

Abstract
Systemic lupus erythematosus (SLE) is a prototypical chronic multiorgan autoimmune disorder that can lead to significant burden of disease and loss of life expectancy. The disease burden is the result of a complex interplay between genetic, biologic, socioeconomic, and health system variables affecting the individual. Recent advances in biological understanding of SLE are yet to translate to transformative therapies, and genetic and socioeconomic variables are not readily amenable to intervention. In contrast, healthcare quality, a variable readily amenable to change, has been inadequately addressed in SLE, despite evidence in other chronic diseases that quality of care is strongly associated with patient outcomes. This article will analyze the available literature on the quality of care relevant to SLE, identify knowledge gaps, and suggest ways to address this in future research.
- SYSTEMIC LUPUS ERYTHEMATOSUS
- PHYSICIAN PRACTICE PATTERNS
- PATIENT SATISFACTION
- OUTCOMES
- PRACTICE GUIDELINES
Systemic lupus erythematosus (SLE) is a chronic multisystem autoimmune disease resulting in significant morbidity and loss of life expectancy1. Advances in the understanding of disease pathogenesis have identified new therapeutic targets, but negative randomized controlled studies have stalled translation to clinical use2. Progress has been made in defining treatment goals, which will potentially lead to the implementation of treatment strategies for SLE3. For the present, however, a significant knowledge gap exists regarding the optimization of treatment regimens4, such that evidence-based guidelines for treatment escalation or de-escalation are not in place. While molecular and strategic advances in the treatment of SLE are anticipated, patients continue to experience significant disease burden because of active disease and treatment-related morbidity5. Patient-reported outcome studies have also shown considerable adverse effects of SLE on patients’ perception of health, daily activities, and disability6.
Similar to other chronic diseases, SLE requires frequent interaction with the healthcare system even in asymptomatic patients7. Disease outcomes in SLE, whether considered in terms of mortality, disease activity, end-organ manifestations, or patient-reported measures, are the result of a complex interplay between genetic, biological, socioeconomic, and environmental variables8. In other chronic diseases9,10, research into quality of care has attracted much interest because of the demonstration of a relationship between better quality care and improved patient outcomes. In contrast, the study of healthcare quality has been largely overlooked in SLE, despite it being an area that is potentially highly amenable to intervention (Figure 1). Identifying deficiencies in quality of care can pave the way for strategies, such as the development of evidence-based chronic disease management programs, that can significantly affect patient outcomes even in the absence of new drugs. Our review analyzed the available literature on the quality of care in SLE, identified key knowledge gaps in application of healthcare quality approaches to SLE, and addressed ways to bridge these gaps in future studies.
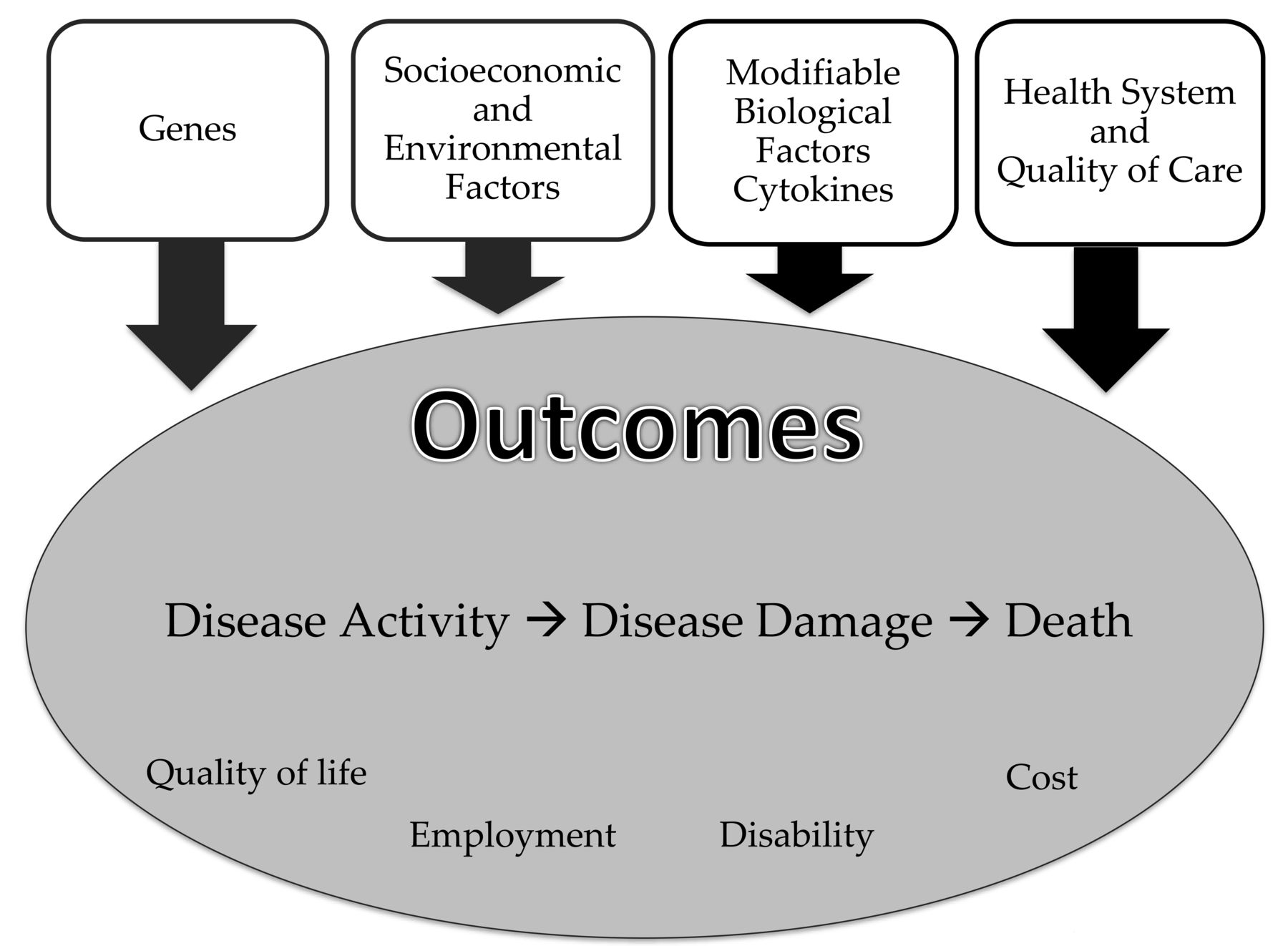
Effect of genetic, socioeconomic, and care-related variables on outcomes in systemic lupus erythematosus (SLE). There are many determinants of outcome in SLE that can be broadly grouped into genetic, biologic, socioeconomic, and health system variables. Genetic variables (e.g., ethnicity or gene polymorphisms) and socioeconomic and environmental variables (e.g., household income and education) are largely irremediable. In contrast, certain biological variables (e.g., cytokines) and healthcare delivery variables can be modified. Some SLE outcomes can be conceptualized as linear, such as disease activity leading to disease damage and consequent mortality. Other outcomes such as changes in quality of life, employment, disability, and cost have a more complex relationship, may not develop sequentially, and can influence each other.
Defining and measuring healthcare quality
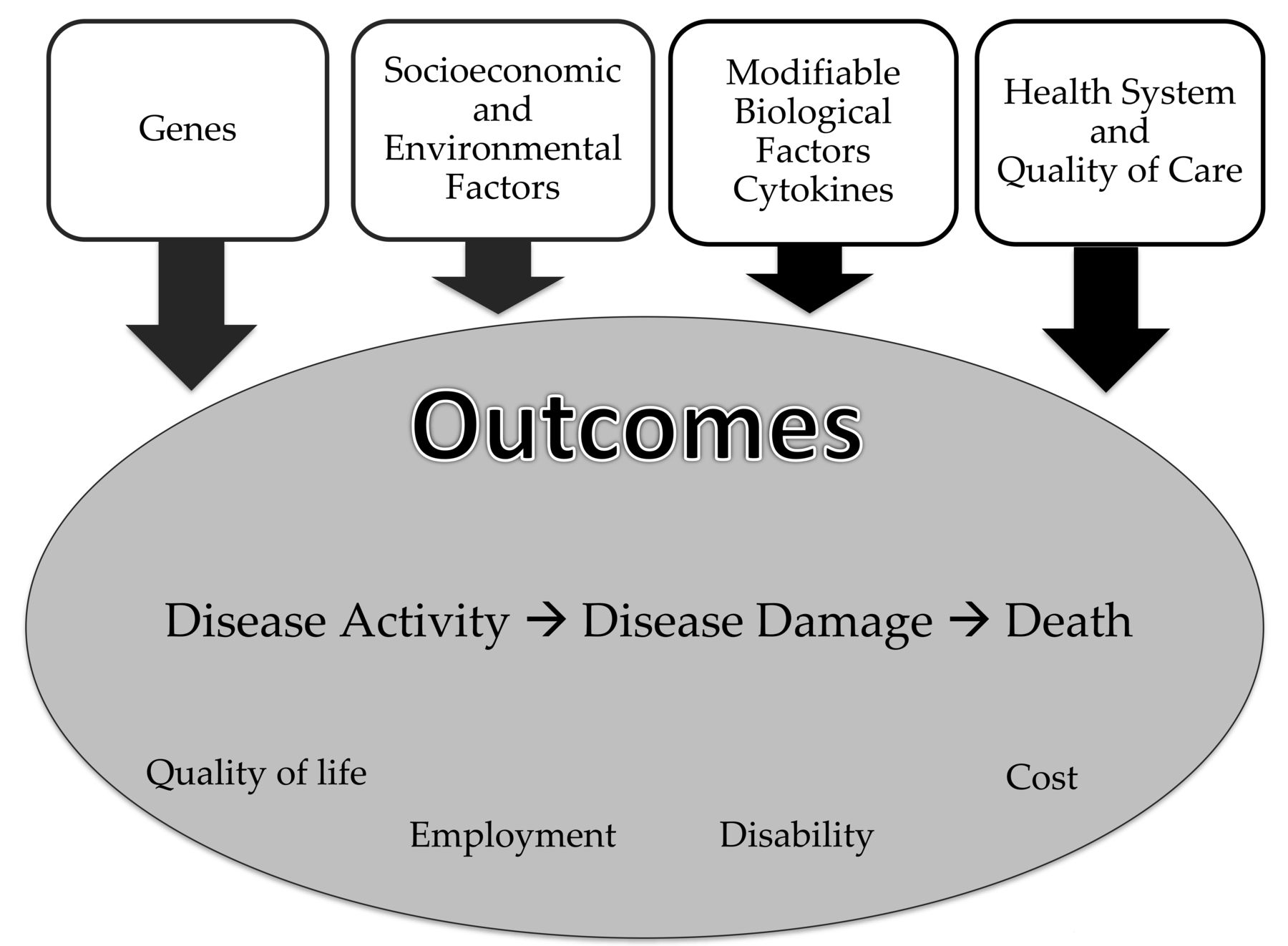
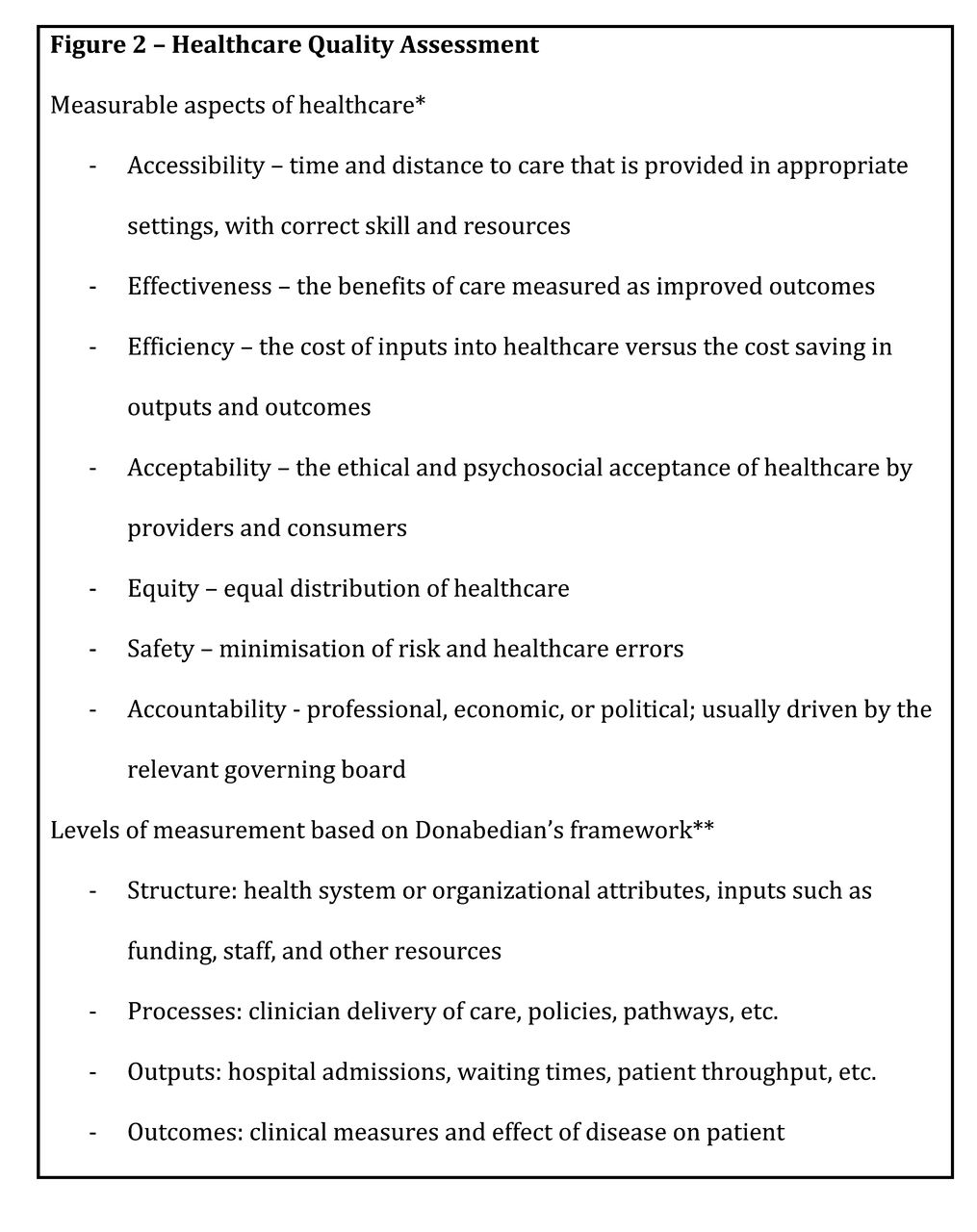
Healthcare quality can be defined as a measure of practice patterns that may affect health outcomes. It takes into consideration the characteristics of the physicians and other healthcare providers, hospital and other healthcare settings, as well as the interactions between healthcare providers and patients in different stages of a patient’s journey. Given its multifaceted design, different frameworks have been used to understand the broad dimensions that healthcare quality covers. The Donabedian framework, for example, is most commonly used, and describes a linear relationship between healthcare structures, processes of care, and health-related outcomes (Figure 2 and Table 1)7,11–20,21–30,31,32,33,34,35,36.

Healthcare quality assessment. * Areas or dimensions of healthcare performance that can be quantitatively assessed and improved36. ** Levels of healthcare measurement based on Donabedian’s framework, which describes a linear relationship between healthcare structure, processes, outputs, and outcomes35.
Summary of selected studies assessing quality of care in SLE. Table demonstrates the range of healthcare quality topics studied and how they link to different aspects and levels of quality measurement described in Figure 2.
Improvement in quality of care in chronic diseases can be conceptualized according to areas such as access, efficiency, effectiveness, appropriateness, acceptability, and safety (Figure 2 and Table 1)36. The McColl Institute Chronic Care Model (CCM), a multidirectional framework of quality of care, has been applied to several chronic diseases in primary care with resultant improvements in preventive care and reduction in hospitalizations10. Models of care for the prevention and management of disability have resulted in improved patient outcomes in several musculoskeletal conditions, such as osteoarthritis (OA), rheumatoid arthritis (RA), chronic back pain, and osteoporosis37. SLE has a lower prevalence than other musculoskeletal conditions, but is more complex, and its management within the healthcare system is complicated and costly. Therefore, it seems likely that improvements in healthcare quality in SLE have the potential to improve patient outcomes and potentially reduce cost.
Research on healthcare quality has lagged other areas of research. Qualitative health quality research, such as gathering information about the healthcare system from focus groups, can often shed light on factors that are worthy of pursuit38. Interview- or observation-based methods can examine the priorities of patients and caregivers, and identify potential obstacles to improvement.
Quantitative health quality research can complement qualitative research. The development of quality indicators, sometimes referred to as performance indicators, allows the assessment of practice variation based on evidence-based practice and expert opinion. Disease-specific quality indicators are available in a few rheumatological conditions such as RA39, OA40, and systemic sclerosis41. Successful use of quality indicator performance data allows identification of gaps between guidelines and actual practice. It highlights areas where there may be variability between different healthcare settings, and the results may lead to a reassessment of the effectiveness of interventions as laid out in published guidelines42.
Healthcare quality needs to be distinguished from quality of life. Patients with SLE report reduced health-related quality of life compared with the general population, with measures similar to those of patients with coronary artery disease, endstage airways disease, human immunodeficiency virus, and RA6,43. As a group, these diseases have been recognized as among the leading causes of the global disability burden from chronic disease44. While they are distinct concepts, improved healthcare quality can improve quality of life.
Quality of care in SLE — the worldwide experience
Healthcare structure
The literature on the effect of healthcare structure in SLE, summarized in Table 1, is dominated by studies in the United States that largely report issues related to access to care. Vast disparities in access are described45, heavily skewed by patients’ medical insurance status, which plays a crucial role in access to and therefore receipt of appropriate care11. Patients lacking insurance have infrequent specialist care12, travel farther to see a specialist, and are more likely to attend the emergency department for care of their SLE13. Insurance status has been shown to have a significant effect on delivery of preventive care17, hospital admission30,31, morbidity22,27,28,46, and mortality32,33.
The effect of insurance status on the quality of care in SLE suggests that this is not only a significant factor in outcomes, but a major research confounder. In contrast to the literature on the effect of health insurance on quality of care in the United States, there are very few data on other structural aspects of the healthcare system, such as issues relating to access to specialists from countries with universal healthcare. In a Canadian cross-sectional questionnaire of patients with SLE and physicians, barriers to healthcare were identified by both, particularly access to medications, which are not universally covered in Canada14. Interestingly, patients identified more barriers than did physicians. Studies from Germany and Russia have shown that patients with SLE wait long periods to receive specialist care47 and continue to accrue significant damage48.
Processes of care
Processes of care, as described by the Donabedian framework, include all the interactions between healthcare professionals and patients. Processes of care are thought to be more sensitive to change than structural components in healthcare quality research, and variation in practice has been shown in different disease models to lead to differences in outcomes49.
Quality indicators in SLE management have mostly been focused on processes of care. There are at least 2 sets of SLE quality indicators that have been developed based on rigorous methodology established by Mosca, et al50 and Yazdany, et al51. Evidence-based quality indicators were used to assess performance in categories such as immunization and sun avoidance, osteoporosis and drug monitoring, renal and cardiovascular (CV) disease prevention, and pregnancy care by reporting the proportion of eligible patients receiving the care advocated by each quality measure51. In some areas such as counseling for sun avoidance and vitamin D supplementation, performance was high (83%–90%), whereas management of hypertension in patients with lupus nephritis (LN) and assessment of traditional CV risk factors was received by only 54% and 29% of patients, respectively18. This large variation in the delivery of evidence-based care highlights an urgent need to revise healthcare processes to improve implementation of care.
Other studies in SLE have also shown poor performance on osteoporosis and CV disease care19,20, as well as reproductive health measures such as counseling about teratogenic medications21,52. Likewise, recommended primary care preventive services such as immunizations and cancer screening were received by less than a third of patients with SLE in the southeastern United States53. In these studies, predictors of poor performance on quality indicators were younger age, non-white ethnicity, and fewer physician visits; the results suggest a lack of adequate health insurance was again a major driver of these discrepancies18,21,30,53. A further US study of quality indicator performance in LN found that among patients without insurance, only a third had received any immunosuppression by 12 months post-diagnosis, and 13% relied on the emergency department for routine care of their SLE22. Risk factors for suboptimal care of LN included endstage renal disease54, non-white ethnicity, and a lack of insurance29.
Appropriate medication use can also be measured by relevant quality indicators, with cost-effectiveness studies of immunosuppressive treatment showing vast potential savings to health systems and patients24,25. Even the use of antimalarial medication, known to have a protective effect on survival55, is still suboptimal in some studies, with reported use ranging from 57%–73%23,56. Routine measurement of hydroxychloroquine and other immunosuppressive treatment drug levels has been suggested as a method to improve adherence4, but to be effective this must coincide with improved physician-patient communication57, something that can potentially be achieved through improved models of care for SLE.
Other quality indicators may also be developed based on our understanding of SLE as a chronic disease. Using the CCM framework, quality indicators in relation to clinical information systems, decision support, self-management support, and community linkages can also be studied and validated. To date, there has been no study to examine the application of CCM framework in SLE and its relationship with disease or patient outcomes, but it has been suggested in a review to be highly applicable to SLE58.
Healthcare outputs and outcomes
There have been few quality-of-care studies examining healthcare outputs and outcomes in SLE. Avoidable hospitalizations for conditions such as pneumonia, congestive cardiac failure, and cellulitis occur in 12.7% of patients with SLE in 1 study31, and readmission rates within 30 days can be as high as 16.5%30. In-hospital mortality has been examined in relation to physician or hospital experience, that is, the collective experience of the treating physician or hospital in dealing with patients with complicated SLE. Patients who present themselves to highly experienced hospitals are less likely to die32,33. In the Lupus Outcomes study, better performance on quality indicators was associated with improved longterm outcomes such as damage accrual, confirming the validity of using performance on quality indicators to improve patient outcomes26.
The patient perspective
Healthcare system performance, including structure, process, and outcomes, can also be measured through indices of patient experience, providing an assessment that is complementary to measures obtained from clinical record reviews. Certain components of the patient experience can be quantitatively measured, for example, waiting time, doctor communication, and availability of patient information59. Patients with SLE are able to identify their perceived unmet needs for care15,60, and inadequate education, lack of support at the time of diagnosis, emotional and physical barriers to care, and difficulty navigating the health system have been documented among these needs61. Evidence suggests that patients with SLE feel misunderstood by their families, the community, and even the specialists treating them62, with the result that patients feel that their quality of life needs are not met by treating teams63.
While some variables can be measured directly, patient experience is inherently multifaceted, influenced by disease severity, previous care experience, and inherent patient values. One US study showed that satisfaction with SLE care was higher among patients at tertiary centers compared with regional centers, despite care being provided by the same physicians16. There is a strong association between patient interaction with providers and the health system and performance on technical quality of care, although further study is required to clarify cause and effect in this relationship64. Nevertheless, satisfied patients have been shown to be more treatment-adherent and allegiant to healthcare providers, 2 factors associated with better clinical outcomes and quality of life65.
Are we doing enough to measure and improve healthcare quality in SLE?
Measuring performance on quality indicators in SLE could lead to the identification of addressable deficiencies in healthcare, and in turn to redesigning the current model of care. Little is known regarding whether interventions that improve performance on quality indicators will translate into an improvement in outcomes, but the positive relationship between higher quality of care and lower damage accrual in the Lupus Outcome Study is encouraging26. In addition, there are limited data on the relationship between healthcare quality and health economic burden in SLE. Interventions to improve healthcare quality do not necessarily mean additional cost. Savings can be made if improvement in healthcare quality results in a substantial improvement in productivity, quality of life, or survival. Much remains to be done.
Unlike diseases such as RA, few evidence-based models of care exist for SLE, despite a burden of pain, functional limitation, and reduced health status equivalent to that of patients with RA66. A treat-to-target approach has been proposed to improve outcomes in SLE, and achievement of such a target was recently reported to be associated with improved SLE outcomes67. While many large observational cohorts of patients with SLE monitor clinical and biological variables, very little is known about healthcare quality in these cohorts, despite performance on quality indicators being potentially just as important for disease outcomes26.
The first step in improving healthcare quality in SLE must therefore be developing systems that routinely measure quality of care, and correlate these against important patient outcomes (Figure 3). A variety of data sources are available including direct reporting by patients, medical record reviews, or administrative data. Performance on quality indicators can then be used to determine whether improvement can be made at the structural or process level. For example, in Australia, specialist care for SLE is provided by rheumatologists, nephrologists, and immunologists in any combination of solo private practice, public hospital general clinics, or specialized SLE clinics68, each of which has been established without data on the benefits or otherwise of that particular structure. Clinicians should take a leadership role in gathering data that will provide the backbone of better clinical governance and healthcare quality research.

Conceptual quality assessment and improvement strategy using processes of care. Aspects of healthcare quality can be measured and changed at multiple levels. The most commonly measured aspect of quality is the process of care, documenting the actual care the patient receives. Quality indicators are disease-specific measures of processes of care, designed as a benchmark for the minimally acceptable standard of care based on evidence. Using these to assess the process of care allows for the identification of deficiencies, and therefore of targets for improvement. Addressing these deficiencies is done through process redesign, ensuring that the desired care needs are met. Improvements in care quality in turn have the potential to translate to better patient outcomes. Top row is adapted from Donabedian’s framework35.
Conclusions and recommendations for future research
Much of the current research on SLE outcomes focuses on the effect of biological determinants, even though many of these are not modifiable with current treatments (Figure 1). In contrast, health system variables such as quality of care are highly amenable to change, but have been comparatively neglected in SLE. Policy change and the implementation of new programs are challenging, but experience in other chronic diseases suggests that significant benefits may result if healthcare quality can be improved. Assessment of quality of care in SLE should no longer be ignored. Using conceptual models of chronic disease management as a roadmap, current practice can be reconfigured to an evidence-based approach that meets the needs of individual patients with SLE. The first step, analyzing deficiencies in quality of care, can happen in any SLE clinic today; we advocate that it should.
- Accepted for publication November 9, 2016.








{kind=link}
{kind=link}
{kind=link}