

Abstract
Objective. To develop preliminary treat-to-target (T2T) recommendations for psoriasis and psoriatic arthritis (PsA) for Canadian daily practice.
Methods. A task force composed of expert Canadian dermatologists and rheumatologists performed a needs assessment among Canadian clinicians treating these diseases as well as an extensive literature search on the outcome measures used in clinical trials and practice.
Results. Based on results from the needs assessment and literature search, the task force established 5 overarching principles and developed 8 preliminary T2T recommendations.
Conclusion. The proposed recommendations should improve management of psoriasis and PsA in Canadian daily practice. However, these recommendations must be further validated in a real-world observational study to ensure that their use leads to better longterm outcomes.
The recent influx of novel therapies for the treatment of psoriasis and psoriatic arthritis (PsA), as well as the development of outcome measures that can detect changes and differences between therapies in clinical trials, has greatly enhanced the need for standardized appropriate assessment of these diseases in Canadian daily practice. Additionally, there is a growing interest in applying the treat-to-target (T2T) approach to the management of chronic conditions such as psoriasis and PsA. This is because severe psoriasis is a risk factor for adverse outcomes including cardiovascular disease (CVD) and PsA1; and delayed consultations for PsA result in more severe disease2,3. The core of the T2T approach is in guiding treatment toward specific and measurable targets, which require frequent and objective assessment of disease activity through validated measures. The overall goal is to provide clinicians with guidance for assessing treatment outcomes and determining when to continue or modify treatment. Selecting a treatment target involves consideration of effectiveness, tolerance, adherence, as well as patient-centered outcomes and satisfaction.
Therapeutic areas where the T2T concept has been implemented have demonstrated that the use of a measurable, target-oriented approach [e.g., blood pressure and cholesterol levels for heart disease, glucose levels for diabetes, and remission or low disease activity for rheumatoid arthritis (RA)] confers better clinical outcomes4. However, there is less evidence regarding the value of defining and ultimately treating to therapeutic targets in psoriasis and PsA. In addition, changes in disease activity over time and in associated comorbidities can further complicate the management of psoriasis and PsA with regards to the T2T approach.
To further assess and validate the use of various outcome measures and the applicability of the T2T concept in the management of psoriasis and PsA in daily practice, a group of Canadian experts in these therapeutic areas formed a task force. The ultimate goal of the task force was to develop preliminary T2T recommendations for the treatment of psoriasis and PsA in Canada, and to further validate and improve the recommendations through future research and educational initiatives.
MATERIALS AND METHODS
The development of preliminary T2T recommendations for psoriasis and PsA comprised several steps. First, a Steering Committee was assembled consisting of Canadian rheumatologists and dermatologists who were identified based on their expertise in treating psoriasis and PsA, participation in clinical trials, and their involvement in the development of consensus statements. The inaugural Steering Committee meeting, which took place in Toronto, Ontario, Canada on April 4, 2014, identified potential unmet needs and topics of interest, and outlined the working platform upon which roles and responsibilities were assigned.
To assess the needs, interest, and willingness of community clinicians in applying the T2T concept in their daily practice, the Steering Committee conducted a series of needs assessment surveys during the summer and fall of 2014. Responses (from 90 dermatologists and 26 rheumatologists) representative of Canadian practice were gathered and analyzed. The surveys revealed interest in the T2T concept with a great majority of participants agreeing or strongly agreeing that there is a need for such an approach. The surveys also provided insight regarding current treatment patterns, tools, and outcome measures used in daily practice. Moreover, the main potential barrier identified for the development of T2T recommendations was timely access to specialists and approved therapies. This valuable feedback was taken into consideration during subsequent discussions and led to the development of the recommendations.
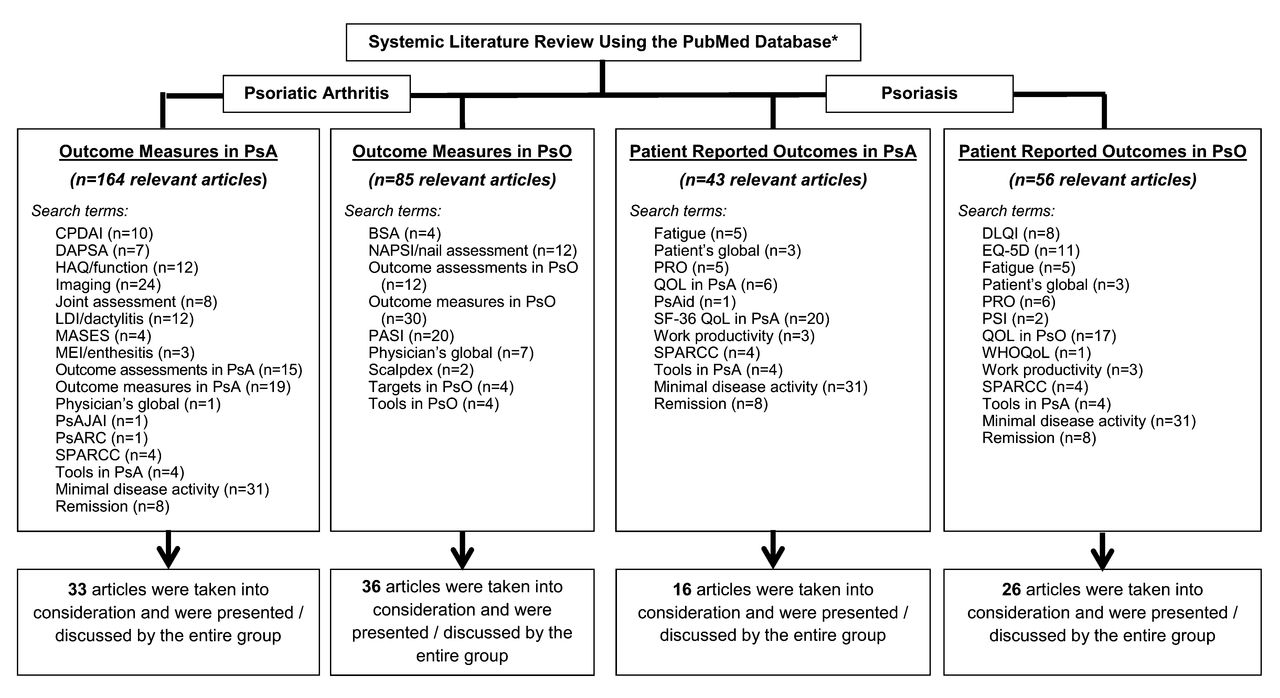
The Steering Committee also regarded a comprehensive systematic literature review as a mandatory initial step (Figure 1). The available literature and background evidence served as a basis for defining overarching principles and consideration of treatment targets. The literature search included terms related to outcome measures and tools commonly used to assess the effectiveness of therapies for treating psoriasis and PsA, as well as definitions of remission and minimal disease activity (MDA) applied to these conditions. Articles published between January 2000 and June 2015 were taken into consideration and the search resulted in 348 citations. The citations were divided into 4 categories: (1) outcome measures in psoriasis, (2) outcome measures in PsA, (3) patient-reported outcomes (PRO) in psoriasis, and (4) PRO in PsA. These topics were assigned to Steering Committee members who, based on scientific validity and relevance to Canadian practice, selected “key” publications and discussed their content during a second Steering Committee meeting that took place in Toronto on August 29, 2015.

Literature search, topics, and article selection. * Articles published between January 2000 and June 2015 were taken into consideration. Rationale for selecting articles published after 2000 was to identify changes in the management of psoriasis and PsA influenced by the introduction of biologics. PsO: psoriasis; PsA: psoriatic arthritis; CPDAI: Composite Psoriatic Disease Activity Index; DAPSA: Disease Activity in Psoriatic Arthritis; HAQ: Health Assessment Questionnaire; LDI: Leeds Dactylitis Index; MASES: Maastricht Ankylosing Spondylitis Enthesis Score; MEI: Mander Enthesis Index; PsAJAI: Psoriatic Arthritis Joint Activity Index; PsARC: Psoriatic Arthritis Response Criteria; SPARCC: Spondyloarthritis Research Consortium of Canada; BSA: body surface area; NAPSI: Nail Psoriasis Severity Index; PASI: Psoriasis Area and Severity Index; PRO: patient-reported outcomes; QOL: quality of life; PsAID: Psoriatic Arthritis Impact of Disease; SF-36: Medical Outcomes Study Short Form-36; DLQI: Dermatology Life Quality Index; PSI: Psoriasis Symptom Inventory; WHOQoL: World Health Organization Quality of Life.
Based on the discussions, the Steering Committee formulated 5 over-arching principles upon which 8 preliminary T2T recommendations were proposed.
PSORIASIS OUTCOME MEASURES
Psoriasis is a chronic, inflammatory disease associated with considerable morbidity and many comorbid conditions. The severity of psoriasis is defined not only by the extent of body surface area (BSA) involvement, but also by location and visibility of lesions, which may interfere significantly with activities of daily life and have a substantial psychological effect on patient well-being and ability to function. The psoriatic lesions usually have variable degrees of erythema, induration, and scaling. Several guidelines that provide in-depth information on diagnosis and treatment options for psoriasis emphasize the importance of assessing disease severity using validated scales5,6,7,8,9.
Disease Activity Measures
The most commonly used assessment tools for disease activity in psoriasis include the Psoriasis Area and Severity Index (PASI)10, the physician’s global assessment (PGA)11, and the assessment of BSA12 affected by the disease.
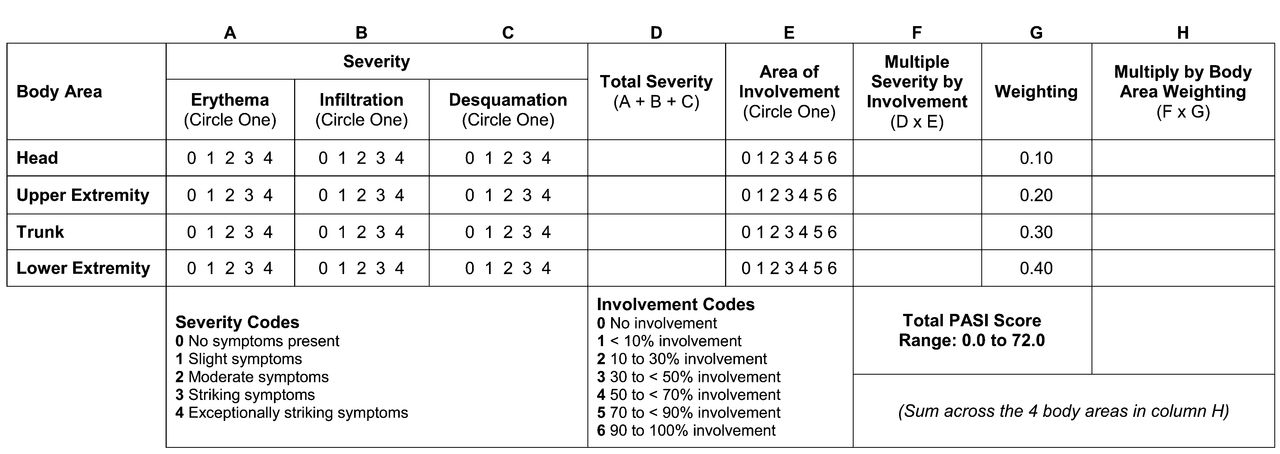
The PASI score combines the assessment of the severity of lesions (including erythema, induration, and scale) and the area affected into a single score from 0 (no disease) to 72 (maximal disease; Figure 2)10. The PASI score has been validated in different patient populations and it correlates well with other outcome measures such as PGA and PRO13,14,15,16; the PASI 75 (i.e., reduction in PASI score by ≥ 75%) is a commonly used primary endpoint in clinical trials assessing therapies for psoriasis7,8. However, a treatment goal of PASI 90 or 100 has become an attainable target17,18. One should also consider that an absolute PASI value might provide a better benchmark, irrespective of the baseline PASI17. Absolute PASI values of ≤ 3 may be a better benchmark of therapeutic success, irrespective of the time of assessment17,19,20. Further, changes in treatment are often requested (and made) when PASI values exceed 5, regardless of baseline. This is especially relevant for patients with high baseline PASI values. For example, reaching a PASI of 5 from a baseline PASI of 20 qualifies the patient as a PASI 75 responder, but the patient (and physician) may be unsatisfied with results.

Calculation of PASI. PASI: Psoriasis Area and Severity Index31. From Rich and Scher. J Am Acad Dermatol 2003; 49:206–12; with permission
Limitations of the PASI score, especially for daily clinical practice, include its complexity and lack of ability to provide a quick estimate of the BSA affected21. The PASI score is not linearly reflective of psoriasis severity and, therefore, improvement in PASI score does not always correspond to clinical relevance. In addition, PASI scoring does not always consider the disease burden reflected in more sensitive areas (e.g., face, genital area, hands, feet) and its effect on quality of life (QoL). Some components of the PASI score tend to respond more readily to treatment (e.g., induration and desquamation) than others (e.g., erythema)21. Moreover, the speed of response typically differs between body regions (e.g., improvement is often observed initially on the head and progresses more slowly on the limbs)21.
While the PASI combines the assessment of the severity of lesions and the area affected into a single score, the PGA assesses overall disease severity and categorizes it into 5 categories: clear, almost clear, mild, moderate, and severe (Table 1)22. Although there are several variants of PGA11,22,23,24, most are fairly straightforward and easy to use in daily practice11,22,23. PGA has been used and recommended as the preferred tool for daily practice by various dermatology groups and organizations9. One of the limitations of the PGA is that it does not provide an indication of the BSA affected. For example, a patient with extensive surface involvement could have the same PGA score as a patient with limited area involvement if the degrees of lesion erythema, induration, and desquamation are the same. Moreover, the PGA does not incorporate any assessment of the affected area or anatomical regions. In daily practice, many clinicians might opt to use a combination of the PGA and BSA25.
Physician’s global assessment for psoriasis22. From Pascoe VL, et al. JAMA Dermatol 2015;151:375-81; with permission.
The common measure of BSA affected by psoriasis assumes that the surface of the patient’s palm is about the equivalent to 1% of the total BSA (Figure 3)12. As depicted in Figure 3, the palm includes the surface area of the palmar side of the hand, including the 5 digits, because this is about the equivalent to 0.8% (men) or 0.7% (women) of the BSA12. The Patient Report of Extent of Psoriasis Involvement method involves patient assessment of the severity of their disease using the palm of their hand as a measure26. The method appears to be a reliable, valid, and responsive measure of BSA affected by psoriasis. It is responsive to change and, therefore, may be useful to monitor BSA affected by psoriasis by patients who want to be involved in decisions about the management of their disease. Computerized multiview imaging methods have also been developed to more precisely assess the BSA affected by the disease27. A patient is photographed from 4 different poses (front, back, right, and left) to ensure that the entire BSA is acquired. BSA is calculated based on body weight and height estimation. Although, interestingly, it is not likely that computerized methods will be used in daily practice in the near future.

Measurement of the BSA with the Rule of Hand Method12. One palm of a patient’s hand is equal to about 1% of BSA. BSA: body surface area.
Tools for assessing nail and scalp psoriasis
Nail involvement is a common feature of psoriasis and PsA, predicting higher disease severity and greater impairment of QoL. Thus, clearing nail disease should be 1 of the therapeutic targets for both psoriasis and PsA. Studies have indicated that nail involvement is a more common and more important manifestation in patients with PsA than in those with cutaneous psoriasis28,29,30. Characteristic changes involving the nail matrix include pitting, leukonychia, lunular red spots, and nail plate crumbling, and changes in the nail bed including onycholysis, splinter hemorrhages, oil drop (salmon patch) discoloration, and nail bed hyperkeratosis.
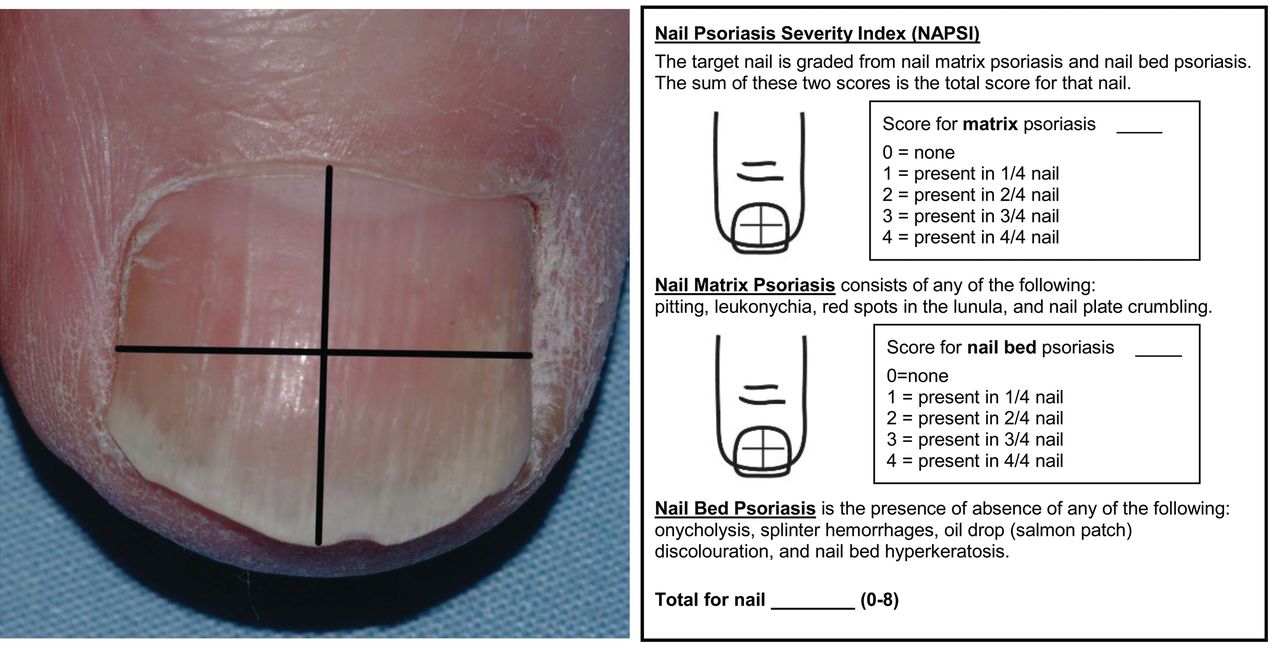
The Nail Psoriasis Severity Index (NAPSI), the most comprehensive assessment of nail disease used in onycholysis clinical trials (Figure 4)31, is a numeric, reproducible, and objective tool for evaluation of nail matrix and nail bed psoriasis. With the nail divided into quadrants by imaginary horizontal and longitudinal lines, each quadrant is given a score for nail bed psoriasis (0–4) and nail matrix psoriasis (0–4), depending on the presence of any of the features of nail psoriasis in that quadrant. This yields a potential total score of 80 when only the fingernails are assessed and 160 when the toenails are included. A modification of this system, the mNAPSI, is a shorter and more feasible scoring system in which each variable is graded from 0 to 3 to obtain a more sensitive system for assessing nail changes in response to therapy. The mNAPSI has demonstrated excellent internal consistency (Cronbach alpha = 0.98) and interrater reliability (ICC 0.92, 95% CI 0.87–0.97)32. Nail scores and physicians’ global nail severity visual analog scores showed good inter- and intrarater correlations (Spearman rho = 0.85 and 0.90–0.99, respectively; p < 0.01)32. A significant correlation (p < 0.05) was also found between mNAPSI scores and several other clinical measures of PsA [including physician’s global PsA disease severity visual analog scale (VAS), swollen joint count (SJC), tender joint count (TJC), and patient’s global nail severity VAS], providing construct validity32. The mNAPSI proved reliable by both dermatologists and rheumatologists in an international study that assessed the reliability of both skin and joint assessments in PsA33.

Nail Psoriasis Severity Index31. From Rich and Scher. J Am Acad Dermatol 2003;49:206–12; with permission.
PRO and Available Tools
PRO, such as health-related QoL (HRQOL) and preference-based utilities, are major outcome variables in both clinical trials and clinical practice34. A literature review by Kitchen, et al34 identified 45 PRO measures used in psoriasis: 16 were specific to psoriasis, 21 assessed other dermatological conditions, and 8 were developed for generic nondermatological health conditions. Thus, several generic and dermatology-related instruments can be used to assess QoL in patients with psoriasis35,36.
The Dermatology Life Quality Index (DLQI) is the most frequently used instrument for the assessment of HRQOL in patients with skin diseases37,38,39. It has been used for over 20 years in 50 different skin conditions. DLQI consists of 10 questions concerning patients’ perception of the effect of skin diseases on different aspects of their QoL over the last week. Each item is scored on a 4-point Likert scale (0 = not at all/not relevant, 1 = a little, 2 = a lot, and 3 = very much). Scores of individual items are added to yield a total score (maximum 30); higher scores mean greater impairment of the patient’s QoL. Strong significant correlations were found among DLQI, PASI, PGA, and self-assessed disease severity on VAS40,41. The dimensions of DLQI and the Medical Outcomes Study Short Form-36 (SF-36) survey are also significantly correlated with each other and the subjective measures of disease activity42. The greatest correlations are found between DLQI and the bodily pain and social functioning domains43. The main limitation of DLQI is that it is unidimensional and, therefore, does not take into consideration all psychological aspects of the disease (e.g., depression). In addition, minimally important clinical difference has not been well studied and defined; although a study by Shikiar, et al43 suggested a minimally important difference (MID) in the range of 2.3–5.7. In comparison, estimates of the MID for the SF-36 physical component summary score ranged from 0.5–3.9 with the best estimate at about 2.5 points.
The EQ-5D is an instrument often used by health economists as a short measure of generic HRQOL. It consists of a 5-item set of health status measures and a VAS, with each of the 5 health states (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression). The health states are evaluated from “no problem” to “extreme problem” and scored from 1–344. Overall, the validity and responsiveness of the EQ-5D was found to be good in people with skin diseases, especially plaque psoriasis or PsA45. The MID for the EQ-5D index score is in the range of 0.09–0.2243. A study by Norlin, et al46 showed that the EQ-5D, DLQI, and PASI identify different aspects of psoriatic disease. The EQ-5D and DLQI were moderately correlated with an absolute value of 0.55 by Spearman correlation (p < 0.001). The correlation between EQ-5D and DLQI was stronger with higher levels of clinical psoriasis severity as measured by PASI. EQ-5D and PASI showed a weak correlation (absolute value 0.25), whereas DLQI and PASI showed a moderate correlation of 0.51 (p < 0.001). This is to be expected because the PASI is assessed by physicians and the EQ-5D and DLQI are assessed by the patient. The moderate correlation between the EQ-5D and DLQI indicates that both measures assess the same aspect of QoL. Nevertheless, a correlation coefficient of < 1 shows that both identify different aspects of the disease and its effect on HRQOL. The study demonstrated that when assessing psoriasis treatments and making decisions about treatment guidelines and resource allocation, all 3 measures (EQ-5D, DLQI, and PASI) should be considered. They are complementary tools that answer different needs. With regards to the SF-36, similar to DLQI, the EQ-5D index score correlates mostly with the SF-36 bodily pain domain. Thus, the bodily pain domain of SF-36 appears to be the most relevant to patients. Swinburn, et al47 developed a disease-specific “bolton” version of the EQ-5D questionnaire for use in psoriasis by adding measures of “skin irritation” and “self-confidence” to the existing EQ-5D questionnaire dimensions. Regression analysis showed that EQ-5D-psoriasis was much better at predicting PRO (DLQI and self-administered PASI) when compared with the unmodified EQ-5D questionnaire.
The Psoriasis Symptom Inventory (PSI) is a recent addition to the psoriasis outcome measure armamentarium. It is an 8-item (itch, redness, scaling, burning, cracking, stinging, flaking, and pain) patient-reported, psoriasis-specific tool to assess severity of psoriasis-related symptoms; it scores from 0–32, with lower scores corresponding to a lesser severity of the signs and symptoms of psoriasis. The tool was validated in 139 patients48. Test-retest reliability was acceptable (ICC range 0.70–0.80). The PSI demonstrated good construct validity and was sensitive to within-subject change (p < 0.0001) and it correlated with DLQI items and SF-36 domains49. The highest association between the PSI and the DLQI was seen between item 1 of the DLQI (“How itchy, sore, painful, or stinging has your skin been?”) and the PSI total score (Spearman rank r = 0.73, p < 0.001). The highest association between the PSI and the SF-36 was observed with the bodily pain domain (Pearson r = −0.59, p < 0.001).
The Scalpdex is a 23-item instrument that uses a similar format as the Skindex questionnaire (designed to assess patient perception of their skin-related conditions), but the wording differs (i.e., “scalp condition” instead of “skin condition”)50. Questions are grouped into 3 categories (symptoms, emotions, and functioning), and all items inquire about the past 4 weeks. The instrument demonstrated reliability with internal consistency (Cronbach alpha = 0.62–0.80) and reproducibility (ICC 0.90–0.97). The Scalpdex was also proven to be reliable, responsive, and valid for the assessment of QoL in children with scalp psoriasis51. In some trials that assessed the effect of biologics on scalp psoriasis, a 7-point, Scalp-specific PGA or 5-point patient’s global assessment (PtGA) was used (Table 2A and Table 2B)52.
Scalp-specific global assessments52. Seven-point scalp-specific physician’s global assessment. From Krell, et al. J Am Acad Dermatol 2008;58:609–16; with permission.
Scalp-specific global assessments52. Five-point scalp-specific patient’s global assessment. From Krell, et al. J Am Acad Dermatol 2008;58:609–16; with permission.
Several studies indicated that psoriasis can have a significant effect on various aspects of patients’ daily life and function, including work productivity and family income53,54,55. This is further heightened because psoriasis is often associated with various comorbidities that can have a major effect on patient well-being56,57,58,59,60,61.
Considerations for Remission and MDA
The concept of MDA is difficult to apply to psoriasis for several reasons. First, psoriasis is a complex, non–life-threatening disease on its own, although its comorbidities are associated with an increased risk of mortality62. Second, unlike joint-related conditions, even severely inflamed and longstanding skin lesions can be cleared without residual tissue damage seen by the naked eye or conventional histology, suggesting a state of remission. However, data indicate that some upregulated genes persist in psoriatic skin 3 months after the lesions are cleared in patients treated with etanercept63. This may explain the quick relapse in some patients after cessation of therapy. Thus, the longstanding and current treatment paradigm is to clear or substantially reduce lesions, with the pathologic skin changes reverting to normal. However, since the severity of skin disease is associated with CV risk, the goal is to manage not only skin lesions, but also the associated comorbidities64. It has been demonstrated that comorbidities such as myocardial infarction, atrial fibrillation, and stroke in patients with psoriasis are correlated with the severity of skin symptoms59.
According to a highly cited European consensus report62, not achieving an improvement of PASI of 50% is defined as treatment failure or inadequate response, while an effective therapy is defined as achieving a reduction of PASI of 75% or more. However, one should keep in mind that the proposed improvements of 50% to 75% in PASI scores, which were chosen based upon common clinical trial benchmarks and not physiologic-validated endpoints, do not always reflect patient or physician preferences, and therefore other patient and disease-related factors should be taken into consideration. According to the consensus report, when the improvement in PASI falls in the range between 50% and 75%, the DLQI should be used to decide whether the treatment goals have been met. Therapy should be modified if the DLQI is > 5 and can be continued if the DLQI is ≤ 5. The most important consideration for establishing a therapeutic target, including in psoriasis, is the need to take action if the target is not met. In psoriasis, this means adjustment of treatment either by increasing the dose, decreasing dose interval, starting combination therapy, or changing medication. Challenges related to achieving a defined therapeutic target include insurance coverage, intolerability issues, patient concern, physician reluctance to use systemic treatments, and the need for regular assessment (every 3 mos) of treatment success (e.g., whether the set targets are met).
Considerations for Canadian Daily Practice
To objectively assess psoriasis in daily practice, treating clinicians can use the BSA, PASI, or PGA
These 3 measures have been validated in many instances and are widely accepted and used in clinical practice and clinical trials. Although many clinicians consider the PASI to be complex for use in routine clinical practice, we believe that this is a misconception (PASI is associated with very low administrative burden and usually takes under 2 min to perform) that can be overcome with proper training and practice. This is of particular importance because in certain situations (e.g., reimbursement requirements), clinicians might be required to provide the PASI score. Outcome measures for psoriasis in specific sites (e.g., nails and scalp) can be used, but are generally unnecessary if the 3 most common measures (BSA, PASI, or PGA) are used.
PRO, especially QoL, should be taken into consideration when developing and adjusting treatment plans, keeping in mind that PRO are often affected by life events and conditions that are not always related to psoriasis
To assess psoriasis-related QoL, we recommend the DLQI because it is a well-established tool and validated in multiple settings. EQ-5D-psoriasis has potential and should be further assessed.
Psoriasis-associated comorbidities, including PsA, CVD, gastrointestinal (GI) disease, metabolic syndrome, ocular disorders, psychiatric manifestations, and cancer should be taken into consideration when selecting appropriate therapeutic targets and the means of reaching them
Psoriasis located in sensitive areas such as the face, genital area, hands, or feet may need to be managed as severe psoriasis.
PSORIATIC ARTHRITIS: OUTCOME MEASURES
PsA is a chronic inflammatory arthritis that affects 0.3% to 1% of the general population and 5% to > 30% of patients with psoriasis64,65. Moreover, PsA is underdiagnosed in primary care. PsA has a significant effect on patients’ functional status and use of healthcare66,67. Patients with PsA mainly experience progressive joint damage and skin-related physical appearance and symptoms that can severely affect their functional capacity.
Disease Activity
Joint assessment
The presence of inflammatory arthritis is a hallmark of PsA, and the first step in the assessment of PsA is to perform tender and swollen joint counts. For PsA, a TJC of 68 joints [including the distal interphalangeal (DIP) joints of the hands] and SJC of 66 joints (excluding hips) are recommended. Since the joints of the feet are commonly affected in PsA, it is important to include the feet in the joint assessment. A joint count usually takes about 5 min and can be incorporated into daily clinical practice68,69.
In a study that assessed reliability of joint assessment between rheumatologists and dermatologists, there was substantial overall agreement in the TJC (overall ICC 0.78), but only fair agreement on the SJC (overall ICC 0.24)33. Further, the agreement on TJC was excellent among rheumatologists (ICC 0.81) and dermatologists (ICC 0.73), while the assessment of the SJC was less reliable, with ICC among rheumatologists and dermatologists of only 0.42 and 0.31, respectively. Previous studies have demonstrated a higher agreement on SJC among rheumatologists (ICC 0.63)70. These data indicate that additional training might be needed to enable both dermatologists and rheumatologists to better estimate the extent of joint disease (see Figure 5 for homunculus). However, it is unlikely that dermatologists would perform joint examinations in daily practice.

Homunculus for swollen joint count for 68 joints. Hips cannot be assessed for swelling (66 joints).
Dactylitis
Dactylitis (Figure 6), reported in 16–45% of patients with PsA, is characterized by the swelling of an entire finger or toe because of synovitis, tenosynovitis, enthesitis, and soft tissue edema71,72,73. Traditionally, it has been assessed by having the investigator examine each digit and determine if it is swollen or not. A quantitative dactylitis measure, the Leeds Dactylitis Index (LDI), has been developed72. The LDI combines circumference of the affected fingers, circumference of contralateral fingers, and tenderness of affected fingers in 1 score (Figure 7)72. To obtain the LDI score, the circumference of the affected digits is measured either with a tape or precalibrated dactylometer loop at the level of the proximal phalanx (a Leeds Dactylometer could be purchased at www.mie-uk.com/dactylometer/index.html). As a comparison, the circumference of the contralateral digit at the same level is measured and if the contralateral digit is involved, the appropriate value from Table 3 can be used. For an accurate measurement, the affected digit should be squeezed with moderate pressure (enough to blanch the examiner’s nailbed). Responses should be recorded for each digit as follows: 0 = no tenderness, 1 = tender, 2 = tender and wince, and 3 = tender and withdraw. The sum of each digit will equal the total score, and a higher score is associated with worse dactylitis. This measure has been proven reliable among rheumatologists in both the International SPondyloarthritis Interobserver Reliability Exercise and the International Multicenter Psoriasis and Psoriatic Arthritis Reliability Trial (IMPART) study, but not dermatologists in the IMPART study33,74.

Dactylitis.

Leeds Dactylitis Index72. Dactylitis score sheet. From Helliwell, et al. J Rheumatol 2005;32:1745–50; with permission.
Leeds Dactylitis Index72. Normative data for men and women (in mm). From Helliwell, et al. J Rheumatol 2005;32:1745–50.
Enthesitis
Enthesitis, present in about 30–50% of patients with PsA, is characterized by inflammation at sites of tendon, ligament, and joint capsule fiber insertion into bone75,76. Although classically depicted as involving the Achilles tendon and plantar fascia insertion sites, enthesitis can be present at any insertion site. Several enthesitis scoring measures have been developed, all involving a standard palpation approach (e.g., applying ∼4 kg/cm2 of pressure, enough to blanch the tip of the examiner’s fingernail) and determining the tenderness.
The Mander Enthesis Index (MEI) was originally developed to assess all clinically accessible and relevant enthesitis points (66 in total)77. However, it has been criticized for the large number of sites examined, rendering it too complicated and time consuming for use, even in clinical trials. The MEI is often referred to for the purpose of describing the overall set of potential enthesitis sites from which other simpler measures have been developed. For example, the Leeds Enthesitis Index (LEI) assesses only 6 entheseal sites78, the Spondyloarthritis Research Consortium of Canada (SPARCC) Enthesitis Index involves 18 sites79, and the Maastricht Ankylosing Spondylitis Enthesis Score examines 13 sites70. The SPARCC and LEI were found to be most reliable in PsA (ICC 0.81)74. The LEI appears to be the easiest to implement and correlates well with disease activity78.
Spine disease
The spinal manifestations of PsA tend to be less severe than those seen in ankylosing spondylitis (AS)80. Because spine involvement tends to be mild and inconsistent, it has not been systematically assessed in clinical trials of PsA. The measures of axial disease developed for AS — the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), Bath Ankylosing Spondylitis Function Index (BASFI), and Bath Ankylosing Spondylitis Metrology Index — are reasonably reliable, responsive, and discriminative for PsA as well as AS81.
Imaging techniques
Imaging techniques such as magnetic resonance imaging (MRI) and ultrasound (US) have been increasingly used in PsA. These modalities can be used to aid diagnosis and to follow outcomes of treatment. The Outcome Measures in Rheumatology Clinical Trials (OMERACT) MRI in inflammatory arthritis group have developed a scoring system for PsA MRI (PsAMRIS)82,83. The joints scored in the PsAMRIS are metacarpophalangeal, proximal interphalangeal, and DIP of fingers 2–5. These joint regions were divided by the midpoints of the phalangeal bones and were then subdivided at the joint space line to give 3 joint regions and 6 subregions (Figure 8)83. The score is time consuming to perform and has not yet been used in clinical trials, although it has been tested in multiple validation exercises. The current involvement of US in PsA has focused on pathogenesis, including bone abnormalities (erosions, enthesophytes, and new bone formation/periosteal reaction). It has been used to predict the development of PsA in patients with psoriasis84.
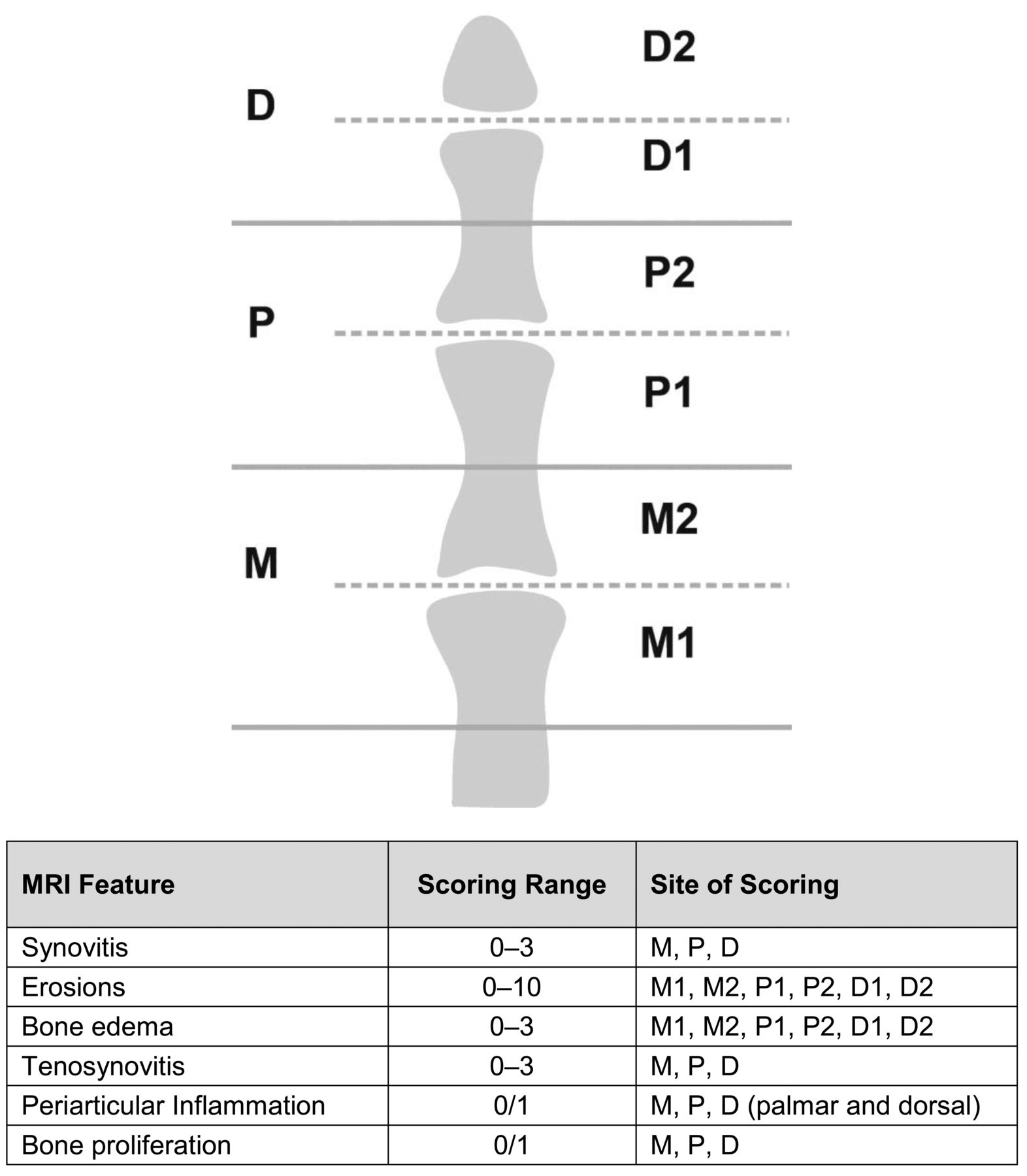
PsAMRIS scoring system83. PsAMRIS: psoriatic arthritis magnetic resonance imaging; D: distal interphalangeal joint region; P: proximal interphalangeal joint region; M: metacarpophalangeal joint region; MRI: magnetic resonance imaging. From Coates, et al. Best Pract Res Clin Rheumatol 2012;26:805–22; with permission.
Physical function (PF)
PF has been reliably assessed in PsA trials by the Health Assessment Questionnaire (HAQ)85. This measure contains 20 items divided into 8 domains (dressing and grooming, arising, eating, walking, hygiene, reach, grip, and common daily activities). Individuals rate the degree of difficulty they have had in the past week on a 4-point scale, ranging from 0 (no difficulty) to 3 (unable to do). The highest scores in each category are summed (0–24) and divided by the number of categories scored to yield a score from 0–386. The limitation of HAQ in PsA is in its inability to adequately identify disability in patients with predominant skin disease.
In a large cohort of patients in the Toronto PsA registry, HAQ scores correlated with the number of inflamed joints (reflecting disease activity) and deformed joints (reflecting damage)87. However, similar to observations from RA, the effect of disease activity on the HAQ declined with duration of disease activity. Leung, et al88 showed that HAQ correlates with other functional indices in PsA (BASFI, Dougados Functional Index, and SF-36-PF). However, SF-36-PF was the best for measuring functional disability in PsA in terms of less floor effect, highest item separation (6.99), reliability (0.85), longest span of item threshold (9.03 logits), less differential item functioning, and better distributional properties88.
Composite measures for PsA
The most commonly used composite measures for PsA are the American College of Rheumatology (ACR) response criteria, the Disease Activity Score (DAS), DAS in 28 joints (DAS28), and the Psoriatic Arthritis Response Criteria (PsARC). The ACR 20% response criterion (ACR20) has typically been used as the primary outcome measure in randomized clinical trials with PsA, and the ACR50 and ACR70, DAS or DAS28, and PsARC have been used as secondary measures. However, these indices evaluate only the joint disease. Recognition that PsA is a complex disease that involves joints, skin, nails, enthesitis, dactylitis, and the spine has led to attempts of developing composite measures of disease activity and response to therapy that take into account most, if not all, these domains. Table 489,90,91,92,93,94,95 provides an overview of several composite measures that have been developed specifically for PsA. These instruments are currently included in clinical trials. While the use of composite measures in daily practice appears to be challenging89,90,91,92,93,94,95, once a patient is properly assessed with an actively inflamed joint count, an assessment of dactylitis, enthesitis, skin, and nails, and the patient completes appropriate PRO measures, it is not difficult to calculate the composite index.
Composite measure specific to PsA.
PRO and Available Tools
Because of the added burden of arthritis, patients with PsA have more functional disability and reduced QoL compared with patients with psoriasis without arthritis96. Assessment of QoL in patients with PsA is important to assess the effect of the disease on the patient’s life, monitor response to therapy, and to identify areas that need improvement. Two validated PsA-specific tools include the Psoriatic Arthritis Quality of Life (PsAQoL) and the Psoriatic Arthritis Impact of Disease (PsAID) questionnaires. The PsAQoL, the most commonly used PsA-specific HRQOL instrument in clinical trials, includes 20 items and takes about 3 min to complete97. In an assessment of sensitivity and response to change, the PsAQoL showed a significant change from baseline at both 3 months (p < 0.01) and 6 months (p < 0.05)98. Tezel, et al99 found the PsAQoL to be moderately to weakly correlated with disease activity measures [DAS28, DAS for reactive arthritis, BASDAI, Ankylosing Spondylitis Disease Activity Score-C-reactive protein (CRP)], pain, and enthesitis. The PsAID includes 2 versions (PsAID-9 and PsAID-12) of a patient-derived weighted questionnaire for assessing the effect of PsA on patients’ QoL100. The PsAID-9 is viewed as an instrument for the assessment of PsA in clinical trials and the PsAID-12 can be valuable in clinical practice, both for identification of areas that should be addressed in clinical management and for monitoring patients longitudinally. However, further validation of the PsAID score is needed, in particular regarding sensitivity to change in comparison with other outcome measures in PsA.
PtGA is included among the core domains for the assessment of PsA by OMERACT101. The intent of the PtGA is to evaluate the effect of disease activity on the patient’s QoL, taking into consideration treatment side effects, among other items. The PtGA for PsA includes 3 self-reported questions that assess102 (1) The overall effect of the disease: In all the ways in which your PSORIASIS and ARTHRITIS, as a whole, affect you, how would you rate the way you felt over the past week? (2) The effect of joint disease: In all the ways your ARTHRITIS affects you, how would you rate the way you felt over the past week? (3) The effect of skin disease: In all the ways your PSORIASIS affects you, how would you rate the way you felt over the past week? The responses are identified on a 100-mm VAS scale. All 3 measures demonstrated good test–retest reliability; ICC was 0.87 for overall effect of the disease, 0.86 for the effect of joint disease, and 0.78 for skin disease.
Another important PRO in PsA is fatigue, which is increasingly recognized as a significant clinical domain in PsA, and was recently included in the OMERACT core domain set for PsA. Fatigue is independent of, and not fully explained by, other domains such as pain, TJC, SJC, PtGA, and function103. The Functional Assessment of Chronic Illness Therapy–Fatigue (FACIT-F) scale was originally developed to assess fatigue associated with anemia104,105. It consists of 13 items and answers are based on a 4-point Likert scale. Total score ranges from 0 to 52 with high scores representing less fatigue. The tool has been validated in the general population106, in patients with cancer105, in patients with RA107, and in patients with PsA108.
The Modified Fatigue Severity Scale (mFSS) includes 9 items that ask about the extent to which fatigue influences motivation, exercise, physical functioning, duties and responsibilities, work, family, and social life. Patients rate each item on a scale from 0 (not at all) to 10 (entirely)109. A higher score indicates more severe dysfunctional fatigue. To that end, moderate to severe fatigue is defined by mFSS scores ≥ 5, and severe fatigue is defined by mFSS scores ≥ 7. Data from the Toronto PsA cohort demonstrated good correlation between the FACIT-F and the mFSS108.
Fatigue is also associated with reduced work productivity. Walsh, et al110 analyzed the relationship between fatigue and work productivity loss (WPL) in 107 people with PsA. The study shows that work productivity was reduced by 6.7% compared with benchmark employees without limitations. Fatigue was reported by 54 patients (50.5%) on the PsAQoL (question #1), and 64 (60.0%) were classified as high fatigue by the BASDAI (question #1). The WPL was associated with fatigue, as measured by the PsAQoL (question #1; p = 0.01) and the BASDAI (question #1; p = 0.002).
Considerations for Remission and MDA
Several studies have used RA remission criteria to evaluate the ability to achieve remission or low disease activity in PsA. Although some of these studies suggest that it may be less difficult to aim for sustained remission in PsA compared with RA111,112, it is important to keep in mind that these groups have used “joint-centered” definitions of remission, which may be a less comprehensive approach to the evaluation of PsA. This prompted the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis to initiate a project led by Coates and Helliwell113 to construct a PsA-specific definition of MDA (Table 5). It has been demonstrated that patients with active PsA who achieved MDA with effective therapy have a significant reduction in radiographic progression114. Several studies demonstrated the effect of weight and/or obesity on the achievement of MDA114,115,116 and found that obesity is associated with a higher risk of not achieving MDA114,115, and weight loss ≥ 5% was a predictor of the achievement of MDA116. Several studies also demonstrated that treatment with antitumor necrosis factor (TNF) agents can lead to MDA in a majority of patients with PsA117,118. Achievement of MDA with biologic therapy is associated with less radiographic progression119. Patient age, CRP, and BASFI at the beginning of treatment were found to be reliable predictors of achieving MDA after 3 months of TNF-α blocker therapy120. Achievement of MDA at 3 months was inversely predicted by age (OR 0.896, p = 0.003) and BASDAI (OR 0.479, p = 0.007), and directly predicted by CRP (OR 1.78, p = 0.018).
Minimal disease activity criteria in PsA113. Minimal disease activity in PsA is defined as achievement of at least 5 of the 7 following criteria.
Considerations for Canadian Daily Practice
Assessment of joints for swelling (66 joints) and tenderness (68 joints) should be the key components of clinical evaluation in patients with PsA
Because it takes a long time for radiographic progression to be demonstrated by radiographs, MRI and/or US should be considered in patients with suspected disease progression (e.g., patients with symptomatic joints) or where there are discrepancies between physician findings and patient reports
To objectively assess dactylitis and enthesitis, we recommend the 2 Leeds indices (LDI and LEI) because they are simple and easy to implement
One should keep in mind that the 3 most common and important enthesitis sites from the patient perspective are (1) Achilles insertion, (2) lateral epicondyle, and (3) plantar fascia insertion121. These sites are more likely to cause functional limitation and have an effect on patient QoL and daily living. Moreover, dactylitis is not included in the definition of MDA because its effect can be detected and assessed during regular joint examination (there are 3 joints affected in a dactylitis digit, thus dactylitis could prevent a patient from achieving an MDA state).
For the assessment of skin involvement, the PASI, PGA, or BSA should be used
Although it has been demonstrated that achievement of MDA will lead to reduction in radiographic progression, the effect of achieving MDA on other longterm outcomes, including the effect on comorbidities, has yet to be confirmed.
PRELIMINARY TREAT-TO-TARGET RECOMMENDATIONS FOR MANAGING PSORIASIS AND PSA IN CANADIAN DAILY PRACTICE
Overarching Principles
The Steering Committee believed that certain aspects relating to the treatment of psoriasis and PsA should form the basis of a framework for specific recommendations. The following items were therefore considered as overarching principles:
A PsA patient with psoriasis should ideally be comanaged by a rheumatologist and dermatologist
T2T will assist in achieving beneficial longterm outcomes:
Reduction in comorbidities (i.e., depression, CVD, diabetes, hepatic steatosis)
Prevention of joint destruction and improvement in productivity and functioning
Physicians and patients must be in agreement with the selected treatment plan
Patient satisfaction with the selected treatment is key to successful outcomes
Targets must be attainable, manageable, and easy to assess in clinical practice
Physicians must follow the evolution of conditions and adjust treatment in accordance with the response to reach therapeutic targets:
Assessment every 3 months for patients with active disease
Assessment every 6 to 12 months for patients with stable disease (when therapeutic targets are reached).
T2T Recommendations
The overarching principles are followed by the preliminary set of 8 recommendations as formulated by the expert Steering Committee (see Table 6 for summarized version).
Summary of preliminary treat-to-target recommendations.
Recommendation 1
A state of clear or almost clear skin should be a therapeutic target for psoriasis regardless of the area affected (e.g., nails, scalp, soles, palms, trunk, extremities, etc.) and the duration of disease (early vs late disease). It should be emphasized that a state (clear or almost clear) is considered a therapeutic target as opposed to the degree of improvement in disease (e.g., reaching PASI 75). With regard to outcome measures for defining a state of clear or almost clear skin, either PASI ≤ 3, BSA ≤ 1, or a PGA ≤ 1 is acceptable.
Recommendation 2
Because a state of remission may be difficult to reach in PsA, a state of MDA is an acceptable therapeutic target. The definition of MDA should be based on TJC ≤ 1 (based on 68-joint count), SJC ≤ 1 (based on 66-joint count), PASI ≤ 1 or BSA ≤ 3 (dermatologists thought that it should be PASI ≤ 3 or BSA ≤ 1), PGA ≤ 1, HAQ of 0.5, and entheseal sites ≤ 11. PRO (patient pain VAS ≤ 15, patient global activity VAS ≤ 20) and measures of QoL (e.g., DLQI ≤ 5) should be taken into consideration.
Recommendation 3
QoL is an important outcome from the patient and physician perspective and should be included in therapeutic targets. Patient satisfaction is crucial to successful longterm disease management. Thus, PRO are important and should be included in therapeutic targets. Any validated PRO measure is acceptable, including PtGA and DLQI, especially since clinical trials have confirmed the correlation between these 2 outcomes. DLQI ≤ 5 is a preferred target for psoriasis.
Recommendation 4
Functional impairment, comorbidities, and treatment risks should be considered when making clinical decisions in addition to assessing measures of disease activity. Psoriasis and PsA are associated with several comorbidities, including CVD, GI disease, metabolic syndrome, and psychiatric manifestations (e.g., depression, anxiety, fatigue). Further, severe psoriasis is associated with an increased risk of premature death, mainly from CV causes. Thus, proper management of comorbidities and collaboration between different specialists are key to disease control and successful outcomes.
Recommendation 5
Physicians and patients must be in agreement regarding selected therapeutic targets, taking into consideration initial severity of disease and the appropriate time frame to reach this target. It is paramount that a treating clinician defines the target with the patient, directs the strategy chosen, and follows the patient over time. Because there may be challenges informing some patients about the need for intensive medication, or the necessity to adjust therapy (e.g., patients with relatively mild symptoms), educational initiatives targeted for patients may be required.
Recommendation 6
Patients must be treated adequately to reach the selected therapeutic targets, with therapy adjustments every 3 months for patients with active disease and every 6 to 12 months for those with stable disease (when therapeutic targets are reached). The benefits of tight control in PsA have been established in the Tight Control of Psoriatic Arthritis trial122,123. In addition, the 2014 Canadian needs assessment survey revealed that community clinicians are in agreement with this recommendation and considered this time frame reasonable and applicable to their daily practice.
Recommendation 7
Once reached, the state of clear or almost clear skin should be maintained for as long as possible with adjustment in therapy at the first signs of disease progression. As reactivation of the disease could lead to reduced QoL and disability, patients who flare/deteriorate during followup should be promptly reassessed. Thus, if a therapy is halted, for whatever reason, it is imperative to ensure frequent followup, monitoring, and reinitiation of treatment at the first sign of disease progression.
Recommendation 8
Standard safety assessments should be performed at each visit. Safety assessments should include tolerability of selected therapy, as well as the effect of therapy on other organ systems. When appropriate and as needed, patients should be referred to other specialists for further evaluation.
Acknowledgment
Radmila Day of SNELL Medical Communication prepared a draft outline manuscript for authors’ comment and approval, and subsequently supported incorporation of comments into final drafts for authors’ approval, and editorial styling required by The Journal. AbbVie paid SNELL Medical Communication Inc. for this work.
Footnotes
Sponsored by AbbVie Canada.
As a supplement, this report was reviewed internally and approved by the Guest Editors for integrity, accuracy, and consistency with scientific and ethical standards.
REFERENCES
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵
- 104.↵
- 105.↵
- 106.↵
- 107.↵
- 108.↵
- 109.↵
- 110.↵
- 111.↵
- 112.↵
- 113.↵
- 114.↵
- 115.↵
- 116.↵
- 117.↵
- 118.↵
- 119.↵
- 120.↵
- 121.↵
- 122.↵
- 123.↵








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}