

Abstract
Objective. Enthesitis is the spondyloarthritis (SpA) landmark, but can also be seen after entheses overuse, such as during intensive sport.
Methods. We aimed to compare entheses ultrasound (US) findings in a prospective cross-sectional study of 30 axial SpA cases, 30 athletes, and 29 controls.
Results. Mean (SD) MAdrid Sonographic Enthesis Index (MASEI) score was 26.3 (13), 12.2 (7), and 10.4 (6) in patients with SpA, athletes, and non-athlete control groups, respectively (p < 0.0001).
Conclusion. The MASEI score was significantly higher in patients with SpA compared with healthy controls, athletes, and non-athletes, and can be of value to distinguish SpA from healthy subjects, whatever their physical activity.
Spondyloarthritis (SpA) is characterized by inflammatory and structural changes in the entheses.
In a cross-sectional study, D’Agostino, et al1 compared ultrasound (US) examination of the major entheses in 164 patients with SpA and 64 control subjects [34 mechanical low back pain and 30 rheumatoid arthritis (RA)]. At least 1 enthesitis was observed in 161 of the 164 patients with SpA (98%) and in 33 of the 64 control patients (52%)1. US enthesitis was most commonly distributed in the distal portion of the lower limbs, irrespective of clinical symptoms.
Similarly, Ruta, et al confirmed the high prevalence of asymptomatic lower-limb enthesitis (almost 60% of subclinical US enthesitis) in 60 patients with SpA compared with patients with RA and healthy subjects2.
However, enthesitis is not only observed in SpA, but can also be seen after entheses overuse, such as during intensive sport.
Several studies have demonstrated that sport can lead to structural changes of the entheses3,4,5,6,7. Enthesis vascularization detected with power Doppler US (PDUS) can also be modified by sport. Boesen, et al observed a significant increase in entheses vascularization as indicated by color Doppler activity in both the Achilles and patella tendons after loading during high-level badminton matches6. Similarly, 634 asymptomatic runners were tested for Achilles tendon thickness, vascularization, and structural abnormalities using a high-resolution PDUS device8. Their mean training volume was 4.0 ± 2.5 h per week. Neovascularization was observed on PDUS in 38%.
The MAdrid Sonographic Enthesis Index (MASEI) is an US score developed by de Miguel, et al for SpA diagnosis and assessment9. A score ≥ 18 performed well in discriminating patients with SpA from healthy controls. The sensitivity, specificity, positive, and negative likelihood ratios (LR+, LR–) were 83.3%, 82.8%, 4.8%, and 0.2%, respectively. This cutoff point was established with an a priori sedentary control group.
Our aim was to compare US findings of entheses among 3 groups: patients with axial SpA (axSpA), athletes, and non-athlete healthy controls, and to assess the discriminant ability of the MASEI score.
MATERIALS AND METHODS
Patients
We conducted a cross-sectional study including 30 patients with axSpA, 30 athletes, and 29 non-athlete healthy controls.
All patients with axSpA fulfilled the 2009 Assessment of Spondyloarthritis international Society (ASAS) criteria10. Athletes were defined as subjects playing a sport resulting in a strain on the lower limbs, such as running or soccer, ≥ 6 h per week. Subjects were recruited among affiliates of a local athletics club. Non-athlete healthy controls had to play a sport < 1 h per week. They were recruited from university students and hospital personnel.
To participate in the study, all healthy subjects, athletes, and non-athletes had to have no musculoskeletal disorder, particularly heel or back pain. A history of surgery and recent corticosteroid infiltration of the heel or the ankle were also noninclusion criteria.
The study was conducted according to the Declaration of Helsinki and French legislation. Before study inclusion, each subject gave informed consent for research use and publication of the results. The local ethics committee CPP Sud Méditerranée I (13-44) approved the study (NCT02038426).
Clinical and biochemical evaluation
Clinical, biological, and imaging evaluations were performed on the same day for patients with SpA and healthy subjects, athletes, and non-athletes.
We collected the following demographic data: age, sex, weight, medical and surgical history, and ongoing treatments (including nonsteroidal anti-inflammatory drugs and oral corticosteroids). As part of the consultation, the clinician (MAL) completed a standardized questionnaire covering the presence or absence of clinical features included in the ASAS classification criteria for SpA, and performed a standardized examination of the heels. Enthesis was defined if the patient reported heel pain during 1 of the following 3 tests: passive stretching, contraction against a resistance exerted by the examiner, and/or Achilles tendon palpation.
Scores on the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) and the Ankylosing Spondylitis Disease Activity Score (ASDAS) were collected for the patients with SpA.
Blood samples were analyzed for HLA-B27 and C-reactive protein (CRP). Levels of CRP > 5 mg/l were considered elevated. A pregnancy urinary test was performed for all women of childbearing age.
Radiographs, an anteroposterior view of the pelvis and 1 oblique view of each sacroiliac joint, were graded using the New York classification scale. We also assessed profile calcaneus radiographs, searching for heel spur.
US evaluation
The physicians who performed the clinical examination and the radiologists performing US scanning were blinded to one another’s results. Patients with SpA and healthy subjects had at least a 15-min rest in the room before US evaluation. US scanning was performed by 3 trained radiologists (OL, AT, CW) using a Toshiba Aplio 500 equipped with linear transducer, frequency of 6–18 MHz. The following enthesis sites included in the MASEI scoring9 were scanned bilaterally, using both greyscale and PD: proximal plantar fascia, distal Achilles tendon, distal and proximal patellar tendon insertion, distal quadriceps tendon, and distal brachial triceps tendon. Each tendon was scanned in both longitudinal and transverse planes, and the scan images were stored. At each site, the following elementary lesions were assessed: bursitis, calcification, erosion, PD, thickening of tendon, and structural change.
Interobserver reliability was assessed by reading 20 images of the study subjects, randomly selected, based on a reading consensus for the MASEI positivity scoring ≥ 18/136.
Analysis
Continuous data are described by mean (SD) and categorical variables and expressed as frequencies and percentages. To compare groups, we used the chi-square test (or Fisher’s exact test when chi-square was not possible) and 1-way ANOVA (depending on categorical/continuous variables) with Bonferroni correction for posthoc tests. Interreader reliability was assessed with Cohen’s κ. SPSS 17.0 version was used for management and statistical analysis.
RESULTS
Patient and control demographic and clinical characteristics are shown in Table 1.
Patients and control characteristics. Values are n (%) unless otherwise specified.
All of the patients with SpA fulfilled the axial 2009 ASAS criteria10. Their mean disease duration was 9.6 years. BASDAI and ASDAS mean (SD) scores were 3.14 ± 1.9 and 1.78 ± 1.01, respectively.
No athletes and 3 non-athlete controls (10%) reported chronic low back pain history. Heel pain history was reported in 56.3%, 20.0%, and 0.0% in the SpA, athlete, and non-athlete groups, respectively. Achilles tendon palpation was painful in 23.3%, 6.9%, and 0.0% of the SpA, athlete, and non-athlete subjects, respectively.
Difference in US enthesis scores among the groups
The mean MASEI and individual subitem scores were significantly higher in the patients with SpA than in both healthy control groups (Figure 1). There was no significant difference between the athlete and non-athlete healthy groups. The percentage of patients with a MASEI score ≥ 18 was 70.0%, 16.7%, and 13.7% in the patients with SpA, athletes, and non-athlete control groups, respectively. Each elementary lesion assessed with the MASEI score was significantly more frequent in the patients with SpA than in the controls, except for bursitis (Table 2). The interreader reliability κ value was 0.68.
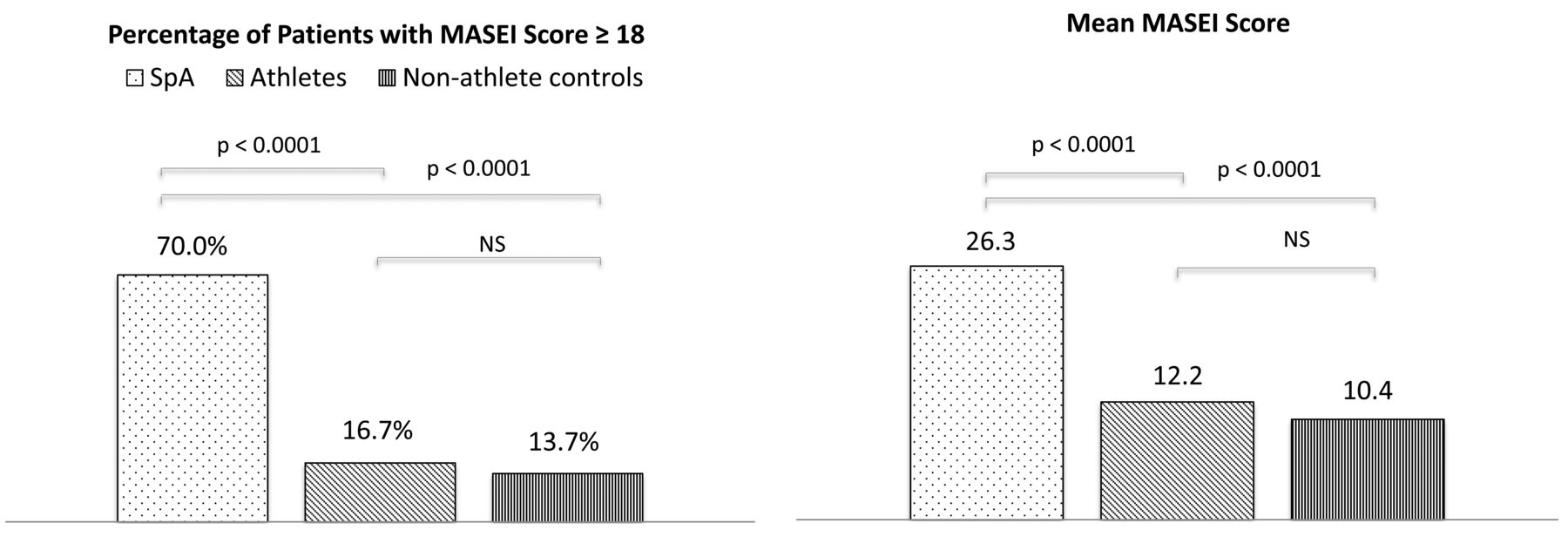
Percentage of patients with a MASEI score ≥ 18 and mean MASEI score in patients with SpA, athletes, and non-athlete controls. MASEI: MAdrid Sonographic Enthesis Index; SpA: spondyloarthritis; NS: not significant.
MASEI elementary lesions in patients with SpA, athletes, and non-athlete controls. Values are mean (SD).
Correlation between heel clinical and US findings
The prevalence of Achilles enthesitis was 23%, 3%, and 0% (p < 0.006) in the SpA, athlete, and non-athlete groups, respectively. No correlation was found in any of the 3 groups between heel enthesis and the MASEI total score, or with PD+ at the calcaneal entheses. In the SpA group, no significant correlation between the BASDAI or ASDAS and MASEI score was found.
DISCUSSION
To our knowledge, no study has ever compared the prevalence of US enthesitis in athletes playing a sport with strains in the lower limbs with those observed in patients with SpA.
In our study, we aimed to analyze the usefulness of the MASEI score in differentiating patients with axSpA from healthy controls, whatever their daily physical/sports activity. We chose the MASEI score because it is the only validated scoring system, including a PD assessment, with a proposed cutoff point9,11. In their articles, de Miguel, et al did not describe the physical activity of the controls.
In our study, the MASEI score was significantly higher in patients with SpA compared with the healthy controls, athletes, and non-athletes. Even if the MASEI score was somewhat higher in the athlete control group than in the non-athlete group, the difference was not significant. These results confirm the diagnostic accuracy of the MASEI score, whatever the physical activity of the subjects.
One of our concerns was the prevalence of Achilles enthesitis in the athlete group. We demonstrated a clear difference between the patients with SpA and the athletes (23% vs 3%, p = 0.052). There was, therefore, a significant proportion of PD+ Achilles tendon enthesitis in patients with SpA, but we were surprised by the low prevalence in the athlete group despite a state of regular overuse. Indeed, we previously showed that a simple walking exercise significantly increases the MASEI score12. These findings suggest that the increase could be reversible and probably related to mechanical stress13. They also emphasize the need to propose systematic rest before any US assessment of enthesis.
The MASEI score was significantly higher in patients with SpA compared with healthy controls, athletes, and non-athletes. The MASEI appears to be of value to distinguish SpA from healthy subjects, whatever their physical activity.
Acknowledgment
The authors are grateful to Peter Tucker for his careful reading of the manuscript.
Footnotes
Supported by a grant from APHM, France.
- Accepted for publication January 4, 2017.








{kind=link}