

Abstract
Objective. Beyond the exacerbation of pain in describing a flare in osteoarthritis (OA), patients and health professionals add other elements that deserve to be fully elucidated, such as effusion, swelling, and mobility limitation. To define and conceptualize the construct flare in OA, the objective was to identify the key variables, or symptoms, that worsen, and to clarify how these variables are described in the literature by patients and clinicians.
Methods. A systematic review of the literature was conducted in Medline and PsychINFO. In brief, the search terms used were “osteoarthritis,” “knee,” “hip,” and “flare.” Specific characteristics of included studies were identified, including the type of study design, type of flare assessed, how the flare developed, and what definition of flare was used, including whether the definition was based on qualitative or quantitative analysis.
Results. Pain was the major factor in the definition of flare within these studies. Four components of flare were identified: pain, other factors, composite criteria, and global assessment. While the majority of studies reported flare as an increase in pain using standardized outcome measures, only 1 study reported the antecedents and consequences of a pain flare using qualitative methods.
Conclusion. The use of flare as an outcome or inclusion criterion in rheumatology trials is a common occurrence; however, this review highlights the wide variation in the definitions of OA flare currently in use and the emphasis on the measurement of pain. This variation in definition does not allow for direct comparison between trials and limits interpretation of evidence.
To develop an evidence-based tool to measure “flare” in osteoarthritis (FLARE-OA), an Outcome Measures in Rheumatology (OMERACT) Working Group has been established and has held virtual Special Interest Group sessions. This is the first report from this group and we aim to use this information to develop interviews with those involved and the implementation of Delphi questionnaires.
With the development of clinical trials targeting hip and knee OA and short- and longterm treatment of symptoms, there is a need for a tool to identify the occurrence of flare in lower limb OA. Such treatments are currently under development, including slow acting or disease-modifying drugs, and will likely bring important changes in patient management. The development of a FLARE-OA tool is essential to identify the occurrence of flare. Indeed, 2 treatments may provide similar improvements over the longterm, but 1 may prevent more flare than the other in between the 2 assessments, therefore improving the patient’s quality of life.
A definition of the construct of flare for OA is needed. The term flare is used in most Westernized countries, including in French (poussée) and in English. Flares tend to be episodic, with a duration ranging from minutes to hours to days. The characteristic feature is that it requires a change in treatment or behavior. Beyond the exacerbation of pain, however, patients and health professionals add other elements that deserve to be fully elucidated, such as effusion, swelling, and mobility limitation.
Although frequently used in general and in patient descriptions, the term flare has not been largely used in the scientific OA literature. Some authors combine several criteria to define or rule out a flare, for example, sudden aggravation of knee pain causing nocturnal awakenings with clinical evidence of knee effusion1. A diagnosis score has been developed for knee OA flare based on a combination of morning stiffness, pain causing nocturnal awakenings, knee effusion, limping, joint swelling, and increased warmth over the knee2. This first interesting attempt, however, did not integrate the patient’s perspective.
Many clinical trials in OA have used a flare design in which the flare is provoked by the temporary interruption of regular medication, resulting in patients with active and painful disease at baseline. Most clinical trials in OA use outcomes centered on exacerbation of pain and consequences regarding discomfort, activity limitation, and less frequently, participation restriction, as outlined in the International Classification of Functioning, Disability and Health framework3. Investigation of the definition of flare used would help document practices, and later serve to develop the FLARE-OA tool.
A definition of flare in rheumatoid arthritis (RA) has been developed by an OMERACT Working Group as “any worsening of disease activity that would, if persistent, in most cases lead to initiation of change of therapy; and a flare represents a cluster of symptoms of sufficient duration and intensity to require initiation, change or increase in therapy”4. The signs and symptoms in RA are different in many aspects, but there may be some similarities that could inform the definition in OA. To define and conceptualize the construct “flare” in OA, our aim was to identify the key variables or symptoms that worsen, and to clarify how these variables are described in the literature by both patients and clinicians.
This is, to our knowledge, the first attempt to examine the variation in definition of OA flare used in research studies and clinical trials. Comparison of outcomes is made difficult by this variability in definition. Our aim was to use the results of this review, in conjunction with patient involvement, to guide the development of a tool to measure flare in OA.
MATERIALS AND METHODS
A systematic review of the literature, following PRISMA guidelines (prisma-statement.org/documents/PRISMA%202009%20checklist.pdf), was conducted in Medline and PsychINFO during March 2017, without restriction on language or date of publication. A review protocol for our study has not been presented. Publications up until March 4, 2017, were eligible for inclusions. In brief, the search terms were “osteoarthritis,” “knee,” “hip,” and “flare,” with the full search shown in Table 1.
Search terms for Medline and no. results found.
Studies were included in which participants had confirmed OA and if a specific definition of OA flare was reported, either in qualitative or quantitative methods. Screening of records was undertaken by 3 authors (MM, LD, FG) reviewing titles, abstracts, and full-text articles where necessary. Articles were then double-extracted independently by 2 authors (LD, MC). Consensus on final inclusion of articles was assessed, with a third reviewer (FG) available to resolve outstanding disagreements. Assessment of risk of bias within articles was not addressed because the definition of OA flare used within the study was the outcome of interest.
Specific characteristics of included studies were identified, including type of study design; type of flare such as flare as part of the study design, flare as an inclusion criterion, or flare as an outcome; how the flare developed; and the definition of flare used (based on qualitative or quantitative analysis).
Extracted data from each article allowed the description of the characteristics of the definition of the term flare in OA. Because our analysis was a review of published literature, ethics approval was not required, in accordance with the policy of the relevant institutions in France and Australia.
RESULTS
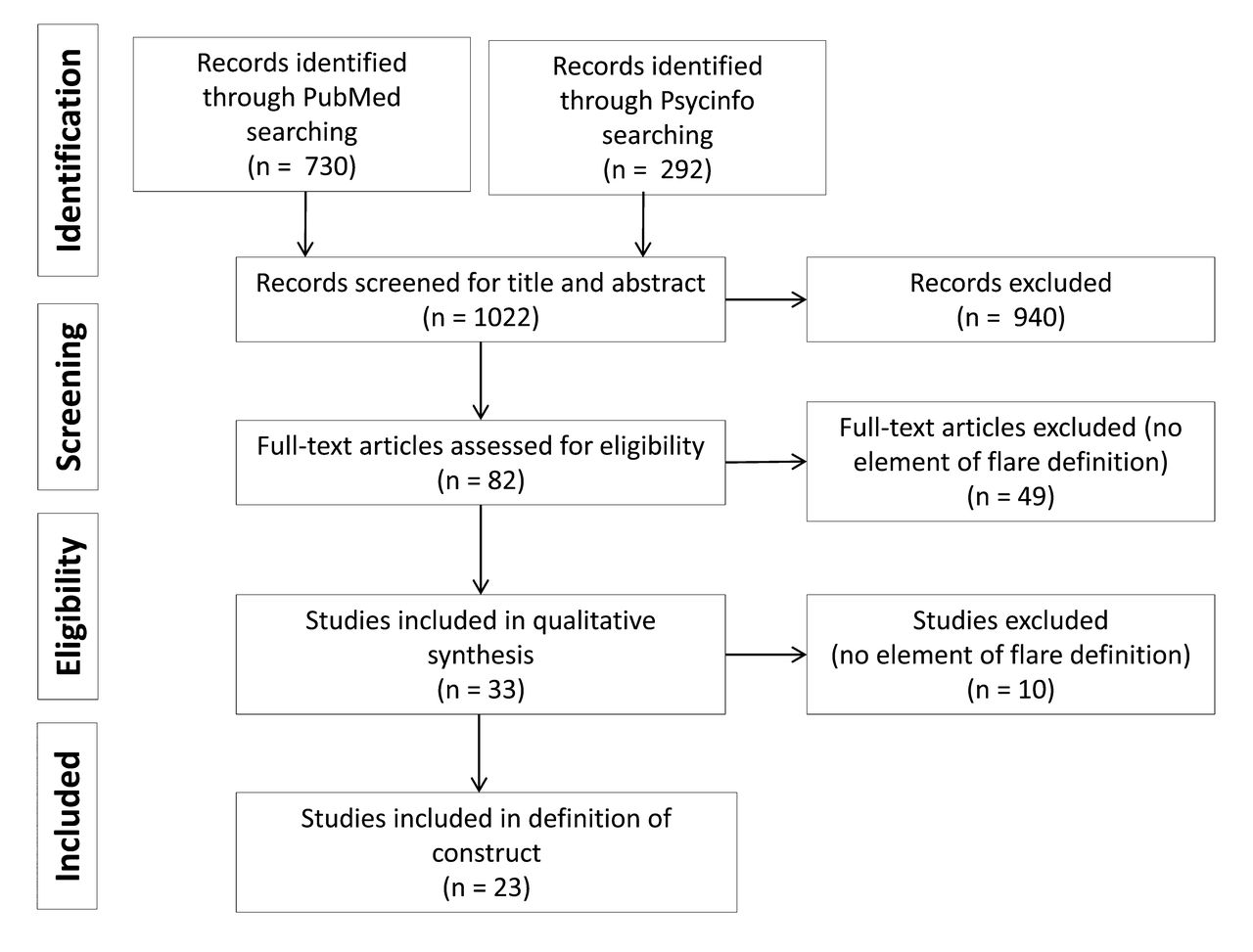
Results of the search are outlined in the study flowchart (Figure 1). Of the 1022 publications identified, 33 were included in the final review process.
Results of literature search.
Consensus discussions resulted in 23 articles considered for final inclusion. Initially, concordance was 79% good agreement, 15% intermediate, and 6% mismatched for study inclusion and definition used. Following discussion and involvement of the third reviewer, consensus was reached regarding definition of flare in included studies. Of the included studies, 15 were clinical trials including a metaanalysis; 3 were the development and validation of a diagnostic tool; and 5 were prognostic studies including a literature review. Twelve studies were of flare design, 2 were of flare inclusion, and 8 of flare outcome. One study included both a flare inclusion and outcome (Table 2)2,5–14,15–22,24,25,26,27.
Studies included in the analysis by type of study.
While the majority reported flare as an increase in pain on Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), visual analog scale (VAS), or global assessment, only 1 study reported the antecedents and consequences of pain flare, using qualitative methods, including the timing of the increase in pain, such as whether it was sudden or of short duration5 (Table 2).
From the assessment of these publications, 4 components of the definition of flare have been identified:
Flare as a concept of pain (pain criteria): 19 items included at least 1 assessment of pain. Eleven reported increasing pain, 9 the need for minimal pain on VAS, and 3 increasing of pain on movement. Other items analyzed in qualitative analysis included timing, awakening at night, sudden increase in pain, increased pain on weight bearing, sharpness, intense pain, and short duration.
Flare as factors other than pain (other factors): 2 articles described joint effusion or swelling and 1 mentioned warmth. Other items analyzed the concept of prolonged morning stiffness, sensitivity/tenderness, limp, and resorting to medication.
Flare as composite factors (composite criteria): 10 articles described a change in the WOMAC score, others spoke of worsening disease status and deteriorating functional status. Qualitative analysis in 1 article investigated antecedents, such as increased activity or sitting for long periods and consequences of actions, such as using additional pain medication or resting until pain decreases.
Flare as a global evaluation (global assessment): 7 articles described a worsening of the overall assessment of the patient and 4 a worsening on the physician’s global assessment.
DISCUSSION
The use of flare as an outcome or inclusion criterion in rheumatology trials is common; however, our review highlights the wide variation in definition of OA flare currently in use and the emphasis on the measurement of pain. This variation does not allow for direct comparison between trials and limits interpretation of evidence. Having a standardized methodology for the assessment of flare would facilitate comparison, underpinning the need for development of a new tool for this purpose.
To date, there is no universally accepted, validated method for defining a flare in OA. The prior literature in this context has largely defined a flare using unidimensional constructs such as pain. While this might be an important component of flare, the specific characteristics of flare need to be devolved, both from the perspective of consumers and healthcare professionals. Much of the extant literature relies on 1 group and has not been developed in a systematic or methodologically sophisticated manner. Moreover, the concept of flare is likely to be more complex than a single unidimensional feature such as pain. The majority of studies found in our review used existing standardized measures to identify flare. While these cover aspects other than pain, such as WOMAC function or global assessment, the emphasis on pain remains with many using only the WOMAC Pain scale, varying also between the use of VAS or Likert scales and whether only baseline or change scores are assessed. In addition, describing flare in terms of effusion and warmth may be problematic because these factors may have limited reproducibility.
The OMERACT process highlights the importance of obtaining the patient’s perspective in the development of outcome measures and clinical practice28. What constitutes a flare to health professionals may not be the same to patients. While pain is the most commonly reported feature of flare, other aspects may be important to patients, such as fatigue or activity restriction, and these factors are not currently included in definitions of OA flare. In addition, duration of the flare may vary from patient to patient. Some studies of flare include patients with pain symptoms lasting longer than 8 h9 or for the previous 72 h5. Measuring only pain as specified by the study design may miss these important aspects, so the inclusion of patients’ definitions of flare may offer a broader picture of its effect.
An OMERACT group has undertaken a similar project in defining flare in RA to develop an evidence-based, consensus-driven standard definition that incorporates the patient’s perspective4, and a similar methodology has been used in France by the Strategy of Treatment in Patients with Rheumatoid Arthritis group for flare in RA29. The involvement of patients in the process of developing a standard definition of RA flare includes constitutional, physical, functional, psychological, and time-oriented elements.
The recent focus on chronic care programs and self-management strategies for OA heightens the need for a patient-reported outcome measure of OA flare. There is a need for an instrument that identifies comprehensive aspects of flare in OA that does not only summarize exacerbation of pain, but also encompasses other functional aspects described by patients. The ultimate aim of the FLARE-OA group is to develop a tool for the use in clinical trials and observational studies to identify the occurrence of flare in hip and knee OA.
- Accepted for publication May 12, 2017.








{kind=link}