014. Followup of each cohort was truncated to make the length of followup comparable (i.e., the 1980–89 cohorts were truncated at December 31, 1994 and the 1990–99 cohorts were truncated at December 31, 2004). A review of medical records was performed by trained nurse abstractors to record the following CV risk factors: age, smoking, hypertension (HTN), diabetes mellitus (DM), and dyslipidemia. HTN was defined according to the criteria of the Joint National Committee on Detection, Evaluation, and Treatment of High Blood Pressure as ≥ 2 ambulatory blood pressure readings ≥ 140 mmHg systolic and/or ≥ 90 mmHg diastolic during a 1-year period, physician diagnosis, or documented use of antihypertensives17. Dyslipidemia was defined based on the Adult Treatment Panel III guidelines18 as total cholesterol ≥ 240 mg/dl, low-density cholesterol ≥ 160 mg/dl, triglycerides ≥ 200 mg/dl or high-density cholesterol < 40 mg/dl, physician diagnosis, or documented use of lipid-lowering medications. DM was defined as fasting plasma glucose ≥ 126 mg/dl, physician diagnosis, or documented use of insulin and/or oral hypoglycemic agents based on the diagnostic criteria adopted by the American Diabetes Association19,20. Data on RA disease characteristics such as rheumatoid factor (RF) positivity, erythrocyte sedimentation rate (ESR), joint erosions/destructive changes on radiographs, and severe extraarticular manifestations of RA including pericarditis, pleuritis, Felty syndrome, glomerulonephritis, cutaneous vasculitis, peripheral neuropathy, scleritis, episcleritis, or retinal vasculitis21 were collected for all patients. Information on antirheumatic medication use, including systemic glucocorticoids, disease-modifying antirheumatic drugs [DMARD; i.e., methotrexate (MTX), hydroxychloroquine (HCQ), other DMARD], biologics (tumor necrosis factor inhibitors, anakinra, abatacept, rituximab), nonsteroidal antiinflammatory drugs (NSAID), and cyclooxygenase (COX)-2 inhibitors, was also gathered during the first year of RA incidence and ever during the followup.
Underlying causes of death were obtained from state and local death certificates and the National Death Index Plus, and grouped according to the International Classification of Diseases (ICD)-Clinical Modification. The ICD, 9th ed (ICD-9) was used for deaths in 1980–1998, and the ICD-10 was used thereafter. All causes of CV death were classified according to the American Heart Association (AHA) classification, with mutually exclusive sets of codes for coronary heart disease (CHD), non-CHD, and noncardiac circulatory causes22. The following ICD codes were used for CHD causes including myocardial infarction, revascularization procedures, CV death, and angina: ICD-9 410–414, and ICD-10: I20–I25; non-CHD diseases of the heart including acute rheumatic fever, chronic rheumatic heart disease, hypertensive heart disease, pulmonary circulatory disease, and other forms of heart disease: ICD-9: 390–398, 402, 404, 405, 415–429, and ICD-10: I00–I09, I11, I13, I26–I51; and noncardiac circulatory causes including cerebrovascular diseases; other hypertensive diseases (not included elsewhere); diseases of arteries, arterioles, and capillaries; diseases of veins, lymphatic vessels, and lymph nodes; other and unspecified disorders of the circulatory system: ICD-9: 401, 403, 430–459 and ICD-10: I10, I12, I15, I52–I99. This study was approved by institutional review boards (IRB) of the Mayo Clinic (IRB #675-99) and the Olmsted Medical Center (IRB #018-omc-06).
Statistical methods
Comparisons of characteristics between cohorts were made with the chi-square and rank-sum tests. The Aalen-Johansen method was used to estimate CV mortality rates adjusted for the competing risk of death from other causes23. Cox proportional hazards models, adjusting for age and sex and other characteristics, were used to compare CV mortality by decade. Analyses were performed using SAS version 9.4 (SAS Institute) and R 3.1.1 (R Foundation for Statistical Computing).
RESULTS
The study included 813 patients with RA (a total of 10,560 person-yrs of followup), of whom 315 developed incident RA during 2000–07, 296 during 1990–99, and 202 during 1980–89. Table 1 shows characteristics of patients with RA overall and by decade of incidence. Patients with RA onset in different decades were similar with respect to demographics and RF-positivity. The percentage of current smokers, the highest ESR in the first year of RA, and the use of other DMARD declined while obesity, hyperlipidemia, and the use of lipid-lowering medications, MTX, HCQ, biologics, glucocorticoids, and NSAID increased in patients with more recent RA onset compared with earlier decades (Table 1). The percentage of patients with erosions in different decades of RA onset remained unchanged (p = 0.26). The delay between first documentation of RA symptoms (i.e., swollen joints) and fulfillment of RA classification criteria has not changed over time (p = 0.54), but the time from fulfillment of criteria to initiation of the first DMARD has decreased in recent years (p < 0.001).
Characteristics of study subjects. Significant differences between the RA and non-RA cohorts overall included smoking status (p = 0.002) and hyperlipidemia (p = 0.01). Significant differences between decades among the RA cohorts included smoking status, obesity, hyperlipidemia, use of lipid-lowering medications, ESR, time from RA incidence to initiation of the first DMARD, use in the first year and ever use of methotrexate, hydroxychloroquine, other DMARD, biologics, glucocorticoids, NSAID, and COX-2 inhibitors (all p < 0.001). Significant differences between decades among the non-RA cohorts included smoking status (p = 0.008), obesity (p < 0.001), hyperlipidemia (p < 0.001), use of lipid-lowering medications (p < 0.001), hypertension (p = 0.024), use of antihypertensives (p = 0.009), and NSAID (p = 0.003). Values are n (%) unless otherwise specified.
The comparison population consisted of 813 non-RA subjects (a total of 11,468 person-yrs of followup), including 315 non-RA subjects with index date in 2000–07, 296 with index date in 1990–99, and 202 subjects with index date in 1980–89 (Table 1). Apart from higher rates of smoking and hyperlipidemia in subjects with RA, there were no statistically significant differences in demographics and CV risk factors between RA and non-RA subjects overall or by decade of incidence/index. The use of NSAID and COX-2 inhibitors during the first year of RA onset and at any point during the followup was higher in patients with RA versus non-RA subjects.
Figure 1 shows trends in CV mortality overall, CHD mortality, and non-CHD mortality in patients with RA by decade of RA incidence. Mortality estimates for patients with RA by decade of incidence are shown in Table 2. During the median followup of 9.0 years, 8 patients in the 2000–07 cohort died from CV disease (CVD), including 2 deaths from CHD (unadjusted 10-yr overall CV mortality estimate 2.7%, 95% CI 0.6–4.8%; CHD mortality 1.1%, 95% CI 0.0–2.7%), suggesting significant improvement in CV mortality after RA onset in 2000–07 versus those with RA onset in 1990–99. After adjustment for age and sex, results remained similar to unadjusted results (Table 2). Table 3 shows the HR for CV mortality in patients with RA onset in different decades. HR for overall CV death in 2000–07 cohort versus 1990–99 cohort was 0.42 (95% CI 0.18–0.95), and for CHD death 0.17 (95% CI 0.04–0.75). Additional adjustment for smoking status, obesity, HTN, and hyperlipidemia did not alter these results (HR for CV death: 0.42, 95% CI 0.18–0.99; HR for CHD death: 0.14, 95% CI 0.03–0.67). In turn, patients in the 1990–99 cohort showed a decrease in overall CV mortality and CHD mortality after RA onset versus those in the 1980–89 cohort (p = 0.003 and p = 0.09, respectively; Table 3). There was no evidence that time trends in overall CV mortality and CHD mortality after RA onset in any of the RA incidence cohorts differed by RF status (interaction p = 0.30 and p = 0.59, respectively) or by sex (interaction p = 0.41 and p = 0.77, respectively).

CV mortality in patients with RA with incidence date in 1980–89 (solid line), 1990–99 (dashed line), and 2000–07 (dotted line). (A) All-cause CV mortality. (B) CHD mortality. (C) Non-CHD mortality. CV: cardiovascular; RA: rheumatoid arthritis; CHD: coronary heart disease.
CV mortality in patients with RA and subjects without RA by decade of incidence/index year. Values are mean ± SD unless otherwise specified.
Relative declines in CV mortality in patients with rheumatoid arthritis by decade of incidence.
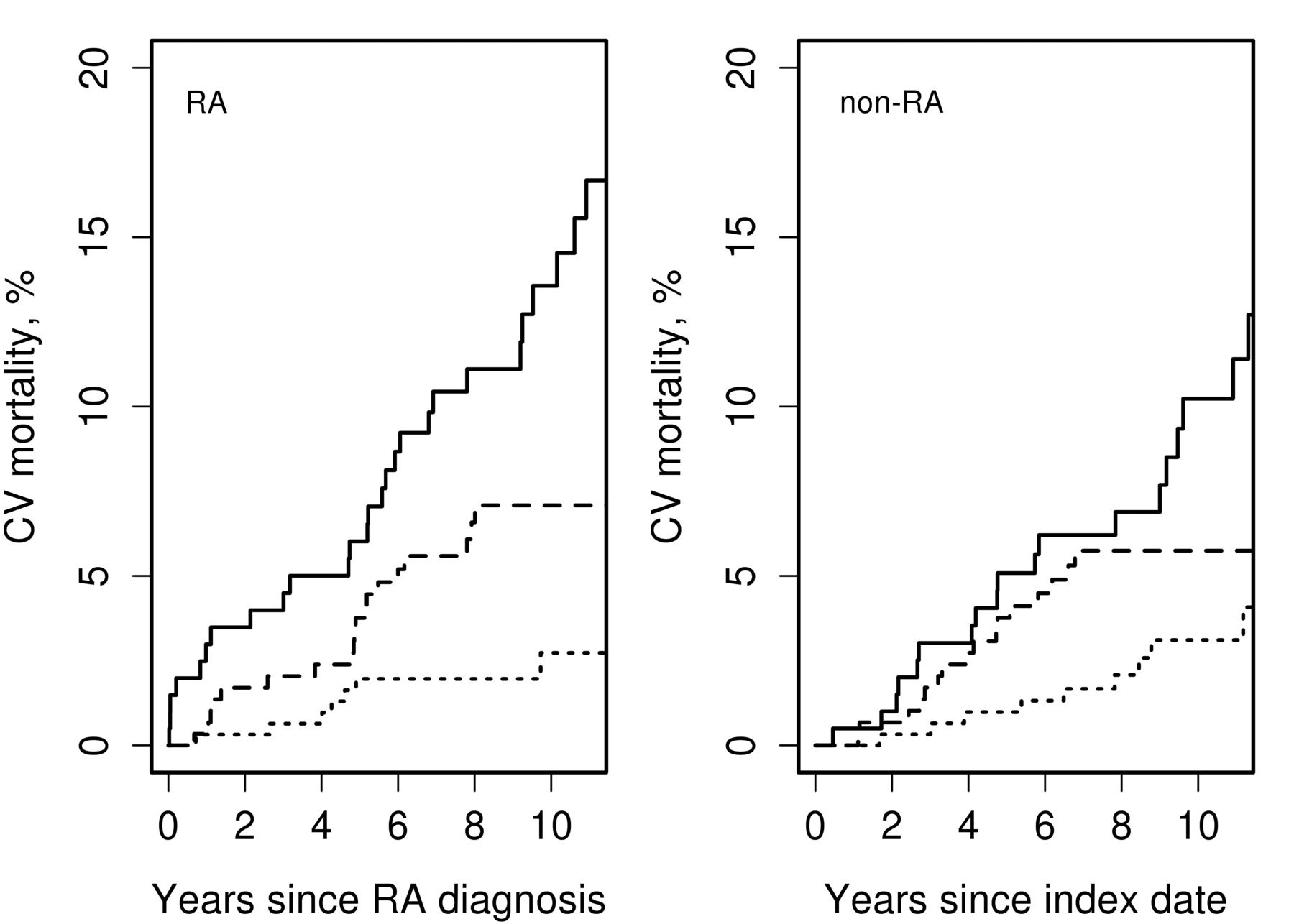
Figure 2 shows CV mortality in subjects with and without RA by decade of RA incidence/index, and Table 2 summarizes these data. There has been no statistically significant difference in overall CV mortality following RA incidence/index date in RA versus non-RA subjects in the 2000–07 cohort (p = 0.95) and the 1990–99 cohort (p = 0.59); in the 1980–89 cohort the difference in overall CV mortality in RA versus non-RA subjects was borderline significant (p = 0.06). CHD mortality following RA incidence/index date was similar in RA and non-RA subjects in the 2000–07 (p = 0.79), 1990–99 (p = 0.27), and 1980–89 cohorts (p = 0.13). After adjustment for age and sex, results remained similar to unadjusted results (Table 2).

CV mortality in subjects with and without RA by decade of RA incidence/index: 1980–89 (solid line), 1990–99 (dashed line), and 2000–07 (dotted line). CV: cardiovascular; RA: rheumatoid arthritis.
There was no significant improvement in non-CHD deaths in patients with RA (p = 0.22; Figure 1, Table 2) or in the non-RA subjects (p = 0.23; Table 2) with RA incidence/index date in different decades. Mortality from noncardiac circulatory causes in RA improved in the 1990–99 cohort compared with the 1980–89 cohort (p = 0.013), but was similar between the 1990–99 and 2000–07 cohorts (p = 0.43). Decline in mortality because of noncardiac circulatory causes in non-RA subjects did not reach statistical significance (p = 0.07). There was no evidence that the trend in mortality because of noncardiac circulatory causes differed between those with and without RA (interaction p = 0.20).
DISCUSSION
The literature on increased CV morbidity and mortality in RA is mounting, but the recent trends in CV mortality following RA onset and the changes in relative mortality in RA versus the general population are not well understood. To our knowledge, our study is one of the first to show a marked decline in overall CV mortality and CHD mortality in patients who developed RA in recent years versus those with RA onset in prior decades.
Few studies have reported recent trends in CV mortality to date10,11,24. A declining trend in overall CV mortality has been suggested in patients with early inflammatory arthritis enrolled in the Norfolk Arthritis Register in 2000–04 versus 1990–94 and censored after the 7-year followup10. Mortality declined nonsignificantly from 8.78/1000 person-years in patients enrolled in 1990–94 to 7.07/1000 person-years in those enrolled in 2000–04, which was similar to the decline in CV mortality in the general population. Lower CV mortality rates in recent years were suggested in a prospective study from a Dutch population comparing CV mortality among patients with RA enrolled in 2009–11 with CV mortality estimates reported in literature for various populations worldwide during the previous decades11.
Extending these findings, our study has shown a statistically significant 58% decline in CV mortality and a dramatic 83% decline in CHD-related mortality in patients with RA onset in 2000–07 versus 1990–99. Although the improvement was most apparent in the 2000–07 cohort, patients in the 1990–99 cohort have also demonstrated a statistically significant improvement in CV mortality compared with the 1980–89 cohort. This improvement in CV mortality was observed in both men and women, regardless of RF positivity, and persisted after accounting for age and traditional CV risk factors.
The reasons for this apparent improvement in CV mortality in RA are not clear. Biologics have been suggested as an important contributor to reduced CV event rates in prior studies and could be contributing to improved CV mortality in our 2000–07 cohort25,26,27. However, CV mortality improvement in the 1990–99 cohort, i.e., before the widespread use of biologics, suggests alternative explanations for the improving mortality. These include increasing use of DMARD as shown in our study, early initiation of antirheumatic treatments and associated improvement in inflammation control as suggested by a decline in highest ESR in the first year of RA onset in our study, and a decline in the rate of flares with concomitant increase in remission rates in RA over the past 2 decades as we showed in this cohort28. Delay in RA diagnosis has been associated with increased rate of CV events29. In our study, time from first documentation of swollen joints to fulfillment of RA classification criteria did not change over time, suggesting that other causes as presented in this discussion may have contributed to the changes in CV mortality in RA.
There is also growing evidence about the CV benefits of traditional DMARD, primarily MTX12,30,31,32,33,34,35, with favorable implications for CV risk and life longevity with DMARD use and adherence to treat-to-target strategy36,37. Increase in glucocorticoid use in the 1990–99 and 2000–07 RA cohort versus the 1980–89 cohort in our study echoes the dynamics in glucocorticoid use described in previous studies from our group38 and others39. This increase in usage could result from changes in practice guidelines. The 2013 European League Against Rheumatism update on treatment recommendations of RA recommends the addition of low-dose glucocorticoids as part of the initial treatment strategy for up to 6 months and tapering as soon as clinically feasible40. Positive dose-response association has been found between glucocorticoid use and CV mortality in RA41. However, our prior studies in this cohort showed that cumulative glucocorticoid dose, at least in the first year of RA diagnosis, has not changed significantly over time36, suggesting no increase in adverse effect of glucocorticoid burden on CV mortality in more recent years versus previously.
Our prior studies have suggested declining incidence of CVD in patients with more recent onset RA, which may also contribute to lower CV mortality rates42. Increased awareness of CVD in RA with advanced management strategies according to existing guidelines of CV management in RA43,44 could have improved CV mortality trends in RA. Improvement in CV health management in the overall population likely explains the improving trajectory of CV mortality in the general population, which may have provided a beneficial background for decreasing CV mortality in RA as well. In combination with improved inflammation control and CVD management in RA, this improvement could at least in part explain the somewhat more rapid decline in CV mortality in RA than in the general population.
Indeed, our study suggests that CV mortality trends were largely similar in RA versus non-RA cohort with RA incidence/index date in 1990–99 and 2000–07. However, subjects with RA incidence in 1980–89 had somewhat higher CV mortality rates than non-RA subjects. These findings echoed a study by Humphreys, et al in which CV mortality in patients with early inflammatory arthritis enrolled in the study after 1990 was similar to that in the general population10. Concordantly, Kerola, et al reported no excess CV mortality in patients with recent onset RA in 2000–07 versus the general population of Finland12. Likewise, Lacaille, et al have reported that 5-year CV mortality in patients with RA onset in 2001–06 was similar to that of non-RA subjects24. Unlike improved CV mortality in incident RA cohorts, no improvement in CV mortality in patients with established RA was detected between 1997 and 201245.
While there appears to be a general tendency toward improved CV outcomes in RA, some populations of patients with RA (including our RA cohort) appear to have had somewhat more pronounced improvements in CV mortality than others. Differences in data collection and case ascertainment as well as different healthcare practices in various populations worldwide may perhaps account for some of these differences. Ready access to healthcare among Olmsted County residents with only a few major healthcare providers and unified healthcare practices may have contributed to the somewhat more pronounced improvements in CV mortality in the patients with RA in our cohort. More studies are needed to understand whether there are other reasons for these heterogeneous trends in CV outcomes and to elucidate major determinants facilitating and precluding the improvement in CV morbidity and mortality in various populations of patients with RA worldwide.
Our study has several important strengths. It is a large population-based study using a comprehensive medical record linkage system including all inpatient and outpatient care from all local providers. Standardized case ascertainment and inclusion of successive incidence cohorts strengthen the study. Our study also takes advantage of the long and complete followup of all subjects and the availability of a non-RA comparison cohort from the same underlying population. Use of uniform classification of CV deaths per AHA guidelines and standardized coding based on the ICD-9 and ICD-10 also strengthens the study.
There are some potential limitations to our study. There is a potential for miscoding of the underlying causes of death. However, this would affect all subjects in the study and thus is unlikely to significantly bias the comparisons. In addition, the coding of cause of death has changed from ICD-9 to ICD-10 in 1999 because of a change in the classification system. This change could influence comparisons of cause of death in the more recent cohorts (1990–99 cohort, which is followed until December 31, 2004, and the 2000–07 cohort, which is followed until December 31, 2014) versus the earlier cohort. These system-based changes are impossible to account for in statistical analyses; however, the fact that the change affected both the 1990–99 and 2000–07 cohorts potentially minimized the shortcoming regarding comparisons between the 2 cohorts.
The followup of the study was limited and the number of CV deaths, particularly deaths from CHD, was small, which may limit statistical power. While we could show statistically significant differences in mortality despite the low numbers, examination of this issue in larger studies with longer followup and higher number of deaths is encouraged. Because of the availability of nonprescription over-the-counter medications, the data on NSAID/COX-2 inhibitors provided in our study may underestimate the true use of these medications and should be interpreted with caution. Finally, during the period of investigation, the population of Olmsted County, Minnesota, was predominantly white. Thus, the results may not be generalizable to nonwhite individuals.
Our findings suggest a significant decline in overall CV mortality, particularly CHD mortality, among patients with incident RA in 2000–07 compared with patients with incident RA in the previous decades. This more recent improvement in CV mortality in RA is perhaps somewhat more rapid than in the general population. While the reasons for the recent improvement in CV mortality in RA are uncertain, beneficial general population trends in CV health may be contributing, as may RA disease–specific factors including early effective antirheumatic treatment and increased awareness of the need for regular CV screening and management of patients with RA as a high CV risk group. Further studies are under way to understand the reasons for this recent improvement in CV mortality in RA, which may provide clues to better CV management in both RA and the general population where benefits of inflammation control may also apply.
Initial findings of our study were presented at the ACR 2015 meeting46.
Footnotes
Funded by a grant from the US National Institutes of Health (NIH), National Institute of Arthritis and Musculoskeletal and Skin Diseases (R01 AR46849). Research reported in this publication was supported by the US National Institute on Aging of the NIH under award number R01AG034676.
- Accepted for publication February 17, 2017.








{kind=link}
{kind=link}