

Abstract
Objective. The objective of this study was to identify risk factors for a relapse at the time of an increase in antineutrophil cytoplasmic antibodies (ANCA) in patients with renal ANCA-associated vasculitis (AAV).
Methods. All patients between January 2000 and November 2011 with renal AAV having an ANCA rise during remission were included. Differences in time to relapse since the ANCA rise were assessed using a Cox regression model. The level of 25-hydroxy Vitamin D (25(OH)D) was assessed at the ANCA rise and at a subsequent relapse or time-matched during remission.
Results. Sixty patients had an ANCA rise, of whom 36 patients relapsed. Three risk factors were associated with a relapse at the time of the ANCA increase: previous disease activity not treated with cyclophosphamide or rituximab (HR 3.48, 95% CI 1.60–7.59), an ANCA rise during the fall season (HR 4.37, 95% CI 1.60–11.90), and an extended ANCA rise (HR 3.57, 95% CI 1.50–8.48). Levels of 25(OH)D significantly decreased during followup in relapsing patients, but not in patients who remained in remission (difference −6.3 ± 14.4, p = 0.017 vs 2.7 ± 16.3, p = 0.430).
Conclusion. ANCA rises occurring during the fall season are more frequently followed by a relapse than ANCA rises occurring during other seasons. Although it is tempting to speculate that decreasing Vitamin D levels following the ANCA rise can be held responsible for the subsequent relapse, this remains to be determined.
- ANTINEUTROPHIL CYTOPLASMIC ANTIBODIES
- ANCA-ASSOCIATED VASCULITIS
- GRANULOMATOSIS WITH POLYANGIITIS
- SEASON
- VITAMIN D
- FOLLOWUP STUDY
Antineutrophil cytoplasmic antibodies (ANCA) are involved in the pathophysiology of ANCA-associated vasculitis (AAV)1. The use of an ANCA rise to predict relapses, however, is a subject for debate2,3,4,5,6. An ANCA rise has previously been used to guide preemptive immunosuppressive treatment to prevent a relapse4. But the use of such a strategy raises concerns over unnecessary exposure to treatment-related side effects, because only a proportion of patients develop a relapse after an ANCA rise3,4,5,6,7,8. Previously, we have shown that ANCA rises are associated with relapses in patients with renal involvement, but not in patients with nonrenal disease8. In our current study, we further elaborated on potential risk factors. Hereto, we include only patients with renal involvement who have an ANCA rise during remission.
Patients with renal involvement are nearly always ANCA-positive, whereas a positive ANCA titer is less often found in patients with nonrenal disease9. From our experience, the presence of ANCA seems necessary for severe disease activity, because all patients were ANCA-positive at the time of a major relapse8. Major relapses can still occur when patients are ANCA-negative, however6,10, and a small subgroup of patients with pauciimmune glomerulonephritis are ANCA-negative11. Yet not every ANCA rise leads to disease reactivation; many rises are not followed by a relapse. We hypothesize that a “second hit” may be required to create a proinflammatory environment that enables the ANCA to become pathogenic. In the second-hit hypothesis, ANCA-induced (severe) disease reactivation is enabled by or aggravated by an as-yet unidentified factor, or second hit. This hypothesis is substantiated by animal models, in which the priming of neutrophils by bacterial lipopolysaccharide is required for antiproteinase 3 antibody (PR3)–induced alveolar hemorrhage and glomerulonephritis12, and aggravates antimyeloperoxidase antibody (MPO)–induced glomerulonephritis13. Several candidates for this second hit have been postulated, such as microorganisms14, environmental factors15,16, and/or other autoantibodies17. We hypothesize that Vitamin D may also be important, because it is a major immune-modulating agent18. In other autoimmune diseases, such as multiple sclerosis and systemic lupus erythematosus, associations have been observed between low levels of 25-hydroxy Vitamin D (25(OH)D), the inactive metabolite of Vitamin D, and disease progression or reactivation19,20,21. However, the involvement of Vitamin D in AAV has not been elucidated. It has been shown that levels of 25(OH)D are lower in patients with AAV compared with healthy controls, but no studies have been published concerning the relation between 25(OH)D and the risk of a relapse in patients with AAV22.
In our current study, we investigated risk factors for a relapse at the time of an ANCA rise to gain insight into potential second hits that are required for disease reactivation. In particular, we focused on seasonal influences, such as 25(OH)D levels at the time of the ANCA rise and at the time of a subsequent relapse or time-matched during remission.
MATERIALS AND METHODS
Inclusion criteria for patients
All patients who visited the clinic at the Maastricht University Medical Center between January 1, 2000, and November 1, 2011, were evaluated. Inclusion criteria were a diagnosis of AAV23, previous renal involvement, and a rise in PR3- or MPO-ANCA during remission8.
Classification of patients
Patients were subclassified using the European Medicines Agency classification into granulomatosis with polyangiitis (GPA), microscopic polyangiitis (MPA), or eosinophilic GPA (EGPA; Churg-Strauss syndrome), and patients with EGPA were subsequently excluded23,24. Renal involvement was preferably determined by a kidney biopsy showing pauciimmune–necrotizing glomerulonephritis25,26. However, surrogate markers such as hematuria in combination with red cell casts, dysmorphic erythrocytes (> 10), and/or proteinuria sufficed24.
All patients have been treated according to the European League Against Rheumatism guidelines7,26. Regarding the treatment of the previous period with disease activity, we grouped therapy consisting of cyclophosphamide (CYC; oral or intravenous) or rituximab (RTX) as “induction regimen with CYC/RTX.” Other therapies [e.g., methotrexate (MTX) or mycophenolate mofetil] were grouped as “induction regimen lacking CYC/RTX.” Current immunosuppressive treatment was classified as “immunosuppressive therapy” if the ANCA rise occurred when the patient was treated with any form of immunosuppressive agent or as “no immunosuppressive therapy” if no immunosuppressive therapy was taken. Antibiotic therapy was classified as antibiotic maintenance therapy or as no antibiotic maintenance therapy (short courses of antibiotics were allowed). Patients were defined as persistently ANCA-positive when ANCA values remained positive during followup and as nonpersistently ANCA-positive when an ANCA measurement had at least once been negative. The season during an ANCA rise in the Netherlands is defined as winter during December to February, spring during March to May, summer during June to August, and fall during September to November27.
Disease activity state
A relapse was defined as reoccurrence or new onset of disease attributable to active disease combined with an increase or addition of immunosuppressive treatment3,4,8,28,29. Relapses were further subdivided into minor or major, depending on whether the relapse was potentially organ- or life-threatening29. For a renal relapse, the (re)occurrence of hematuria in combination with a rise in serum creatinine of 25% was required to be characterized as a major relapse.
Followup
Patients were routinely screened for potential symptoms of a relapse and blood was drawn8. Antigen-specific, solid-phase ANCA tests were performed for the detection and quantification of PR3- and MPO-ANCA. Initially, commercially available direct PR3- and MPO-ANCA ELISA were used (Euro Diagnostica)30. On October 1, 2005, this assay was replaced by a fluorescent-enzyme immune-assay (FEIA) for PR3- and MPO-ANCA (EliA, Thermo Fisher)31. During the transition, ANCA measurements were performed by both methods.
In addition, ANCA were detected by indirect immunofluorescence (IIF) on ethanol-fixed neutrophil granulocytes (INOVA Diagnostics)31. Samples were diluted serially in phosphate buffered saline starting at 1:16.
Clinical characteristics were recorded in all subjects according to the Dutch law on Medical Treatment Act, the Personal Data Protection Act, and the Code of Conduct for Health Research32. Ethics approval was waived by our local ethics committee.
Definition of an ANCA rise
For the detection of an ANCA rise, the value was compared to all measurements made with the same assay in the past 6 months. Next to ANCA rises as detected by antigen-specific assays, we additionally investigated ANCA rises as detected by the IIF technique. For the IIF, a rise was defined as a 4-fold increase2. For the antigen-specific, solid-phase assays, we defined a rise using the slope of an increase as previously described8, thereby taking into account the relative increase (in %) and the time between measurements (in days). A receiver-operating characteristics curve was calculated to determine the optimal cutoff value of the slope. The chosen cutoff values as determined by the ELISA and FEIA methods were 2.56%/day and 2.25%/day, respectively. This is equivalent to a relative increase of 78% and 68% over 1 month or 233% and 205% over 3 months. An ANCA increase was defined as an extended rise when the next sample after the ANCA increase continued to rise.
To ensure that small elevations were above the intraassay coefficient of variation, a rise had to constitute to a relative increase of at least 25% and an absolute increase equivalent to a doubling of the lowest value of a borderline result (at least 10 AU for the ELISA and 5 U/ml for the FEIA). Because our analysis is focused on patients in remission, only serum samples drawn at least 3 months after the previous disease activity were eligible for detection of an ANCA rise8. An ANCA rise was defined as an extended ANCA rise if the next sample was also rising.
Assay of 25(OH)D and serum selection
Quantification of 25(OH)D was performed using the automated LIAISON 25-OH Vitamin D TOTAL assay (DiaSorin). A serum sample was selected at the time of the ANCA rise in all patients. A second sample was selected at the time of the relapse in relapsing patients, or time-matched during remission in patients who remained in remission. If serum was no longer available at the ANCA rise or relapse, a sample 1 month prior or after the ANCA rise or relapse was selected. Circulating 25(OH)D levels above 75 nmol/l (30 ng/ml) were considered sufficient, according to international guidelines33.
Statistical analysis
Numerical variables were expressed as mean (± SD) or median (interquartile range), and categorical variables as numbers (%). Associations were presented as HR with 95% CI. A p value ≤ 0.05 was considered significant. All statistical analyses were performed using GraphPad Prism version 6.04 for Windows (GraphPad Software) and SPSS statistics for Windows, version 23.0 (IBM).
Differences in baseline patient characteristics were investigated using the chi-square test for categorical variables and the Mann-Whitney U test for continuous variables. Two paired columns were compared using the paired Student t test. Two unpaired columns were compared with the Mann-Whitney U test.
The time to relapse was estimated using the Kaplan-Meier method. An event was defined as a relapse at the time of the start or increase of immunosuppressive treatment. Subjects were censored at the time of death, last ANCA measurement, or closure of study. Univariate analyses were performed using the log-rank test for categorical variables and a Cox regression model for continuous variables. HR for categorical variables were derived from a Cox regression model. All variables with a p value ≤ 0.05 according to the univariate analysis were included in a multivariate analysis using a Cox regression model. The proportional hazards assumption was assessed by Schoenfeld residuals and by visually inspecting log-log plots; variables were included as a time-dependent variable if the assumption was violated.
Several risk factors for a relapse at the time of remission have been described in the literature. However, no analyses have been performed at the time of an ANCA rise. Therefore, several variables were assessed that were thought to be clinically relevant. Included variables were age, sex, diagnosis, ANCA serotype, ENT involvement, Birmingham Vasculitis Activity Score (BVAS; v3), induction regimen at previous disease activity, persistence of ANCA positivity during followup, the time between previous disease activity and the rise, the season in which the rise occurs, the slope of the rise, the value of the rise, whether the rise is extended, 25(OH)D level, current immunosuppressive treatment, antibiotic maintenance therapy, and the existence of a concomitant rise in the IIF titer.
RESULTS
Patient characteristics and outcome
Sixty patients were included at the time of an ANCA rise (Table 1). Fifty-one patients (85%) were PR3-ANCA–positive and 9 patients were MPO-ANCA–positive. Fifty-five patients (91.7%) had GPA, while the remaining 5 patients had MPA. Thirty-six patients relapsed: 20 major relapses [BVAS 17 (15–19)] and 16 minor relapses [BVAS 7 (4–13)]. Relapses occurred after a median of 6 months (2–13) since the ANCA rise.
Patient characteristics. Values are median (interquartile range) or as the n (%).
Risk factors of a relapse
We observed that a rise during the fall season was highly associated with a relapse (HR 4.37, 95% CI 1.60–11.90; Figure 1A; see Table 2 for the results of the univariate analysis). Also, 2 other risk factors were significantly associated with a relapse: an induction regimen at previous disease activity lacking CYC or RTX (HR 3.48, 95% CI 1.60–7.59) and an extended ANCA rise (HR 3.57, 95% CI 1.50–8.48). All 3 risk factors remained significantly associated with a relapse according to the multivariate analysis (Table 3).
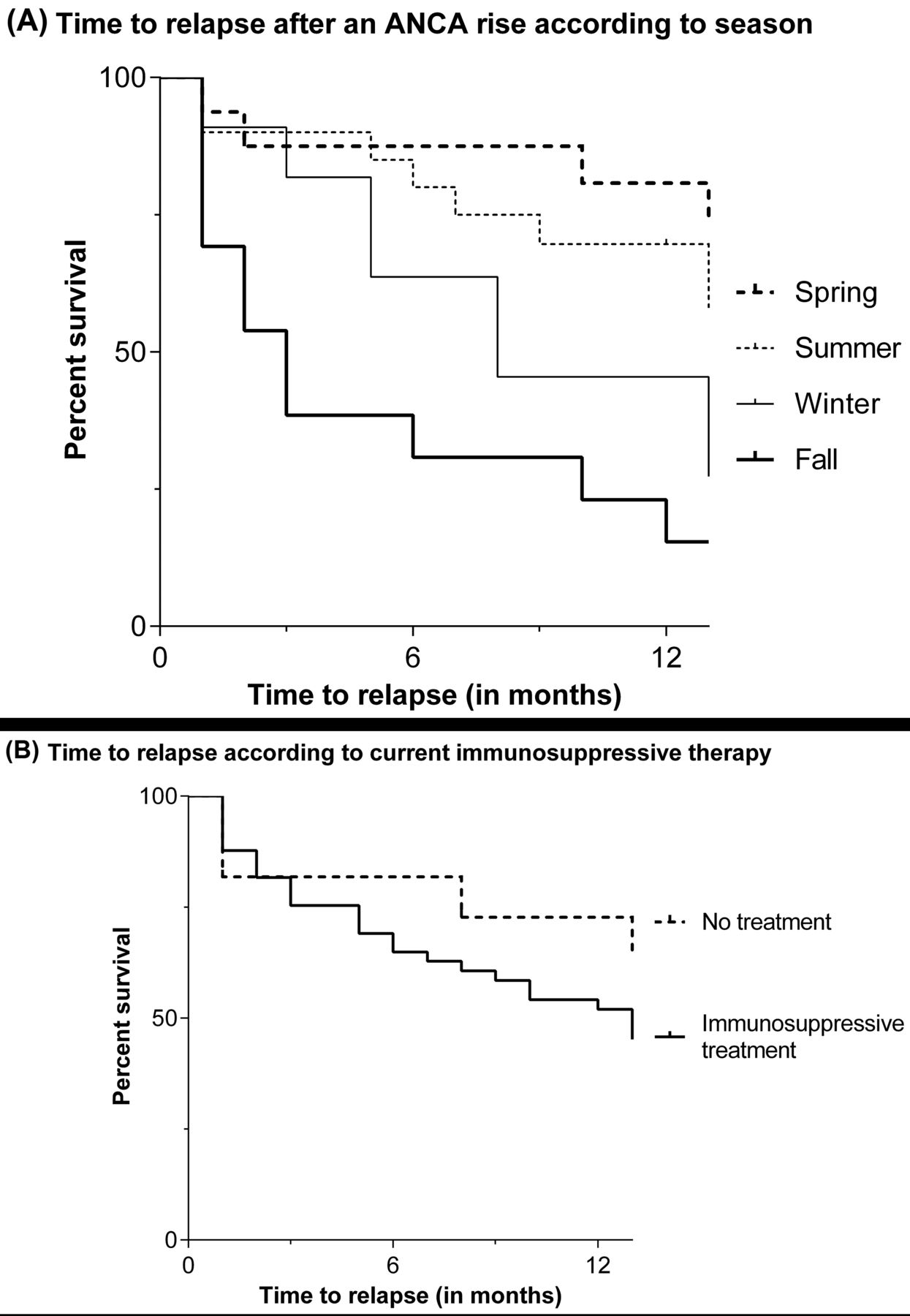
Time to relapse after an ANCA rise according to (A) season (chi-square = 12.383, p = 0.006) and (B) current immunosuppressive therapy (chi-square = 1.173, p = 0.279). ANCA: antineutrophil cytoplasmic antibodies.
Results of the univariate analysis of risk factors for a relapse from the time of an ANCA rise. Differences were assessed using the log-rank test for categorical variables and a Cox regression model for continuous variables.
Results of the multivariate analysis of risk factors for a relapse from the time of a rise in antineutrophil cytoplasmic antibodies.
In 13 patients, the ANCA rise occurred during the fall season, of whom 9 (69.2%) and 11 patients (84.6%) relapsed within 6 and 12 months, respectively. The proportion of patients who relapsed increased if the next ANCA measurement demonstrated a further rise: 7 of 9 (77.8%) after 6 months and 9 of 9 (100%) after 12 months (Table 4).
The proportion of relapsing patients within 6 and 12 months since the ANCA rise by number and type of risk factor.
Maintenance therapy
Forty-nine patients were taking immunosuppressive therapy at the time of the ANCA rise, while 11 patients no longer used any immunosuppressive agent at the time of the ANCA rise. Immunosuppressive treatment did not protect patients from a relapse following an ANCA rise (chi-square = 1.173, p = 0.279; Figure 1B). In addition, glucocorticoid therapy also did not significantly influence the HR for a relapse after an ANCA rise (Supplementary Data available with the online version of this article).
Thirty-nine of 60 patients were receiving antibiotic maintenance therapy at the time of the ANCA rise. Antibiotic maintenance therapy also did not protect patients from a relapse (chi-square = 0.010, p = 0.922).
Levels of 25-hydroxy Vitamin D
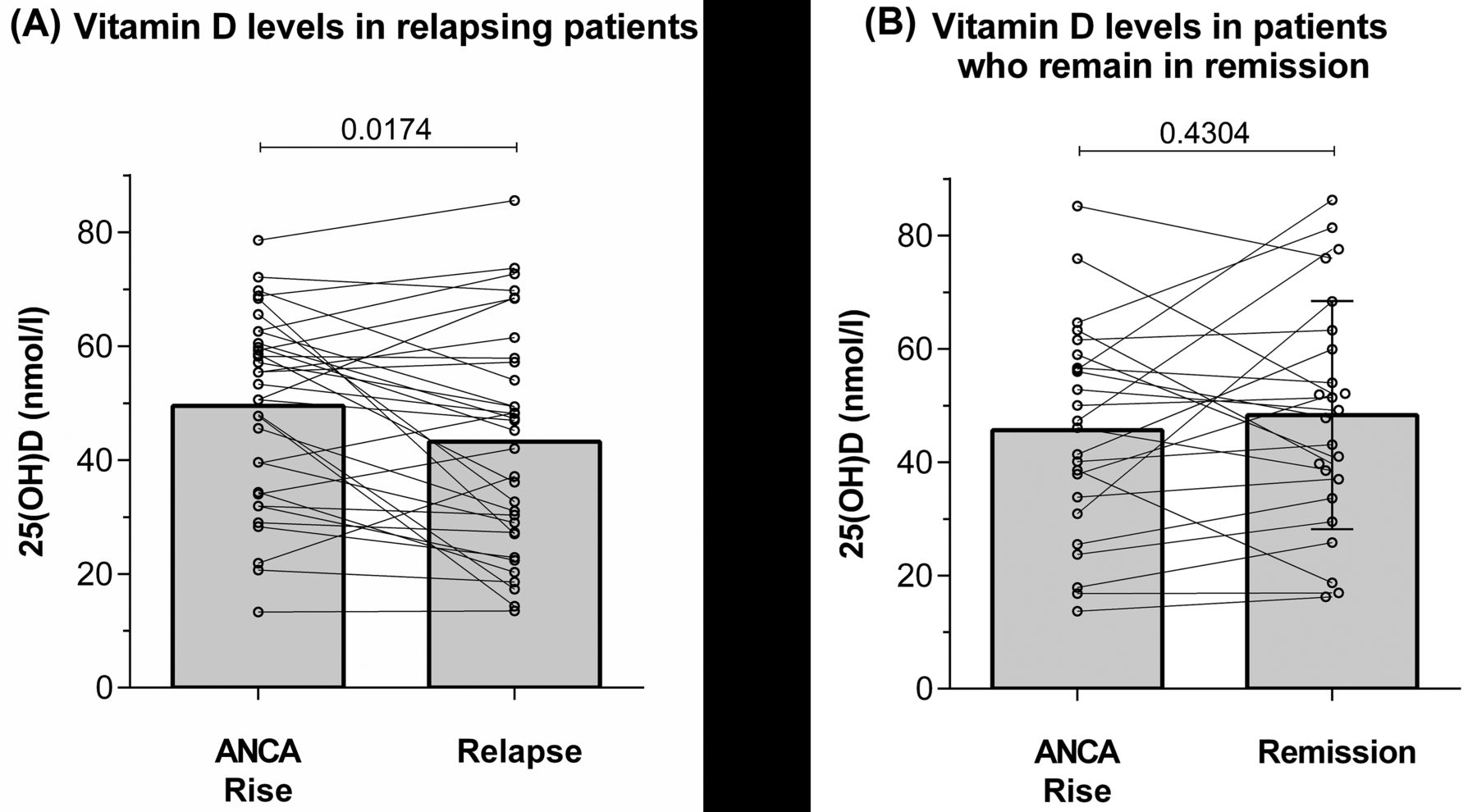
In 58 of 60 patients (97%), a serum sample was still available at the time of the ANCA rise. Four patients had sufficient levels of 25(OH)D, while 54 had insufficient 25(OH)D levels. At the ANCA rise, there was no difference in 25(OH)D levels between relapsing patients (49.5 ± 16.6 nmol/l) and patients who remained in remission (45.6 ± 18.7 nmol/l, p = 0.415).
Paired samples were available in 57 of 60 patients (95%). In relapsing patients, the 25(OH)D level was significantly lower at the time of the relapse compared with the time of the ANCA rise (difference −6.3 ± 14.4 nmol/l, p = 0.017; Figure 2A), while the 25(OH)D level was slightly higher during followup in patients who remained in remission after the ANCA rise (difference 2.7 ± 16.3 nmol/l, p = 0.430; Figure 2B).
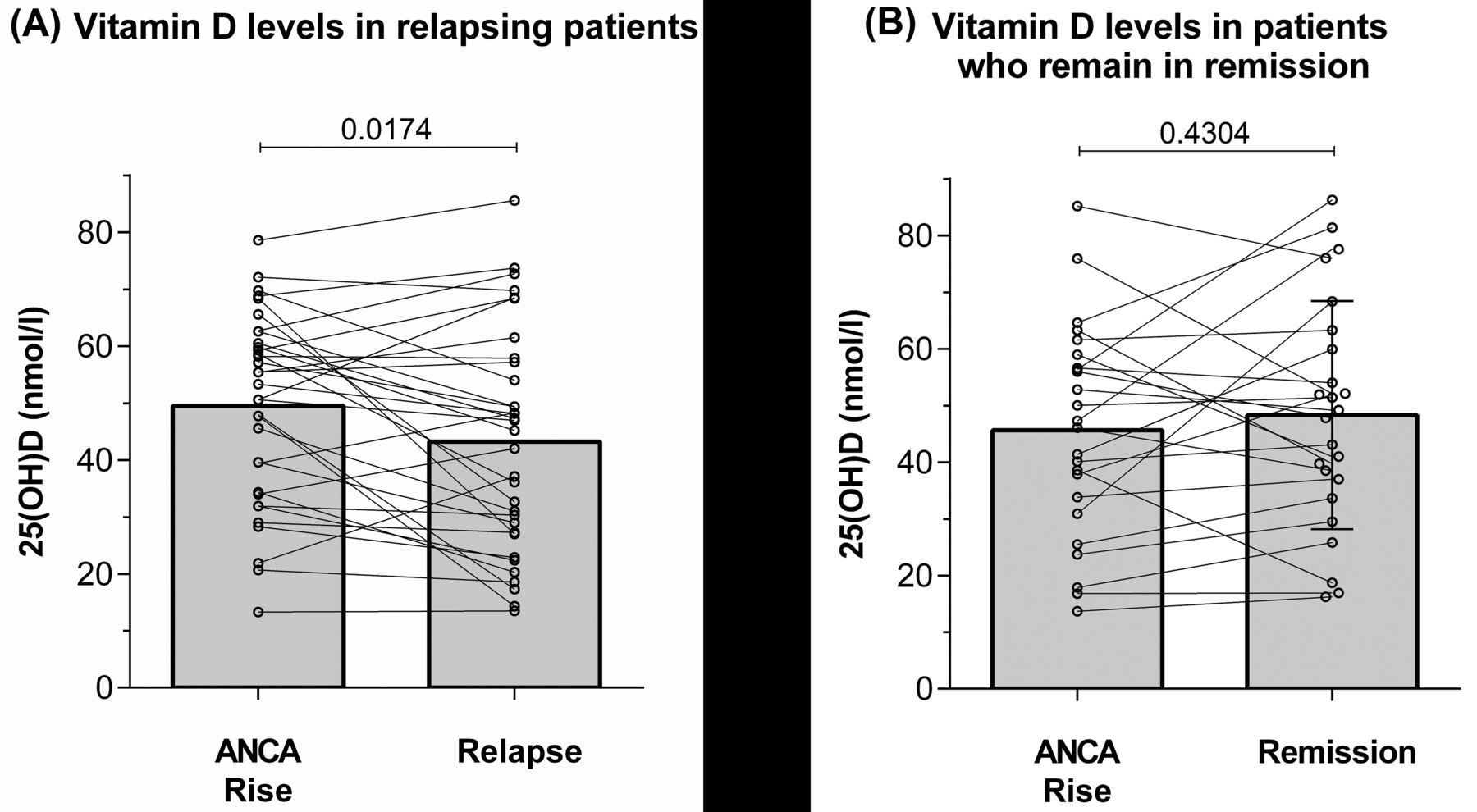
Level of 25(OH)D during followup in (A) patients who relapse after the ANCA rise and (B) patients who remain in remission after the ANCA rise. 25(OH)D: 25-hydroxy Vitamin D; ANCA: antineutrophil cytoplasmic antibodies.
DISCUSSION
In our study, we report risk factors for a relapse at the time of an ANCA rise in patients with renal involvement. Most importantly, we demonstrate that an ANCA rise is most often followed by a relapse when it occurs during the fall season. The level of 25(OH)D significantly decreased after the ANCA rise in relapsing patients, but not in patients who remained in remission.
Several theories have been postulated on the relationship between ANCA and disease reactivation. An ANCA rise may be directly pathogenic. This is unlikely, however, because fewer than half of the patients in whom an ANCA rise occurs will relapse within a year. Therefore, a second hit is probably required5,13. In a mouse model of MPO-ANCA, it has been demonstrated that proinflammatory stimuli of infectious origin and ANCA act synergistically to induce glomerulonephritis13. Our finding that an ANCA rise occurring during the fall season is more often followed by a relapse is in accordance with this hypothesis, because patients in the Netherlands are at increased risk of a respiratory tract infection during the following months34. However, we did not systematically score for infections during followup. Therefore, no objective arguments of an infection were systematically obtained.
Interestingly, however, antibiotic maintenance therapy does not protect against a relapse after an ANCA rise in our current study. This contrasts with previous observations, because it has been shown that cotrimoxazole maintenance therapy is protective of a relapse35. There may be several reasons for this. First, in the study by Stegeman, et al, a high dose of cotrimoxazole (960 mg twice daily) was given, while this was not always the case in our patients35. Second, patients who did not receive antibiotic maintenance therapy were advised to take a short course of antibiotics as soon as symptoms of a possible infection occurred. Third, the antibiotic agent that is taken during antibiotic maintenance therapy may not cover all relevant infections. Therefore, no firm conclusion can be drawn on the influence of antibiotics on the risk of a relapse after an ANCA rise.
Another important seasonal factor is Vitamin D. At the latitude of the Netherlands, the nadir of Vitamin D occurs during the end of the winter, while the level of Vitamin D is at its highest at the end of summer36. It is known that Vitamin D is an important immune-modulating agent18. In vitro studies have shown that Vitamin D skews immune cells toward a more tolerogenic status18. For instance, the proliferation of B cells, an important cell in the pathophysiology of AAV, was inhibited by the active metabolite of Vitamin D (1,25-dihydroxy Vitamin D) in experimental studies37. In vivo, however, the interactions between Vitamin D metabolites and B cells seem to be more complex38. Importantly, associations with disease reactivation have previously been observed in other autoimmune diseases, but not in AAV19,20,21. We demonstrate that a reduction of 25(OH)D upon an ANCA rise is associated with the development of a relapse in AAV. This decrease in patients who will relapse was to be expected, because these patients more often have an ANCA rise during the fall season. Therefore, their levels of 25(OH)D will decrease during the upcoming months according to the seasonal variation of 25(OH)D. However, it is questionable whether the observed changes in Vitamin D are biologically significant. Also, no firm conclusions can yet be drawn concerning the causality of this association. We conclude that patients with AAV may in particular benefit from Vitamin D supplementation during the fall and winter to prevent a disease relapse.
While the quantity of the autoantibody may be important, other factors may be involved5. For instance, epitope specificity, avidity, and the sialylation level of ANCA may contribute to the risk of developing a relapse after an ANCA rise39,40. Therefore, further research on the association between the quality of ANCA at the time of an ANCA rise and disease activity is warranted.
Changes in ANCA level may be related to changes in immunosuppressive treatment41. Importantly, we found that a similar number of patients relapsed after an ANCA rise regardless of whether they were receiving immunosuppressive therapy. We found, however, that patients who were treated during the previous disease activity period with an immunosuppressive regimen lacking CYC or RTX relapsed more often than patients who were treated during the previous disease activity period with CYC or RTX. This finding adds to the growing body of data that suggests that a milder treatment modality, such as MTX, induces a less-stable remission compared with CYC or RTX42.
Our study has several limitations8. In our current retrospective study, physicians were not blinded to ANCA results2,3. Our cohort was mostly composed of PR3-ANCA–positive patients; therefore, our findings may not apply to MPO-ANCA–positive patients. This also holds true for patients with MPA because the majority of our patients had GPA. We have no solid data on the usage of Vitamin D supplements by our patients, because these supplements are readily accessible over the counter. Vitamin D supplementation (500 mg/800 IE) is prescribed to all patients who receive prednisone with a dosage higher than 7.5 mg per day for a period longer than 3 months. No data are available on the vaccination status of our patients, although no increased risk for a relapse was previously observed following a vaccination43. Importantly, we verified that risk factors were specifically associated with both major relapses and minor relapses, as well as renal and nonrenal relapses (Supplementary Data, available with the online version of this article). Our current study is low powered and the lack of precision of our results is obvious in the 95% CI around the estimated HR. This limitation is most evident when only major or renal relapses are studied, as highlighted by the broad 95% CI (Supplementary Data, available with the online version of this article). Yet our findings are significant in a small single-center study and warrant further research in a large, prospective, multicenter study. Genuine and important risk factors may have been missed because of the inadequate power of our study. The risk factors of the relapse identified in our study need to be replicated in more rigorous larger studies in the future. Results from small studies may be affected by a few outliers. We identified 2 outliers who relapsed a very long period after the ANCA rise (73 and 95 mos). However, exclusion of these patients did not change the results (data not shown).
We identified risk factors for a relapse at the time of an ANCA rise in patients with renal involvement. In particular, an ANCA rise occurring in the fall season is an important risk factor for a relapse. We postulate that a subsequent decrease in Vitamin D level may enable proinflammatory skewing of the immune system and can therefore in part be held responsible for this phenomenon. The influence of other factors, such as intercurrent infections and the quality of ANCA on the risk for a relapse after an ANCA rise, should be prospectively studied.
ONLINE SUPPLEMENT
Supplementary material accompanies the online version of this article.
- Accepted for publication December 23, 2016.








{kind=link}
{kind=link}