

Abstract
Objective. To characterize the practicing rheumatologist workforce, the Canadian Rheumatology Association (CRA) launched the Stand Up and Be Counted workforce survey in 2015.
Methods. The survey was distributed electronically to 695 individuals, of whom 519 were expected to be practicing rheumatologists. Demographic and practice information were elicited. We estimated the number of full-time equivalent rheumatologists per 75,000 population from the median proportion of time devoted to clinical practice multiplied by provincial rheumatologist numbers from the Canadian Medical Association.
Results. The response rate was 68% (355/519) of expected practicing rheumatologists (304 were in adult practice, and 51 pediatric). The median age was 50 years, and one-third planned to retire within the next 5–10 years. The majority (81%) were university-affiliated. Rheumatologists spent a median of 70% of their time in clinical practice, holding 6 half-day clinics weekly, with 10 new consultations and 45 followups seen per week. Work characteristics varied by type of rheumatologist (adult or pediatric) and by practice setting (community- or university-based). We estimated between 0 and 0.8 full-time rheumatologists per 75,000 population in each province. This represents a deficit of 1 to 77 full-time rheumatologists per province/territory to meet the CRA recommendation of 1 rheumatologist per 75,000 population, depending on the province/territory.
Conclusion. Our results highlight a current shortage of rheumatologists in Canada that may worsen in the next 10 years because one-third of the workforce plans to retire. Efforts to encourage trainees to enter rheumatology and strategies to support retention are critical to address the shortage.
There is concern in Canada1,2 and other countries3,4,5 that the number of rheumatologists may be insufficient to meet population needs and that there may be regional disparities6, with clustering around larger urban centers leading to greater challenges in access to specialty care in rural/remote areas.
“Rheumatologists per capita” is a performance measure in Canada7. Additionally, if available, it is recommended to identify the number of clinical full-time equivalents (FTE) per population to reflect the percentage of working time allocated to direct patient care. Currently, we do not have estimates outside academic institutions for the number of clinical FTE rheumatologists8,9,10.
A national workforce survey of Canadian rheumatologists was conducted in collaboration with the Canadian Rheumatology Association (CRA) with the primary objective of estimating the number of adult and pediatric clinical FTE rheumatologists. Secondary objectives were to describe (1) the demographics of the current rheumatologist workforce including retirement projections, (2) the uptake of electronic medical record (EMR) use, (3) rheumatologists’ participation in traveling clinics, telehealth, and e-consultation, (4) collaboration with allied health professionals (AHP), and (5) how care was delivered to Canadian indigenous populations.
MATERIALS AND METHODS
Survey development
A literature review was conducted8 to determine whether other sources for rheumatologist workforce information were available and if there were gaps in knowledge about these estimates and workforce characteristics. A set of draft questions was then developed and circulated to 20 people including adult, pediatric, community- and university-based rheumatologists, researchers, AHP, and CRA staff for input on question scope and wording. The survey consisted of a total of 63 questions and was pilot-tested in French and English.
Identification of survey participants
A practicing rheumatologist was defined as either a physician with rheumatology and/or internal medicine or pediatric certification with at least 1 clinic weekly devoted to rheumatology. CRA staff identified practicing rheumatologists from the following sources: CRA membership list (this includes some retired members, trainees, and scientist members who were not practicing); the Royal College of Physicians and Surgeons (RCPSC); the provincial colleges; as well as snowball sampling, whereby rheumatologists in leadership positions recruited rheumatologists in their provinces/communities who may not have been readily identified by other sources.
Survey dissemination
The survey was sent out by the CRA electronically on March 9, 2015, and closed August 23, 2015. The following strategies were used to maximize participation rates: periodic reminders were circulated to nonresponders by e-mail, fax, and office phone calls; the survey was advertised on the CRA Website and in membership communications; and during the spring, an identified “provincial champion” for the project presented information about the survey at regional rheumatology meetings.
Analysis
To maintain the privacy of individuals, because only a small number of internists reported practicing as rheumatologists, these groups were combined. Also, cell sizes n < 6 are not displayed and/or data from regions are aggregated. Medians and interquartile ranges (IQR) are reported for continuous variables because the distribution of the data was not normal. Percentages are reported for categorical data. Where data are incomplete, the denominator is displayed (n). SPSS version 22 (IBM) was used for all analyses.
The national clinical FTE was estimated based on the survey question asking respondents to report the percentage of time allocated to clinics. Because the survey did not have a complete response rate, we applied this percentage to the number of rheumatologists practicing in each province according to the data from the Canadian Medical Association (CMA) from 2015 (n = 398)11. We mapped the number of FTE rheumatologists in each province using ArcGIS version 10.2.2 (ESRI Inc.). We then determined the number of FTE rheumatologists (adult and pediatric considered together) required in each province to meet a threshold of 1:75,000, a threshold recommended by the CRA Human Resources (HR) committee (oral communication with the committee chair as described by Kur and Koehler2).
Ethics
Ethics approval was provided by the University of Calgary (REB14-2135). The CRA HR committee approved the manuscript.
RESULTS
Response rates
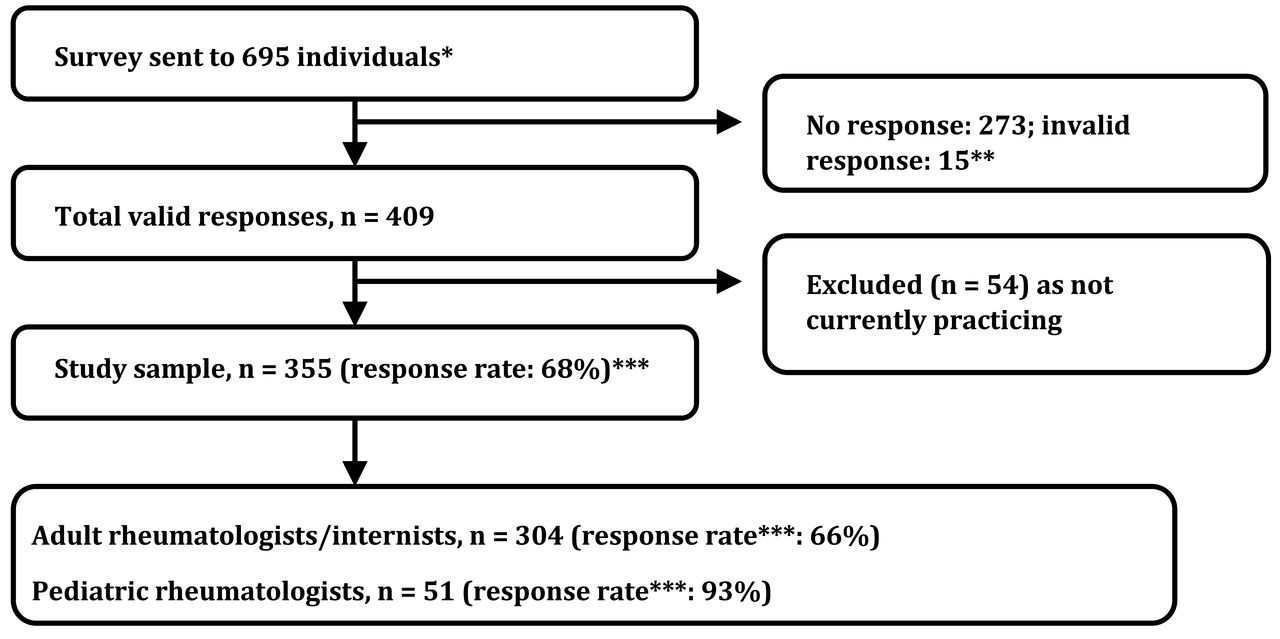
Figure 1 depicts survey response rates. The CRA sent the survey to 695 individuals (including retired members, trainees, and scientists). According to CRA data, this included an estimated 519 practicing rheumatologists (464 adult rheumatologists/internists and 55 pediatric rheumatologists). There were 409 total valid responses in which eligibility for the study could be determined and of these, 54 did not meet inclusion criteria, yielding a sample of 355 rheumatologists and a response rate of 68% based on a denominator of 519 practicing rheumatologists (66% for adult and 93% for pediatric rheumatologists).

Response rate to Stand Up and Be Counted rheumatologist workforce survey. * Includes ineligible individuals who are CRA members (retired, not in clinical practice, trainees). ** Responses were deemed invalid if an individual consented to the survey but did not answer a single question, or did not confirm that they were a rheumatologist. *** Response rate 355/519 = 68%, based on the Canadian Rheumatology Association (CRA) estimated number of practicing rheumatologists (464 adult rheumatologists/internists, 55 pediatric rheumatologists).
Respondent characteristics
Table 1 depicts the respondents’ characteristics. Although there were respondents from all Canadian provinces, because of small cell sizes to respect confidentiality, responses in some provinces were grouped by regions. Most respondents had certification in rheumatology from the RCPSC and/or the Collège des Médecins du Québec (CMQ; n = 299, 84%). Eighteen respondents (5%) had certification from outside Canada (and no Canadian certification) or had entered practice before the institution of rheumatology examinations at the RCPSC in 1972. Thirty-four (10%) had pediatric or internal medicine certification from the RCPSC and/or CMQ with no additional rheumatology certification.
Characteristics of respondents to the Stand Up and Be Counted survey1. Values are n (%) unless otherwise specified.
The distribution of respondents by year of practice is shown in Table 1. The median age of respondents was 50 years and 47% were men. Overall, one-third (32%) plan to retire within the next 5–10 years.
Practice characteristics
Although 81% of rheumatologists were affiliated with an academic center, only 40% of adult rheumatologists and 80% of pediatric rheumatologists had university-based practices (Table 2). Seventy percent of rheumatologists used an EMR in their practice with provincial numbers varying from 50% in Quebec to 83% in Alberta, and the majority were office-based platforms (52%).
Practice characteristics of respondent rheumatologists. Values are n (%) unless otherwise specified.
Almost all respondents (96%) held general rheumatology clinics (either adult or pediatric). However, 63 rheumatologists (19%) reported participation in subspecialty clinics (Table 2). Although pediatric rheumatologists only consisted of 15% of rheumatologists in Canada, an additional 150 adult rheumatologists (50% of 300 respondents) reported seeing patients < 18 years old. Seventy-five adult rheumatologists also reported providing care to pediatric patients in transition clinics (25% of 300 respondents) and the minimum patient age reported for these clinics was 17 years (IQR 16–17).
Respondents reported that 70% of their practices consisted of patients with inflammatory arthritis (IQR 50–80) and 50% were patients with comorbidities (IQR 30–60). English was the most frequent language of communication with patients (92%), followed by French (27%), and 9% of rheumatologists reported communication with patients in 1 or more of 12 other languages.
Remuneration
Sixty-one percent of rheumatologists billed as fee for service (FFS); however, this proportion varied by province (Table 2) and was higher for adult than pediatric rheumatologists (69% vs 16%) because 84% of pediatric rheumatologists were paid through an alternate funding or blended funding arrangements. The remainder of rheumatologists were paid for their services using some form of alternate funding. Nationally, 78% of rheumatologists billed as a “rheumatologist,” although this also varied by province, with some provinces having a higher proportion of rheumatologists billing as other specialist types, most commonly as a “general internist” (Table 2). Among pediatric rheumatologists, 6% billed as a pediatrician and an additional 4% billed as both a pediatrician and a rheumatologist.
Work characteristics
Work characteristics varied by type of rheumatologist (adult or pediatric) and by practice setting (community- or university-based).
For all adult rheumatologists, the median time allocated to clinical practice was 75% (IQR 60%–90%). The median number of half-day clinics was 7 (IQR 4–8). The median number of new patients seen per week was 12 (IQR 8–20) and the median number of followups was 50 (IQR 30–70). Community-based adult rheumatologists held a median of 8 half-day clinics per week (IQR 6–9), the median number of new patients per week was 16 (IQR 10–24), and the median number of followups was 55 (IQR 40–75). University-based adult rheumatologists held a median of 4 half-day clinics per week (IQR 3–6) with a median of 8 new patients seen per week (IQR 4–12) and 36 in followup (IQR 25–55).
For all pediatric rheumatologists, median time allocated to clinical practice was 60% (IQR 46%–70%). The median number of half-day clinics was 3 (IQR 2–4). The median number of new patients seen per week was 4 (IQR 2–5) and the median number of followups was 15 (IQR 8–20).
Both adult and pediatric rheumatologists estimated spending a median of 2 half-days per week devoted to clinical paperwork. For both groups, the median number of weeks worked per year was 46, and the median hours worked per week was 50. Most rheumatologists (91%) reported that they were still accepting new patients in their practices.
Sixty-three percent of rheumatologists participated in a rheumatology call roster, and the median number of days per year on-call for adult rheumatologists was 53 and for pediatric rheumatologists was 90; however, this number varied substantially by province (Table 3). In addition, 5% of adult and 10% of pediatric rheumatologists participated in internal medicine and pediatric call schedules exclusively. Nine percent of rheumatologists reported that participating in an internal medicine or pediatric call schedule was mandatory, with < 1% reporting that they subcontracted this work to a locum.
Work characteristics. Values are median (interquartile range) unless otherwise specified.
Rheumatologists per capita
The national estimate of the percent of time allocated to clinical work from the workforce survey was used to adjust 2015 data on rheumatologist numbers per province from the CMA11 to estimate the number of clinical FTE rheumatologists (adult and pediatric considered together) per 75,000 population (Figure 2). None of the Canadian provinces met the threshold of rheumatologists 1:75,000 when FTE was considered. The deficit of full-time clinical rheumatologists required to meet the threshold in each province varied between 1 and 77, with a total deficit of 203 (Figure 2). However, it should be noted that the CMA has published a lower estimate of rheumatologists11 than the CRA estimated for our denominator (398 vs 519). Our estimated denominator was not used in mapping because we did not have a complete response rate and therefore could not confirm that all 519 were indeed rheumatologists. However, using 519 as the total number of Canadian rheumatologists and applying the adjustment based on the national clinical FTE still revealed a deficit of 117 rheumatologists nationwide.

Map of Canada depicting the number of FTE-practicing rheumatologists per 75,000 population (see legend colors) and the number of FTE rheumatologists required to meet the target of 1:75,000 benchmark (superimposed provincial count). FTE were estimated based on the national median reported time allocated to clinics from all respondents of the 2015 Stand Up and Be Counted survey and used to adjust the 2015 Canadian Medical Association numbers of rheumatologists in each province. FTE: full-time equivalent; YU: Yukon; NT: Northwest Territories; NU: Nunavut; BC: British Columbia; AB: Alberta; SK: Saskatchewan; MB: Manitoba; ON: Ontario; QC: Quebec; NL: Newfoundland and Labrador; PE: Prince Edward Island; NB: New Brunswick; NS: Nova Scotia.
Provision of care to rural and remote communities
Participants estimated that 20% of the patients in their practice travel > 2 h to receive care (IQR 5–30). This estimate was higher in university-based practices compared with community-based (20% vs 15%) and in pediatric rheumatology practices compared with adult (25% vs 15%).
Sixteen percent (54/341 respondents) reported participating in traveling clinics, including 11 pediatric (23%) and 43 adult rheumatologists (15%). The median number of new and followup patients seen per year through traveling clinics was 48 (IQR 24–102) and 120 (IQR 63–289), respectively. Fourteen percent (48/339) reported participating in telehealth or e-consultation services, including 35 adult rheumatologists (12%) and 13 pediatric rheumatologists (27%). The median number of new patients seen per year through telehealth or e-consultation was 12 (IQR 4–36) and the median number of followups per year was 24 (IQR 5.5–60).
Provision of rheumatology care to patients with indigenous identity
Rheumatologists were asked to estimate the percentage of their practice who were patients of indigenous identity and to describe how and where they provided care for this population. Seventy-three percent of rheumatologists reported providing rheumatology care for patients with an indigenous identity and estimated that this population represented 5% of their primary rheumatology practice (IQR 2%–5%), 15% of patients seen in their traveling clinics (IQR 5%–50%), and 2% of patients seen by telehealth or e-consultation (IQR 2%–35%; respondent denominators shown in Table 2).
Rheumatologists seeing patients with indigenous identity were remunerated for their work usually through FFS (73%, 247 respondents). When traveling to rural/remote communities, a variety of funding sources for travel/accommodations were reported, including provincial governments, provincial arthritis agencies, regional health authorities, and local hospitals. Rheumatologists also reported paying for travel/accommodations themselves.
Collaboration with AHP
Almost half (47%) of rheumatologists reported working with AHP in their rheumatology clinic. The proportion of rheumatologists who did traveling clinics, e-consultation, or telehealth with AHP was 9/54. Working with AHP was more commonly reported among pediatric rheumatologists (85% compared with 40% of adult rheumatologists). The most common reported type of professional working with a rheumatologist in clinic was a registered nurse (n = 114 respondents), followed by a physiotherapist (n = 45 respondents), occupational therapist (n = 30 respondents), and an Advanced Clinician Practitioner in Arthritis Care Extended Role Practitioner (ACPAC ERP; a special designation in Canada for AHP with advanced training in arthritis diagnosis and management12, n = 28 respondents). Fifty-two rheumatologists had access to a social worker, 12 to a dietitian, and 29 to a pharmacist.
The most common tasks in a rheumatology clinic for nurses were in-clinic patient education, assisting with rheumatology clinic, and providing teaching and/or administration of intramuscular or subcutaneous medications. Physiotherapists assisted by seeing patients in clinic, providing in-clinic education, and/or class-based patient education.
Seventy-nine percent of rheumatologists reported a need to increase the numbers of AHP working in their rheumatology clinics; however, most respondents identified barriers to this occurring, including funding (n = 123/125, 98%), office space (56%), finding AHP with appropriate training (50%), recruiting and retaining staff (28%), and concerns about practice scope (18%). Very few rheumatologists were concerned that AHP detracted from physician billings (6%). Other concerns included hospital politics, lack of administrator/funder understanding of the value of AHP to patients, administrators preventing AHP from working within their full scope, and difficulties with unions/funders restricting AHP work schedules (e.g., more dedicated time allotted to inpatient and/or urgent care settings than to ambulatory rheumatology clinics).
DISCUSSION
To our knowledge, ours is the first national rheumatology workforce survey in Canada. It provides valuable information about the workforce for use in planning, recruitment, and development of enhanced models of care. The survey highlights that the rheumatologist workforce in Canada is aging and up to one-third plan to retire in the next 5–10 years. Further, the current number of rheumatologists in all provinces and territories is inadequate to meet population needs, with a deficit of up to 203 rheumatologists. The CRA HR committee has estimated that the number of rheumatologists needed is about 1:75,000 population2. While this threshold is not scientifically derived, it is a reasonable estimate and is in alignment with other workforce targets reported in the United States and in the United Kingdom13,14,15. There is no single accepted threshold for rheumatologists per capita in Western countries, with a recent review finding up to a 5-fold difference in workforce requirements16. Our work provides a basis for geographic information systems-based studies to more accurately ascertain a supply-demand ratio for the Canadian population.
There are about 34 rheumatology residency positions8 across Canada each year, although this varies yearly and some positions may be designated for out-of-country trainees who may leave after graduation. It is therefore unlikely, based on current and future demand, even with maximum enrolment, that sufficient numbers of rheumatologists will be practicing to meet current population demands in all centers. This problem may even be more marked in pediatric rheumatology where there are only 3 Canadian training centers.
The survey also provided insights about practice characteristics of rheumatologists in different settings (community- vs university-based) and in adult and pediatric practices. Clinical practices of adult and pediatric rheumatologists differed, with pediatric rheumatologists doing more calls and seeing fewer patients in the clinic setting — this could be due to factors such as having a largely academic practice with a smaller proportion of FTE (60% vs 75%) for clinical care. Indeed, clinical volumes are lower in university-based compared with community-based practices. Additional differences, which contribute to pediatric clinical volumes, include the need to spend more time with children and their families and increased focus on developmental, psychosocial, and family issues. Across Canada, there are many adult rheumatologists seeing patients < 18 years of age, which may reflect access issues to pediatric rheumatology in some centers and regions. Encouragingly, many adult rheumatologists were participating in transition clinics for pediatric rheumatology patients.
Given the vast geography of Canada, it is not surprising that rheumatologists estimate that 20% of patients travel > 2 h for rheumatology care. Conversely, a small number reported participating in traveling clinics and using tools such as telehealth and e-consultation for patients in rural and remote regions. It is unclear whether the current patterns of care delivery in these regions are meeting patient needs. Further work needs to be done to better determine access to care, especially in indigenous communities, given the higher prevalence of rheumatic conditions in this population17 and a more severe phenotype of disease18.
While this was a rheumatologist survey, we recognize that rheumatology care benefits from interprofessional teams. Indeed, almost half of respondents reported working with AHP and a majority identified a desire to increase AHP numbers in their practice, with finances being the main barrier identified. While AHP scope of practice was briefly analyzed, this area warrants further study, especially considering the new Canadian ACPAC program certification19,20. It is unclear whether ACPAC ERP and other AHP are working to their full scope across Canada. There are benefits to shared models of arthritis care including ACPAC ERP as well as increasing access to arthritis care21,22 and patient satisfaction23. It is also unclear which other specialists in Canada may be managing patients with various rheumatic conditions; this, too, warrants further analysis and consideration in future studies of the rheumatology workforce.
Several limitations to our work are recognized. First, it is possible that some rheumatologists were not identified and consequently were not invited to participate in the survey. There is no single comprehensive list of rheumatologists in Canada; however, a list based on multiple sources was generated, but it is possible that this was incomplete. Accordingly, it was challenging to estimate the denominator for our response rate calculation. Further, although response rates were moderate for our survey (overall 59% and 68% of practicing rheumatologists), they were still substantially higher than the last American College of Rheumatology (ACR) workforce survey in the United States in 2005–2006, where the return rate was 37%3. Response rates were higher for pediatric rheumatologists, likely because it is a small and largely academic community that collaborates frequently on national projects, facilitating communication about the survey. Additionally, pediatric rheumatologists have conducted workforce surveys every 2–3 years8 and therefore were potentially more attuned to responding. It is also possible there was some systematic bias in response rates, with lower-than-anticipated numbers of respondents in some provinces (e.g., Quebec and Newfoundland) and it is also likely that university-based rheumatologists are overrepresented in respondents.
Finally, an important limitation of our study is that we do not have a proven benchmark in Canada for the number of rheumatologists required per capita that is based upon population estimates of rheumatic disease prevalence and healthcare use. Instead, we used an accepted CRA benchmark of 1:75,000, but note that Dejaco, et al16 have recently shown that there is a great heterogeneity in methods used regarding rheumatology workforce planning in Western countries.
While we were unable to provide an estimate of the number of rheumatologists in each province because of incomplete response rates, we did obtain an estimate of the median clinical FTE for rheumatologists and applied it to the CMA’s provincial rheumatologist numbers11, but were unable to provide further within-province regional distributions. It should also be noted that the CMA’s estimate of the number of rheumatologists was lower than our denominator estimate, likely because we included internists who were practicing as rheumatologists. Our projected workforce shortage also needs to be further evaluated using modeling to better account for changes in supply and demand over time, which is beyond the scope of our present work.
Our projection of a current and future deficit of rheumatologists and a maldistribution of rheumatologists is not a problem unique to Canada3,4,24, although some countries, including the United Kingdom5, have reported improvements in the rheumatologist workforce supply over the last 10 years. The ACR recently launched a workforce study and the results are available25, although studies based on the ACR membership database4 and Medicare physician claims data26 suggest ongoing rheumatologist supply issues in many regions.
Our workforce study highlights a need for further investigation of workforce supply compared to population needs in Canada. Based on our data and estimates, it is likely many regions currently have an insufficient number of rheumatologists, and given retirement projections and an aging population, this will likely be exacerbated over the next 5–10 years. This is an issue shared with many other countries, including the United States3. Finally, our study highlights the current distribution of Canadian rheumatologists, and may allow future vision for training and retention of rheumatologists and AHP and dispersion of practices for optimum patient care.
Acknowledgment
The authors acknowledge the Canadian Rheumatology Association Human Resource committee members for supporting this work and providing input and provincial champions: Dr. Trudy Taylor, Dr. Patrick Liang, and Dr. Aurore Fifi-Mah for reviewing a French translation of the survey. We also thank Dr. Ronald Laxer for reviewing a version of the manuscript.
Footnotes
Funding provided by the Arthur J.E. Child Chair Rheumatology Outcomes Research. In-kind support for administration of the survey and promotion of the project was provided by the Canadian Rheumatology Association (CRA). Dr. Marshall is a Canada Research Chair in Health Services and Systems Research and the Arthur J.E. Child Chair Rheumatology Outcomes Research. L. Jewett was paid through the Arthur J.E. Child Chair in Rheumatology for her work on this project. Dr. Lacaille holds the Mary Pack Chair in Rheumatology research from The Arthritis Society of Canada and the University of British Columbia. Dr. Cividino is the current chair of the CRA Human Resources committee. Dr. Baillie was the president of the CRA at the time this study was completed.
- Accepted for publication October 26, 2016.








{kind=link}
{kind=link}