

Abstract
Objective. To assess the attitudes and strategies of pediatric rheumatology clinicians toward withdrawing medications for children with clinically inactive juvenile idiopathic arthritis (JIA).
Methods. Members of the Childhood Arthritis and Rheumatology Research Alliance (CARRA) completed an anonymous electronic survey on decision making and approaches for withdrawing medications for inactive nonsystemic JIA. Data were analyzed using descriptive statistics.
Results. Of 388 clinicians in CARRA, 124 completed surveys (32%), predominantly attending pediatric rheumatologists. The most highly ranked factors in decision making for withdrawing medications were the duration of clinical inactivity, drug toxicity, duration of prior activity, patient/family preferences, joint damage, and JIA category. Diagnoses of rheumatoid factor-positive polyarthritis and persistent oligoarthritis made respondents less likely and more likely, respectively, to withdraw JIA medications. Three-quarters of respondents waited for 6–12 months of inactive disease before stopping methotrexate (MTX) or biologics, but preferences varied. There was also considerable variability in the strategies used to reduce, taper, or stop medications for clinically inactive JIA; most commonly, clinicians reported slow medication tapers lasting at least 2 months. For children receiving combination MTX-biologic therapy, 63% of respondents preferred stopping MTX first. Most clinicians reported using imaging only seldom or sometimes to guide decision making, but most were also reluctant to withdraw medications in the presence of asymptomatic imaging abnormalities suggestive of subclinical inflammation.
Conclusion. Considerable variability exists among pediatric rheumatology clinicians regarding when and how to withdraw medications for children with clinically inactive JIA. More research is needed to identify the most effective approaches to withdraw medications and predictors of outcomes.
- JUVENILE IDIOPATHIC ARTHRITIS
- PEDIATRIC RHEUMATIC DISEASES
- CLINICAL DECISION MAKING
- CLINICAL INACTIVE DISEASE
The availability of effective synthetic and biologic disease-modifying antirheumatic drugs (DMARD) has improved clinical outcomes in children with juvenile idiopathic arthritis (JIA)1. With these improvements in disease control, clinicians and investigators alike have increasingly aimed for patients with JIA to achieve clinical inactive disease (CID)2,3. CID encompasses a validated composite definition of several clinical factors: no active arthritis, uveitis, or systemic JIA symptoms; the best possible clinical global assessment; inflammatory markers normal or elevated for reasons other than JIA; and no more than 15 min of joint stiffness4. CID is a realistic clinical target for many children in clinical practice1.
Several studies, many small, most retrospective, have studied outcomes of children with JIA who discontinued therapies after achieving inactive disease (variably defined across studies)5,6,7,8,9,10,11,12,13. In multiple studies, discontinuation of biologic therapy with or without concomitant methotrexate (MTX) led to JIA flares in one-half to two-thirds of patients within 1 year5,7,8,11. One small retrospective study (n = 19) suggested that longer durations of medicated remission and medication tapering (vs immediate discontinuation) were associated with improved outcomes5. However, the study did not include patients who flared while tapering, potentially biasing the results. Further, larger, subsequent studies have not replicated those findings, including the lone published randomized trial on medication (MTX) discontinuation in JIA6,8,11. Multiple studies have failed to identify other demographic and disease-specific factors associated with flare after medication discontinuation8,10,11. Two single-center observational studies have shown improved outcomes with strategies of medication reduction (rather than discontinuation): use of low-dose etanercept (ETN)9 and continued biologic use after MTX withdrawal11.
Given the dearth of high-quality evidence of optimal strategies for JIA medication withdrawal and clinical predictors of successful withdrawal, we hypothesized that there would be a wide variability in how clinicians managed JIA in CID (excluding systemic JIA). To test this hypothesis and lay the groundwork for future studies on managing CID, we administered a survey to the Childhood Arthritis and Rheumatology Research Alliance (CARRA).
MATERIALS AND METHODS
Setting, study design, and participants
CARRA is the largest pediatric rheumatology research network in North America. Its members include over 90% of US and Canadian pediatric rheumatologists along with nurse practitioners, trainees, and other associated clinicians and research personnel. As of December 2015, CARRA had a total of 445 members, including 388 clinicians across 110 institutions. Upon enrollment in CARRA, members may affiliate with 1 or several disease-specific committees, including the JIA Committee (43% of CARRA members).
We conducted an anonymous, cross-sectional electronic survey of CARRA members over 4 weeks in November–December 2015. Clinicians who reported taking clinical care of children with JIA were eligible to complete the full survey. Following the initial survey invitation, nonrespondents received up to 2 e-mail reminders to encourage participation.
Study data were collected and managed using the Research Electronic Data Capture (REDCap) tools hosted at Rutgers New Jersey Medical School. REDCap is a secure, Web-based application designed to support data identification for research studies14.
Our study was approved by the Institutional Review Board at Rutgers Biomedical and Health Sciences (Pro20150002424).
Survey
The survey collected anonymous information on participants’ demographics, priorities in making decisions to withdraw JIA medicines for patients with CID, approaches to withdrawing JIA medicines, ancillary testing used in clinical decision making for patients with CID, and self-reported outcomes of patients with CID after stopping medications (Full survey available as supplementary data from the authors on request). Respondents were asked to consider patients with JIA (except systemic JIA) who did not have a history of uveitis, psoriasis (PsO), or inflammatory bowel disease (IBD). In doing so, we sought to reduce the potential complexity of considerations for decision making. For similar reasons, we focused on strategies to taper or stop either MTX monotherapy or biologic monotherapy for most of the survey. Participants were given the option to choose more than 1 preferred strategy for withdrawing medication. The survey used branching logic to tailor questions to participants’ responses. In addition to multiple choice questions, participants were given the option to write about additional factors that were important in decision making and to clarify or elaborate on their responses. This survey was developed by members of the study team and refined through preliminary testing by several other pediatric rheumatologists not affiliated with our study.
Statistical analysis
Survey data were analyzed using chi-square statistics for categorical data. Principal components analysis, a form of factor analysis, was used to identify clusters of related factors to which clinicians attributed similar importance when making decisions about stopping/tapering medications15. To understand whether professional interest in JIA or clinical experience was related to clinicians’ outlook or approach to CID, we tested for differences in responses between those who were and were not affiliated with the JIA Committee and between attending rheumatologists with at least 10 years of post-training experience and all other respondents. To test for evidence of nonresponse bias, we compared the characteristics of survey respondents with the broader CARRA community, the characteristics of respondents who did and did not complete the survey, and the responses of early and late survey respondents who completed the survey16. Early response was defined as completion of the survey before the first reminder was sent 2 weeks after the initial invitation.
Two-sided p values < 0.05 were considered statistically significant. All analyses were conducted using Stata 12.1 (StataCorp).
RESULTS
Among 388 clinicians of CARRA, 132 responded to the survey (34%) and 124 completed it (32%; completion rate: 94%). Of those clinicians who completed the survey, 121 (31% of clinicians in CARRA) reported taking clinical care of children with JIA and were thus eligible to complete the full survey (hereafter called “respondents”). Survey respondents were most commonly attending physicians (87%) and had a pediatric-only practice (87%) with at least 50% clinical professional time (73%) and at least 10 years of post-training clinical experience (49%; Table 1). One-half of respondents were affiliated with the JIA Committee; respondents consisted of 33% of JIA Committee clinician members and 40% of its attending physician members.
Characteristics of survey respondents who reported taking care of children with JIA. Values are n (%).
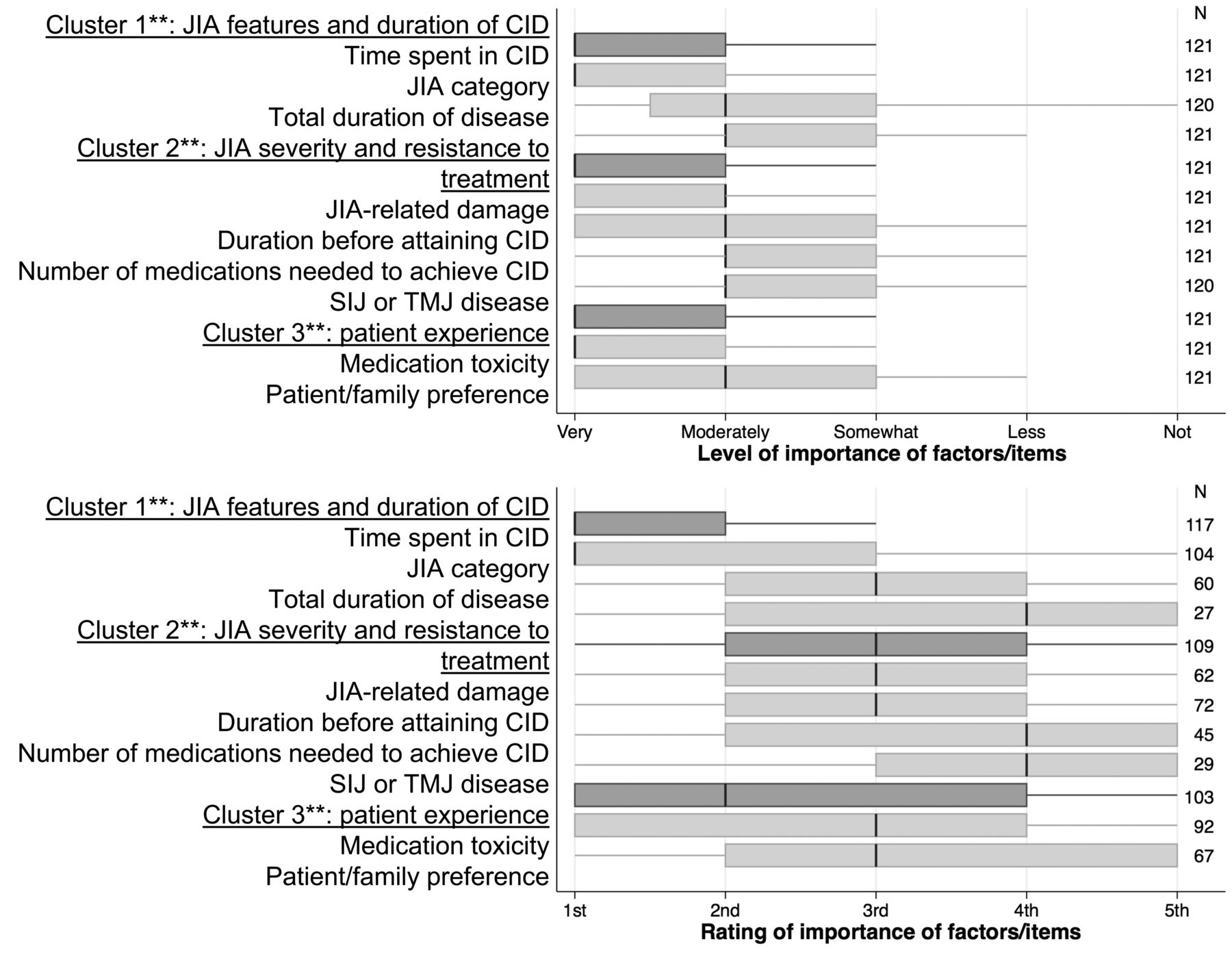
When asked to consider the importance of factors in making decisions about withdrawing JIA medications, respondents generally classified most factors provided to them as moderately or very important (Figure 1). Two factors were classified as very important by over half of respondents: time that a patient spent in CID and a history of drug toxicity. Most participants also ranked these 2 factors most highly and most often among their top 5 factors for decision making. Other commonly ranked factors were JIA duration before attaining CID, patient/family preferences, presence of JIA-related damage, and JIA category. Regarding JIA category, clinicians were least likely to stop medications for children with rheumatoid factor (RF)-positive polyarthritis (85%) and most likely to stop medications for children with persistent oligoarthritis (87%; Figure 2). Three clusters of factors were identified through principal components analysis: (1) JIA features and CID duration: time spent in CID, JIA category, and total disease duration; (2) JIA severity and resistance to treatment: duration of JIA before CID, joint damage, number of drugs needed to achieve CID, and a history of sacroiliac or temporomandibular disease; and (3) patient experience: drug toxicity and patient/family preference. Participants mentioned additional important factors in decision making that were not included in the survey. These factors included history of prior JIA flares or failed attempts to taper (n = 6), which were most strongly correlated with cluster 1, and difficulty in controlling JIA disease (n = 4), which was most strongly correlated with cluster 2. Three respondents also identified life context as important, such as timing vis-à-vis competitive sports events or transition of care.
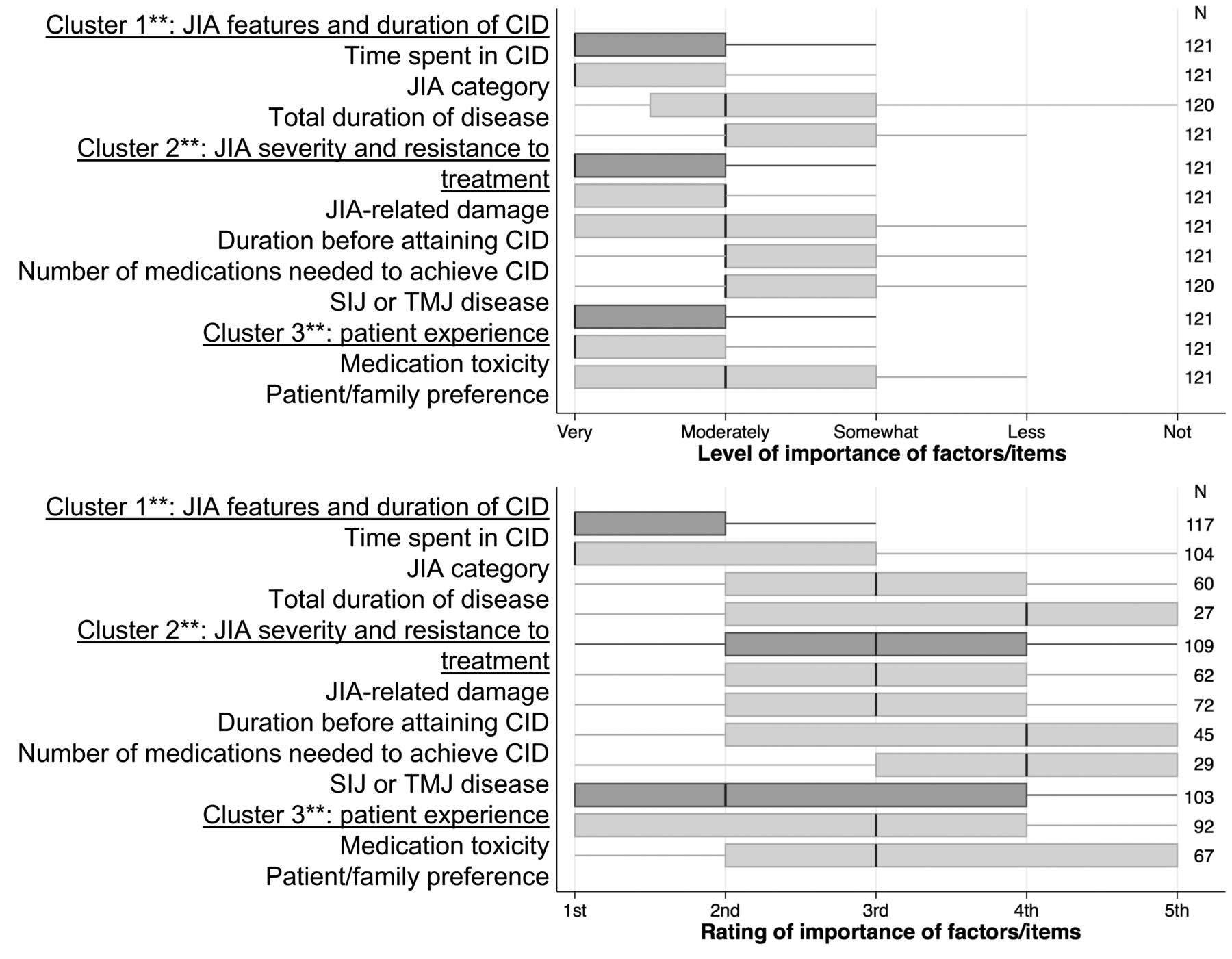
Importance and ratings of survey items for making decisions about withdrawing therapy for children with JIA and CID. Box plots show responses at the median (vertical black line), between the 25th and 75th percentiles (shaded rectangle), and outside the 25th and 75th percentiles (shaded lines), excluding outliers. ** Clusters of survey items (dark gray bars) were derived by principal components analysis; overall importance/rating of the cluster reflects the highest level among items within that cluster (light gray bars). JIA: juvenile idiopathic arthritis; CID: clinical inactive disease; SIJ: sacroiliac joint; TMJ: temporomandibular joint.
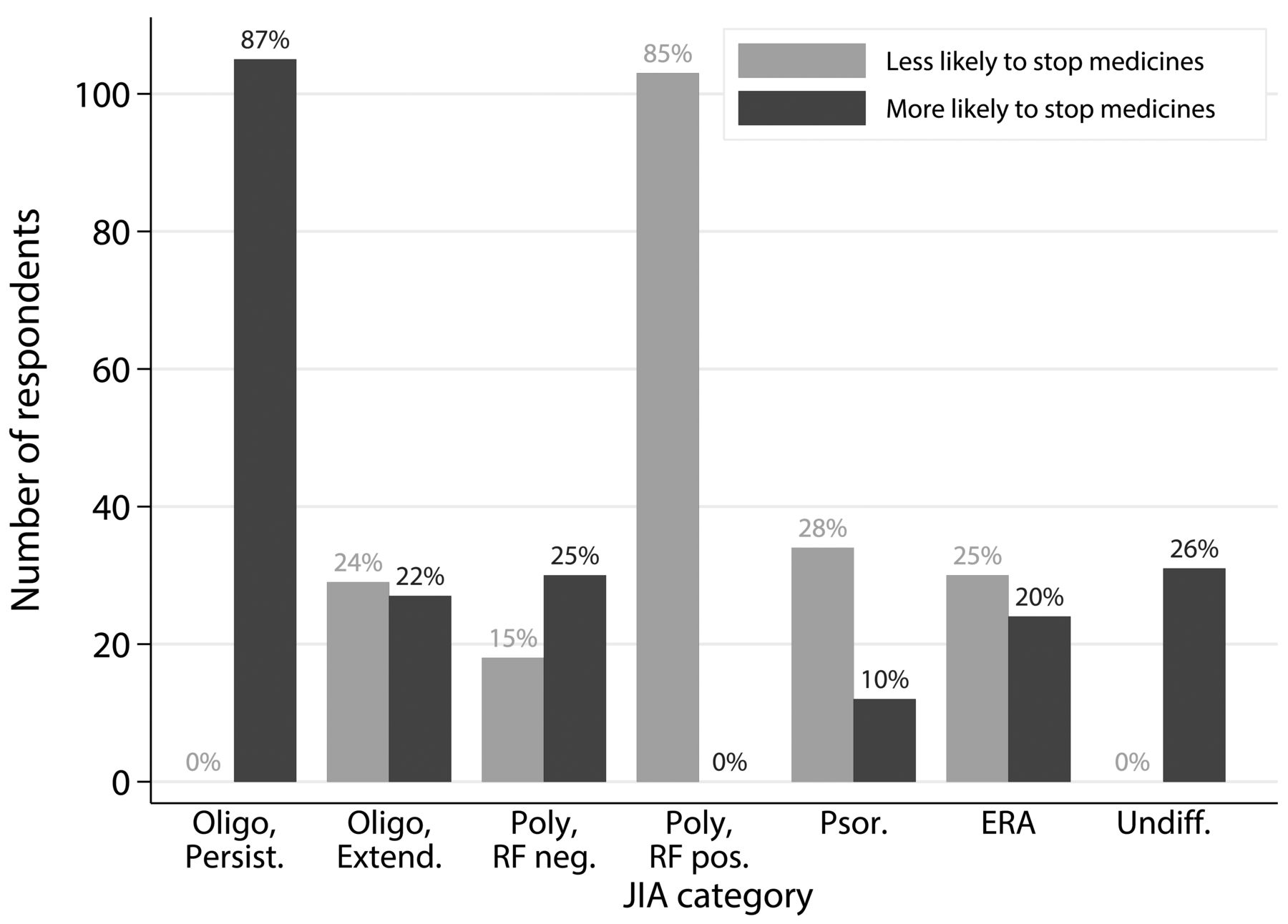
Influence of JIA category on likelihood of stopping medications for patients with CID. JIA: juvenile idiopathic arthritis; CID: clinical inactive disease; Oligo, Persist.: persistent oligoarticular JIA; Oligo, Extend.: extended oligoarticular JIA; RF: rheumatoid factor; Poly, RF neg.: RF-negative polyarticular JIA; Poly, RF pos.: RF-positive polyarticular JIA; Psor.: psoriatic JIA; ERA: enthesitis-related arthritis; Undiff.: undifferentiated JIA.
In addition to prioritizing the factors above, participants were asked to identify clinical features that would make them reluctant to withdraw JIA medicines for children who otherwise met formal criteria for CID for a “sufficient amount of time” and assuming patients/families were interested in stopping medicines. The most commonly cited factors were history of erosions (81%), asymptomatic joint abnormalities on ultrasound (US; e.g., increased Doppler signal) or magnetic resonance imaging (MRI; e.g., edema or enhancement; 72%), and failure of multiple prior DMARD or biologics (64%) to control the JIA (Table 2).
Considerations for withdrawing JIA medications and participants’ estimates of patient outcomes after treatment withdrawal. Values are n (%).
Regarding preferred duration of CID, over half of respondents said that they would wait a minimum of 12 months of CID before starting to withdraw MTX or biologic monotherapy (Figure 3). A sizable minority of participants would wait only 6 months before considering tapering or stopping MTX (31%) or a biologic (23%). Fewer respondents indicated that they would wait 18 months or longer (13% for MTX, 18% for biologics) or suggested that decisions were too individualized to give a single number (3%–5%).
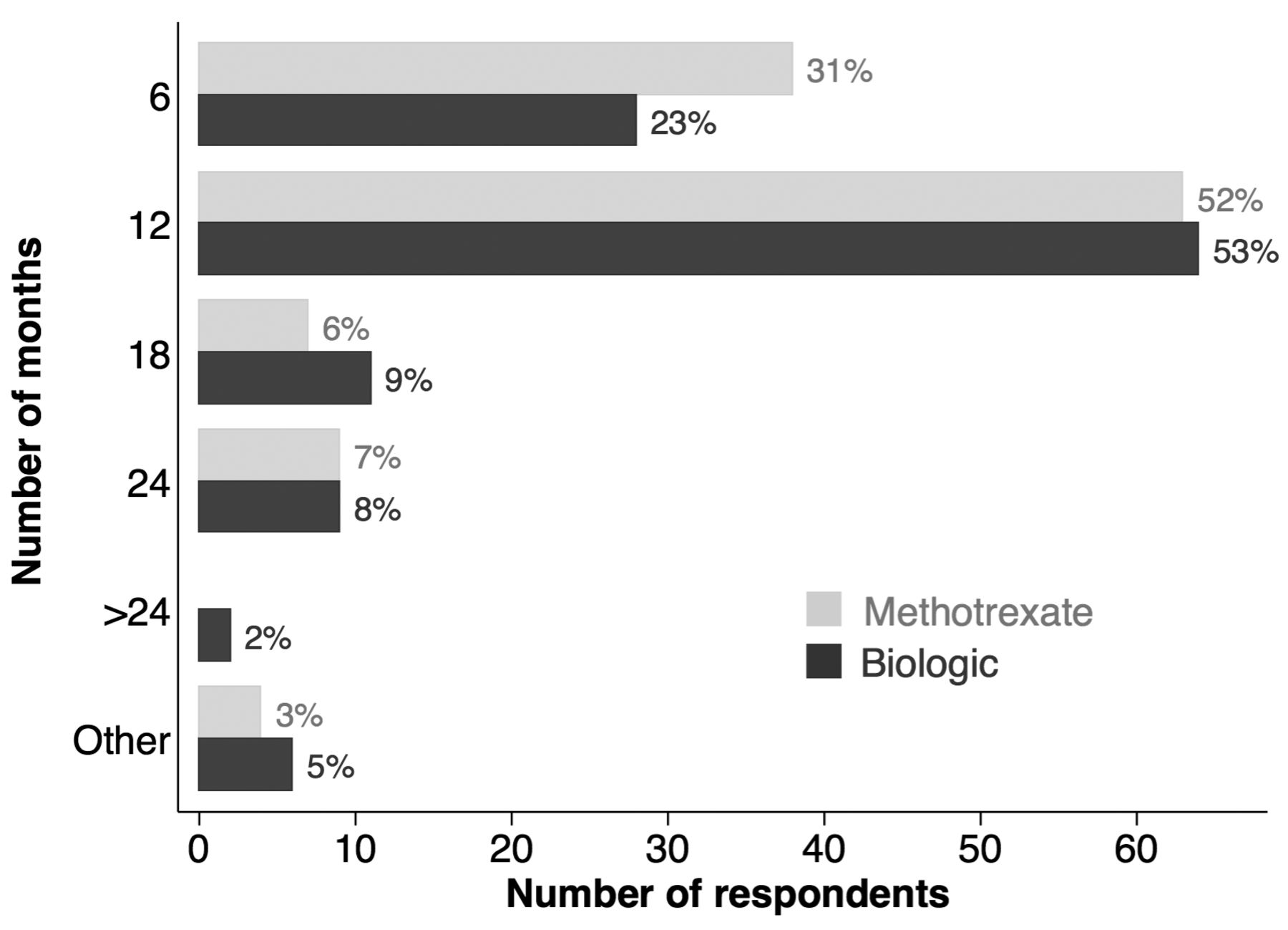
Minimum time that patients with JIA should have CID before withdrawing methotrexate or biologic monotherapy. JIA: juvenile idiopathic arthritis; CID: clinical inactive disease.
There was more heterogeneity among the actual strategies reported for withdrawing these medicines (Figure 4). For children receiving MTX monotherapy, half of respondents reported tapering the drug over 2–6 months. One-third reported tapering MTX more slowly, while about one-fourth performed either rapid tapers (7%) or stopped MTX at once (17%). The responses regarding biologics were even more varied. One-third of respondents would taper biologics over 2–6 months, while about one-fourth favored slower tapers and about one-fourth preferred faster tapers or immediate discontinuation. When respondents wrote in free text how they preferred to taper biologics, 13% indicated spacing out the interval between doses; none reported decreasing drug dose. Compared with MTX, biologics were more commonly maintained indefinitely on fixed longer intervals (21% vs 3%) or fixed lower doses (7% vs 2%). There were no appreciable differences in preferred withdrawal strategies for specific biologic medications; these comparisons were limited by the small numbers of respondents listing preferences for different drugs.

Strategies for withdrawing methotrexate or biologic monotherapy for patients with JIA and CID. Respondents could choose more than 1 strategy. JIA: juvenile idiopathic arthritis; CID: clinical inactive disease.
When asked about children receiving combination MTX/biologic therapy with CID, a majority of clinicians reported tapering or stopping MTX first (63%; Table 2). One-quarter of respondents said that the order of withdrawal was strongly context-dependent; the most commonly cited factor in this decision was a history of drug toxicity or intolerance (10%).
Imaging was not frequently used by most respondents as an ancillary test that influenced decision making to withdraw medicines (Table 2). Fewer than half of respondents reported using imaging often (9%) or sometimes (36%) in decision making. Among imaging modalities, MRI was most commonly chosen as important (72%). While input from patients and family was assumed to be important in decision making, only 25% reported using specific patient-reported outcomes in deciding to withdraw medications (Table 2).
Finally, participants were asked to estimate the outcomes of their patients after stopping DMARD or biologic therapy. A majority of respondents estimated that fewer than half of their patients flared within 1 year of treatment discontinuation. Most clinicians (74%) reported controlling at least half of their patients’ flares with the prior regimen within 3 months of restarting therapy.
We performed several exploratory comparisons of responses between key groups of respondents. When comparing results based on JIA Committee affiliation, there were no significant differences in the importance or ratings of factors, preferred duration of CID, or preferred tapering/stopping strategies (p > 0.05 for all comparisons). When comparing attending physicians with ≥ 10 years of clinical experience with other respondents, experienced physicians were less likely to consider duration of CID (p = 0.02) or patient/family preference (p = 0.01) as important in decision making. There were no other significant differences in the responses between experienced physicians and all others.
In analyzing the possibility of nonresponse bias, attending physicians were more likely to complete the survey (85% of survey completers vs 73% of CARRA clinicians) and fellows were less likely (10% of survey completers vs 22% of CARRA members; overall chi-square p = 0.02). Aside from a trivial difference in the proportion of clinicians with combined pediatric/adult practices, early and late respondents did not significantly differ in demographics, decision making, or management approaches.
DISCUSSION
High-quality evidence is lacking on successful strategies to withdraw medications for patients with well-controlled JIA. In the absence of good evidence or relevant guidelines, as anticipated, we found considerable heterogeneity in the attitudes and approaches of US and Canadian clinicians regarding when and how to withdraw medications for children with CID. Among the many factors considered important in making decisions to withdraw JIA medicines, time spent in CID was most highly ranked by survey respondents, although more experienced physicians tended to value this factor to a lesser degree. Other reported factors that strongly influence decision making include a history of drug toxicity, patient and family preferences, duration of JIA before CID, failure of multiple prior DMARD or biologics, JIA category, a history of joint damage, and the presence of asymptomatic imaging abnormalities suggesting subclinical inflammation. History of prior flare was another important consideration mentioned by numerous respondents. About three-quarters of clinicians would wait for patients to have CID for a minimum of 6–12 months before tapering or stopping medication; about two-thirds of respondents would wait for at least 12 months of CID. Strategies for decreasing or stopping either MTX or biologic therapy varied substantially; a majority of respondents preferred medication tapers lasting over 2 months, while a sizable minority favored maintaining children on biologics given at longer fixed intervals. For children on combination MTX-biologic regimens, most clinicians preferred stopping MTX first.
Some, but not all, of our results corroborate findings of a prior survey of 31 pediatric rheumatologists from the United Kingdom17. Similar to members of CARRA, UK rheumatologists reported duration of remission and presence of problematic drug side effects as important factors in the timing of DMARD withdrawal; JIA category and duration of DMARD therapy were less important. In deciding when to withdraw JIA drugs, UK rheumatologists also considered the timing of major life events, the preferences of patients, and concerns about flare factors echoed by CARRA members. The vast majority of UK rheumatologists surveyed preferred to wait for 1–2 years of disease remission before withdrawing medication. In contrast, a majority of CARRA members now favor withdrawing drugs after 6–12 months of CID. These differences in preferred duration of CID could relate to differences in populations who receive biologics; biologics in the UK are reserved for children with the most severe JIA18, whereas biologic usage is more than twice as common in the United States19. Assuming these treatment differences do not reflect large discrepancies in disease severity between populations, some children with JIA receiving biologics in the United States may have less severe disease and thus a lower risk of bad outcomes if drugs are discontinued sooner. Aside from its larger size and quantitation of influential factors, our survey also identified additional factors that are involved in decision making, including joint damage, imaging findings, and total number of drugs required to achieve CID. We identified 3 main groups of factors important in decision making: (1) JIA features and CID duration, (2) JIA severity and resistance to treatment, and (3) patient experience, including drug toxicity and patient/family preference. Further, our findings are novel in detailing the many ways that clinicians withdraw JIA medications in practice.
Several findings in our study can be compared with the available evidence on drug withdrawal for inactive JIA. CARRA members ranked time spent in CID of greatest importance in deciding when to withdraw JIA medications. However, the main publication supporting this concept is a retrospective study that showed 2 flares among just 12 children who had achieved ≥ 6 months of inactive disease with ETN5. Based on these scant data, the study’s authors advocated waiting for at least 2 years of disease inactivity before withdrawing medications. In contrast, despite the value placed on duration of CID, fewer than 10% of CARRA members reported waiting 2 or more years of CID before withdrawing medications. Of note, several larger studies, including 1 randomized trial, have failed to show that duration of CID is predictive of outcomes after drug discontinuation6,8,11. With regard to imaging, studies have shown that MRI and US can detect subclinical arthritis in children with JIA in clinical remission20,21,22. However, the clinical and prognostic significance of such findings remains unclear23,24. Perhaps this uncertainty helps explain why more than half of respondents seldom or never use imaging to guide decisions on withdrawing therapy. Nonetheless, abnormalities present on imaging, including erosions and evidence of subclinical disease on MRI or US, made most respondents more reluctant to withdraw therapy for children with CID.
RF-positive polyarticular disease was the JIA category that made most respondents less likely to taper or stop JIA medications. This is consistent with prior studies showing that RF-positive polyarthritis is associated with higher rates of flares than other JIA categories8,13. On the other hand, most respondents were more likely to stop medications for those with persistent oligoarticular JIA, even though rates of flares in this category appear similar to other JIA types13. This method may reflect a belief that flares in children with persistent oligoarticular JIA will be less severe and easier to control. Additionally, clinicians may use different approaches when withdrawing MTX versus withdrawing biologics because of underlying differences in the patients themselves; children receiving biologics often have more severe disease. Consistent with this notion, respondents were more likely to taper MTX within 6 months. In contrast, for children receiving biologics, clinicians more frequently lengthened the intervals between doses as a means of reducing dose without fully stopping the drug.
Regarding outcomes after drug withdrawal, most respondents estimated that fewer than half of their patients flare within 1 year of medication withdrawal. These estimates are consistent with studies of children with inactive JIA who predominantly or exclusively received MTX6,13. However, studies of children taking biologics have shown that about two-thirds of patients flare within 1 year of drug withdrawal7,8,11,12. Biologic predictors of flare have been studied, but are not yet validated for routine use in clinical practice6,25. Notably, about three-quarters of respondents estimated that most of their patients’ flares off therapy could be controlled with the prior regimen within 3 months. In contrast, 1 single-center study suggested that disease control, even when successful, often requires longer periods of time11. More research is needed to understand the quality and timing of responses to retreatment across various centers and JIA populations.
Our study had several limitations, including a high rate of nonresponse. Compared with the overall CARRA community, survey respondents were more likely to be attending physicians and less likely fellows. This suggests that our results reflect, to a greater extent, the opinions of more experienced clinicians than a simple random sample of CARRA. Otherwise, there was little evidence that non-response biased our results16. While CARRA membership consists of the vast majority of US and Canadian pediatric rheumatologists, our survey’s findings may not necessarily represent the opinions or practice styles of other clinicians in other parts of the worldwide pediatric rheumatology community. Another limitation in the generalizability of our findings was the exclusion of questions regarding systemic JIA, IBD, PsO, and uveitis from the survey. Such exclusions were intended to simplify responses and encourage participation because in practice, the manifestations and outcomes of these diseases could substantially influence treatment decisions for children with JIA. Other omissions from the survey, such as specific questions about inflammatory markers or patients with prior flares, or more extensive questions about children following combined MTX-biologic regimens, may have left other relevant questions about clinical decision making unanswered. Finally, while the survey was anonymous, it is possible that certain self-reported responses (e.g., regarding preferences of patients and families or patient outcomes) could have been overestimated or subject to recall bias and may not fully reflect respondents’ clinical practices.
To our knowledge, our survey is the first comprehensive evaluation of influential factors and approaches for the clinical management of children with clinically inactive JIA. The attitudes and strategies of US and Canadian pediatric rheumatology clinicians for withdrawing JIA medications are variable. Interestingly, these attitudes and strategies did not appreciably differ between experienced physicians and other respondents. Our survey’s findings will be useful in planning future prospective studies that seek to standardize and optimize treatment withdrawal in JIA and to study the outcomes of drug discontinuation. In addition, these findings from clinicians will be useful to compare with the perspectives of patients and families regarding decisions to withdraw JIA medications.
Acknowledgment
The authors thank Sheffa Ariens for her help in distributing the survey, and the following for their help in testing and refining the survey: Matthew L. Basiaga, MD, MSCE; Alexis Boneparth, MD; AnneMarie Brescia, MD; Kristen N. Hayward, MD, MS; L. Nandini Moorthy, MD, MS; Nanci Rascoff, MD; Susan Shenoi, MD, MS; Lehn Weaver, MD, PhD; and members of the Juvenile Idiopathic Arthritis Protocol Evaluation Subcommittee. Thanks also go to participating members of the Childhood Arthritis and Rheumatology Research Alliance (CARRA). The authors acknowledge CARRA and the ongoing Arthritis Foundation financial support of CARRA.
Footnotes
Funded by Rutgers Biomedical and Health Sciences and the National Institutes of Health/National Institute of Arthritis and Musculoskeletal and Skin Diseases (K23-AR070286).
- Accepted for publication December 8, 2016.








{kind=link}
{kind=link}
{kind=link}
{kind=link}