

Abstract
Objective. To assess mortality related to musculoskeletal (MSK) disorders and rheumatoid arthritis (RA), specifically, among adults (aged ≥ 20 yrs) in southern Sweden using the multiple-cause-of-death approach.
Methods. All death certificates (DC; n = 201,488) from 1998 to 2014 for adults in the region of Skåne were analyzed when mortality from MSK disorders and RA was listed as the underlying and nonunderlying cause of death (UCD/NUCD). Trends in age-standardized mortality rates (ASMR) were evaluated using joinpoint regression, and associated causes were identified by age- and sex-adjusted observed/expected ratios.
Results. MSK (RA) was mentioned on 2.8% (0.8%) of all DC and selected as UCD in 0.6% (0.2%), with higher values among women. Proportion of MSK disorder deaths from all deaths increased from 2.7% in 1998 to 3.1% in 2014, and declined from 0.9% to 0.5% for RA. The mean age at death was higher in DC with mention of MSK/RA than in DC without. The mean ASMR for MSK (RA) was 15.5 (4.3) per 100,000 person-years and declined by 1.1% (3.8%) per year during 1998–2014. When MSK/RA were UCD, pneumonia and heart failure were the main NUCD. When MSK/RA were NUCD, the leading UCD were ischemic heart disease and neoplasms. The greatest observed/expected ratios were seen for infectious diseases (including sepsis) and blood diseases.
Conclusion. We observed significant reduction in MSK and RA mortality rates and increase in the mean age at death. Further analyses are required to investigate determinants of these improvements in MSK/RA survival and their potential effect on the Swedish healthcare systems.
Musculoskeletal (MSK) disorders are a heterogeneous group of chronic conditions that can lead to acute and chronic pain, impaired mobility and function, decreased quality of life including mental health impairments, and mortality1. MSK disorders are among the leading causes of disability, accounting for 18.5% of the years lived with disability2 and ranked as the seventh contributor of disability-adjusted life years globally in 20153. In addition, MSK burden is expected to dramatically increase in the coming decades because of population growth, aging, obesity, and increased sedentary lifestyle4. Rheumatoid arthritis (RA) is a common chronic MSK disorder affecting 0.5% to 1.0% of the adult population in the most developed countries. It is the main chronic inflammatory rheumatic disease and is known to be associated with increased mortality5. In a recent study in Sweden, RA was reported as the leading cause of death among MSK disorders, with about 33% of all MSK deaths attributable to RA6.
MSK conditions have not been perceived as “fatal” and the evidence on associated mortality has been sparse7. There has been a growing body of evidence on mortality rates among people with some MSK disorder including RA compared with the general population8,9,10,11,12. However, MSK disorders are rarely studied as causes of death. In addition, causes of death studies are generally limited to the underlying cause of death (UCD). In Sweden, the age-standardized mortality rates of MSK (RA) as the UCD were 24.9 (8.9) and 16.0 (3.4) per million person-years for women and men, respectively6. While the UCD provides important insights, it underestimates the involvement of the chronic conditions, which are more likely to be one of several contributing diseases13. This is especially the case for MSK disorders, which are more common among older people who generally suffer from multiple comorbidities14,15. For example, the proportion of death certificates with RA as the underlying cause to death certificates with any mention of RA was 28% in São Paulo, Brazil16, and 41% in France17. A multiple-cause-of-death approach has been suggested as a superior alternative because it provides a more comprehensive picture of mortality related to chronic conditions13. In addition, data on multiple causes of death can be used to evaluate the associations between diseases listed on a death certificate18. While this approach has been used in studies on RA and osteoporotic fractures16,17,19,20, it has not been used for MSK disorders. The aim of our current study was to evaluate the effect of MSK disorders and RA specifically on mortality among people aged 20 years and older in southern Sweden between 1998 and 2014 using a multiple-cause-of-death approach. We also investigated the patterns of causes of deaths associated with MSK and RA over the same period.
METHODS AND MATERIALS
Setting and data
The region of Skåne is the southernmost province of Sweden and has an area of 11,027 km2. In 2014, it had a population of 1,288,908 (13.2% of Sweden’s entire population), distributed among 33 municipalities (www.scb.se). We obtained data on all death certificates issued in the region of Skåne between 1998 and 2014 from the Swedish National Board of Health and Welfare’s Cause of Death Register (www.socialstyrelsen.se). The death certificates are filled out according to the World Health Organization (WHO) recommendations and consist of 2 parts. In Part I, a sequence of conditions leading to death including the UCD are recorded. In Part II, all other contributing/contributory conditions that did not directly lead to UCD are reported. For our study, the following data on the death certificate were used: the de-identified personal number, sex, age, date of death, the UCD, and up to 20 additional causes of death according to the International Classification of Diseases, 10th ed (ICD-10). We defined all causes on death certificates other than the UCD as nonunderlying causes of death (NUCD). We identified MSK deaths as ICD-10 codes M00–M99, and RA deaths as ICD-10 codes M05–M06. For our current study, we included death certificates for people aged 20 years and older who were registered inhabitants in Skåne at the time of death. The study was approved by the Lund University ethics committee (Dnr 2014/276).
Statistical analysis
The percentage of MSK (RA) from all deaths and the ratio of MSK (RA) as an UCD to any mention were calculated by sex, age group, and year. The mean age at death and number of causes listed on death certificates with any mention of MSK (RA) were compared to death certificates without these conditions. When MSK (RA) was reported as an UCD, we examined most common NUCD recorded on death certificates and inversely when MSK (RA) was recorded as an NUCD, we evaluated the most common UCD. To assess whether these patterns changed over time, we considered 2 subperiods (1998–2002 and 2010–2014) and reported the difference in proportions with 95% CI using the Newcombe-Wilson hybrid score21.
We computed annual age-standardized mortality rates per 100,000 population by means of direct standardization using the WHO Reference Population with age groups of 5 years (20–24, 25–29, …, 85+). The population data by sex and age groups were obtained from the Statistics Sweden (www.scb.se). We also calculated age-specific death rates for 6 age groups (20–49, 50–59, 60–69, 70–79, 80–89, and 90+). We analyzed death certificates with MSK (RA) reported as (1) an UCD and (2) any mention on death certificate. The average annual percent change (95% CI) in age-standardized mortality rates of MSK (RA) as an UCD and with any mention were obtained from joinpoint regression with permutation tests22 available in the Joinpoint Regression Program version 4.2.0.2 (surveillance.cancer.gov/joinpoint).
The associations with other conditions were assessed by dividing the number of observed pairs of causes of death (O) on the number of expected pairs of causes (E), based on the assumption of independence13. The expected numbers of deaths were estimated using cross tabulation of MSK/RA and a specific cause mention on death certificates. An O/E ratio higher (lower) than 1 shows that more (fewer) deaths with paired causes were observed than could be expected by chance if the paired causes were independent. The O/E ratios were adjusted for sex and age and were reported with 95% CI.
RESULTS
MSK (RA) was mentioned on 5732 (1512) death certificates out of a total of 201,488 death certificates registered in the region of Skåne among people ≥ 20 years during 1998–2014, with a women-to-men ratio of 2.3 for MSK and 3.5 for RA (Table 1). On average, MSK (RA) was reported as an UCD in 19.6% (24.4%) of death certificates with any mention of MSK (RA), with slightly higher values in women compared with men. While the proportion of MSK (RA) reported as an UCD among all death certificates was stable between 1998 and 2014, the proportion of any mention of MSK (RA) among all death certificates increased (declined) from 2.7% (0.9%) in 1998 to 3.1% (0.5%) in 2014. Therefore, the reporting of MSK (RA) as an UCD among all certificates listing MSK (RA) decreased (increased) during the study period (Supplementary Tables 1 and 2, available with the online version of this article). Across age groups, the highest proportions of MSK- and RA-related mortality were observed in the age group 80–89 years (Supplementary Table 3, available with the online version of this article).
Characteristics of death certificates with mention of MSK disorders/RA in southern Sweden, 1998–2014.
Mean number of causes and age at death
The mean ± SD number of causes on death certificates with any mention of MSK (RA) was 5.6 ± 2.4 (5.0 ± 2.2; Supplementary Figure 1, available with the online version of this article). There were more causes listed on death certificates with any mention of MSK (RA) compared with those without any mention (mean difference 2.4, 95% CI 2.3–2.4 causes for MSK and mean difference 1.7, 95% CI 1.6–1.8 causes for RA; Supplementary Figure 2, available with the online version of this article). The mean age at death (95% CI) increased by 2.6 years (1.9–3.3) and 1.8 years (0.6–3.0) for death certificates with any mention of MSK and RA, respectively, between the 2 subperiods. Compared with death certificates without MSK/RA mention, the mean age at death was higher for death certificates with any mention of MSK/RA (mean difference 2.8, 95% CI 2.4–3.1 yrs for MSK and mean difference 1.1, 95% CI 0.4–1.7 yrs for RA), and this gap increased over the study period (Figure 1).

The mean (95% CI) age at death for death certificates with any/no mention of musculoskeletal disorders/rheumatoid arthritis, 1998–2014.
Time trends in mortality rates
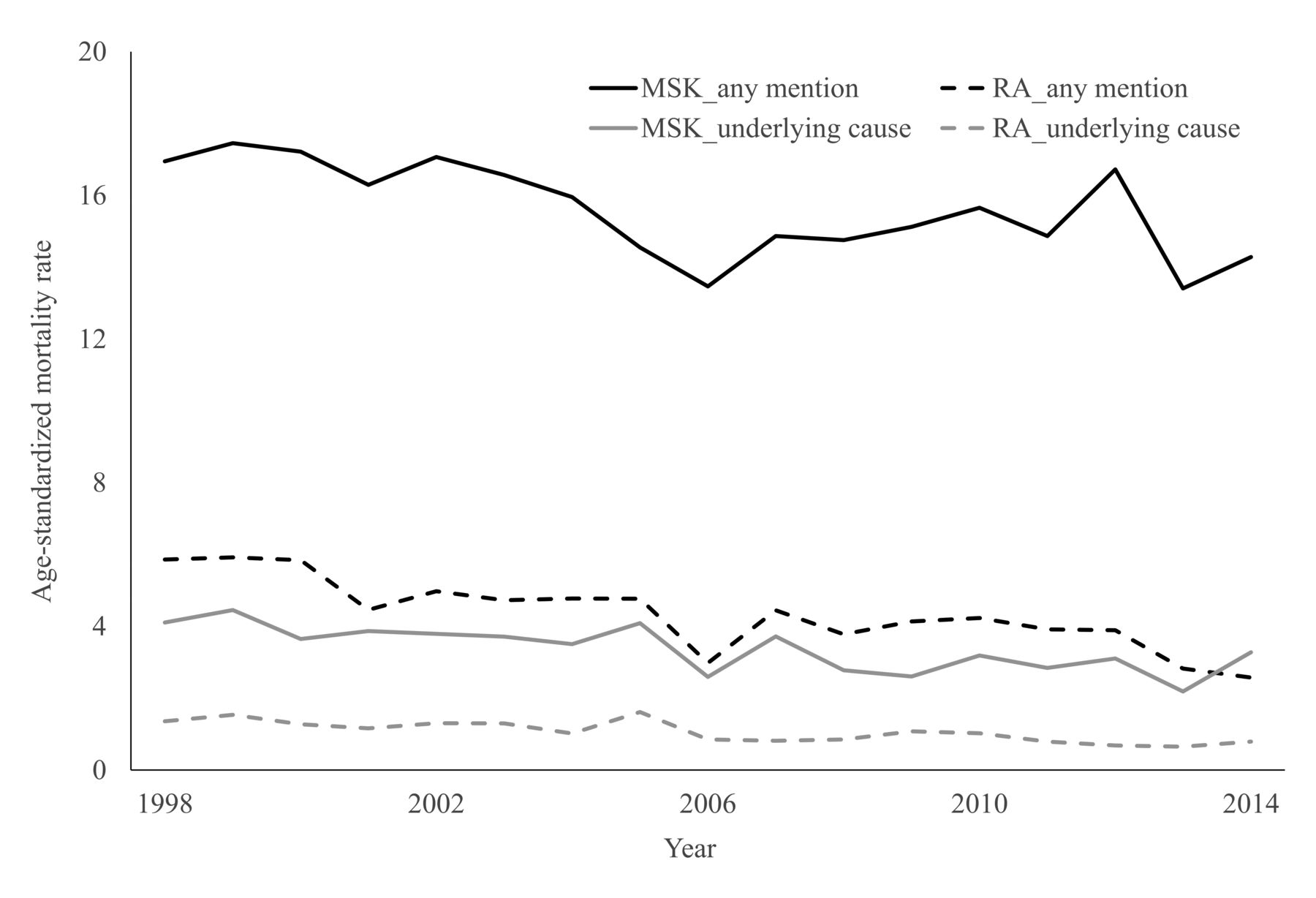
The mean age-standardized mortality rate of MSK (RA) was 15.5 (4.3) per 100,000 person-years. The joinpoint regression showed that the age-standardized mortality rates of MSK (RA) declined by 2.7% (4.4%) per year as an UCD and 1.1% (3.8%) per year with any mention (Figure 2). In addition, age-specific mortality rates were stable or declined in all age groups except MSK mortality in the oldest age group (Supplementary Figures 3 and 4, available with the online version of this article).

Age-standardized mortality rate per 100,000 person-years for MSK disorders/RA as underlying cause and any mention on death certificates, 1998–2014. MSK: musculoskeletal; RA: rheumatoid arthritis.
Associated causes of deaths
When MSK was reported as an UCD, the most common NUCD were pneumonia (28.4%) and heart failure (19.9%), and the proportion of most NUCD were stable/increased between the 2 subperiods (1998–2002 and 2010–2014; Table 2). When MSK was recorded as an NUCD, the most common UCD were diseases of the circulatory system (48.3%), neoplasms (13.7%), and diseases of the respiratory system (8.3%; Table 3). There were statistically significant increases in certain infectious and parasitic diseases, mental disorders, and diseases of the nervous system as an UCD on death certificates with MSK as an NUCD between the 2 subperiods. There were statistically significant increases in infectious and hypertensive diseases as an UCD on death certificates with RA as an NUCD between the 2 subperiods.
NUCD when MSK disorders/RA were the underlying cause of death. The most common NUCD are listed. Values are number (%) unless otherwise specified.
The UCD on death certificates with MSK disorders/RA listed as a nonunderlying cause of death. The most common underlying causes of death are listed. Values are n (%) unless otherwise specified.
For both MSK and RA, the greatest O/E ratios were seen for infectious diseases and diseases of the blood and blood-forming organs. All causes but neoplasms, mental disorders, and cerebrovascular diseases were reported more often than expected by chance on death certificates with any mention of MSK (Table 4). The similar patterns were generally observed for RA except diabetes mellitus, mental disorders, diseases of the nervous system, and ischemic heart diseases.
Age- and sex-adjusted observed/expected ratios for joint mention of MSK disorders/RA and a specific cause. Both underlying and nonunderlying causes of death are included. Numbers in parentheses are 95% CI, and numbers in brackets are the observed no. death certificates with joint mention of a specific cause and MSK disorders/RA.
DISCUSSION
In our current study, we analyzed all death certificates registered in southern Sweden from 1998 to 2014 and found that MSK disorders were reported on about 3% of all death certificates. For both MSK and RA, the age-standardized mortality rates declined and the mean age at death increased during the study period. The pattern of mortality suggested an increase in the frequency of mental disorders and diseases of the nervous system on death certificates with mention of any MSK.
The observed proportion of RA-related deaths from all deaths in our study (0.75%) was substantially higher than that reported in São Paulo, Brazil (0.11%)16, France (0.22%)17, and the United States (0.41%)23. Moreover, ratio of UCD to any mention of RA was lower in our study (0.24) compared with São Paulo, Brazil (0.28)16, and France (0.41)17. Higher incidence and prevalence of RA in north European and North American countries compared with south European and developing countries24 might partially explain higher RA mortality in Sweden and the United States than in France and Brazil. In addition, differences in quality of cause-of-death registration and coding practices might be other potential reasons for the observed disparities.
The observed declining trend in MSK and RA age-standardized mortality rates in our study is in line with previous studies6,16,17,23. Moreover, the mean age at death increased over the study period and this increase was higher than the observed increase for death certificates without any mention of MSK (RA). In line with this, more recent population-based cohort studies reported a greater improvement in survival of patients with RA than the general population in the United Kingdom and Canada25,26,27. These favorable changes are possibly due to improvement in management of MSK disorders, including an early and aggressive treatment with disease-modifying antirheumatic drugs for RA. While the higher mean age at death for RA compared with the general population in our study is in contrast with findings from Brazil16 and France17, it is in line with a study in France28 and a previous study in Finland29. The observed inconsistency might be due to between-country differences in diagnosis and treatment of RA (which might influence the effect of aging on RA incidence and progression), in the age composition of the population, and in cause-of-death coding practices. In addition, higher mortality rates among women compared with men are attributed to higher prevalence of MSK and RA among women30,31.
In parallel to previous studies, when MSK (RA) were recorded as an UCD, pneumonia was the most common NUCD and when MSK (RA) were reported as an NUCD, diseases of the circulatory system were the main UCD16,29,32. In addition, leading underlying causes of deaths were similar with the general population (i.e., diseases of the circulatory system, neoplasms, and diseases of the respiratory system). In a review of studies over 60 years, Sokka, et al14 reported significant similarity in patterns of causes of death in patients with RA compared with the general population. Further, we observed increases in the proportion of deaths with infections, mental disorders, and diseases of nervous system as UCD on death certificates with MSK as an NUCD. On the other hand, proportion of deaths with diseases of the circulatory system as UCD declined over the study period. We observed similar patterns in the general population in our data. This highlights potential shifts in the burden of diseases in Sweden in coming years, which should be taken into account by policymakers.
The observed associations between MSK (RA) with other causes are consistent with previous studies16,17,28. The strongest positive associations were observed with infections, diseases of the blood, and renal failure. The positive association with infections including pneumonia has been attributed to the use of some drugs (e.g., methotrexate, antitumor necrosis factor agents, and prednisone) and the association of active RA with reduced response to infection33,34,35. Hypertension, amyloidosis, glomerulonephritis, and analgesic abuse have been suggested as potential causes of renal failure in people with systemic lupus erythematosus and RA36,37. The negative association with neoplasm might be because of underreporting of comorbid conditions in deaths with neoplasms as UCD (i.e., tendency to report fewer causes on death certificates with neoplasm as an UCD)38,39. In our data, the mean number of causes on death certificates with neoplasms (ICD-10 codes: C00.0–D48.9) as UCD was only 2.6 while the corresponding number for diseases of the circulatory system (ICD-10 codes: I00–I99), diseases of the respiratory system (ICD-10 codes: J00–J99), and MSK disorders (ICD-10 codes: M00–M99) was 3.5, 3.4, and 4.6, respectively. Comparing O/E ratios between 2 subperiods suggested that the associations between MSK (RA) with other causes were generally constant over time. This is consistent with findings from a previous study in southern Sweden which reported similar excess cardiovascular mortality over time among patients with RA40.
Using the multiple-cause-of-death approach and access to all death certificates over 17 years in Skåne are the main strengths of our current study. However, there are limitations mainly related to our data source (i.e., death certificates). It is well recognized that MSK including RA are underreported on death certificates15,41. Moreover, diagnostic inaccuracy and incompleteness of death certificate are also concerns. Because of inherent limitations in the study design and data source (i.e., death certificate), any causal inference from the findings should be avoided. The small number of deaths and the wide CI, particularly for RA, call for caution in interpreting the results. In addition, we included MSK only according to ICD-10 chapter XIII (M-codes). This means that fractures (mainly S-codes in ICD-10 chapter XIX) were not identified, which resulted in an underestimate of the total MSK-related mortality. Investigating mortality related to fractures is a subject for future research.
We found a declining trend in the age-standardized mortality rate of MSK and RA in southern Sweden. We also noted that the mean age at death increased over time with a larger gain for death certificates with any mention of MSK including RA compared with the general population. On one hand, reduction in MSK and RA mortality rates and an increase in the mean age at death alongside population aging imply that in the coming years, not only will the number of people having these disorders increase, but also people will live longer with these conditions. On the other hand, such improvements in life longevity alongside decline in RA disease activity might lead to less old-age dependency, more years of productive work, and improvements in work productivity. Further analyses are required to investigate determinants of observed decline in MSK/RA mortality and the actual effect of improved survival on healthcare systems and societies.
ONLINE SUPPLEMENT
Supplementary material accompanies the online version of this article.
Footnotes
Supported by the Swedish Research Council, Crafoord Foundation, Greta and Johan Kocks Foundation, The Swedish Rheumatism Association, the Faculty of Medicine Lund University, Governmental Funding of Clinical Research within National Health Service (ALF), and Region Skåne.
- Accepted for publication January 25, 2017.








{kind=link}
{kind=link}