

Abstract
Objective. To evaluate the initial serological responses to pneumococcal vaccination with the 13-valent protein-conjugated pneumococcal vaccine (PCV13) followed by the 23-valent polysaccharide pneumococcal vaccine (PPV23) among patients with rheumatoid arthritis (RA) treated with biological disease-modifying antirheumatic drugs (bDMARD) according to dosing and intervals between immunizations.
Methods. Investigator-initiated clinical trial. Patients with RA receiving bDMARD were randomized (1:1:1) to immunization with single dose PCV13 followed by PPV23 after 16 or 24 weeks, or double dose PCV13 followed by PPV23 after 16 weeks. A comparison group of patients with RA treated with conventional synthetic (cs)DMARD received single dose PCV13 followed by PPV23 16 weeks later. Pneumococcal antibodies were collected before and 4 weeks after each vaccination. The primary endpoint was the proportion of participants responding to ≥ 6/12 pneumococcal serotypes 4 weeks after both vaccinations.
Results. Sixty-five participants receiving bDMARD and 35 participants receiving csDMARD were included. After PPV23 vaccination, 87% (95% CI 0.76–0.94) and 94% (95% CI 0.77–0.99), respectively, of participants treated with bDMARD and csDMARD had reached the primary endpoint. There was no significant difference in primary endpoint between the 3 randomization arms. The response for rituximab-treated participants was 25% compared to ≥ 89% in participants treated with bDMARD with other mode of action.
Conclusion. The early serological response to prime-boost vaccination with PCV13 followed by PPV23 was very similar among participants receiving bDMARD and csDMARD. However, notable differences in response were observed according to individual bDMARD. It is important to consider the RA treatment when planning pneumococcal vaccination in patients with RA.
- RHEUMATOID ARTHRITIS
- VACCINATION
- IMMUNOSUPPRESSION
- CLINICAL TRIALS
- DISEASE-MODIFYING ANTIRHEUMATIC DRUGS
Patients with rheumatoid arthritis (RA) are at greater risk of pneumococcal disease because of the autoimmune disease itself and the use of immunosuppressive therapies1,2,3,4. Routine pneumococcal vaccination should be considered to reduce morbidity and mortality in patients with RA receiving immunosuppressive treatment, such as conventional synthetic (csDMARD) or biological disease-modifying antirheumatic drugs (bDMARD)5,6. Both Danish national and international guidelines recommend prime-boost vaccination with the 13-valent protein-conjugated pneumococcal vaccine (PCV13) followed by the 23-valent polysaccharide pneumococcal vaccine (PPV23) at least 8 weeks later7,8,9,10.
The PCV13 induces a T cell–dependent immune response and memory T and B cells11. This phenomenon is called priming and it is hypothesized that it enhances a secondary antibody response after contact with the pathogen or revaccination and prolongs the period of protection among the vaccine recipients.
Previous studies investigating the safety and immunogenicity of pneumococcal vaccination in patients with RA have either assessed the earlier 7-valent conjugated pneumococcal vaccine, PCV7, or PPV23, but the currently recommended prime-boost combination of the vaccines has not yet been examined in this population. Further, the optimal vaccine dose and interval between prime and boost vaccination has not been examined.
While it is well recognized that treatment with anti-CD20 monoclonal antibody rituximab (RTX) severely impairs serological responses to immunizations12,13,14, studies of treatment with anti-tumor necrosis factor-α (anti-TNF-α), interleukin 6 inhibitors (anti-IL-6), or T cell lymphocyte costimulation inhibitors (CTLA-4) have shown less severe effect on vaccine responses13,15–24,25. Combination treatment of bDMARD and methotrexate (MTX) has often been associated with decreased seroresponses compared with MTX monotherapy17,18,19,22,24,25.
To date, no studies have investigated the serological response after vaccination with PCV13 followed by PPV23 among immunosuppressed patients with RA. For this reason, our primary objective was to evaluate the serological responses to prime-boost pneumococcal vaccination with PCV13 followed by PPV23 among patients with RA treated with bDMARD according to dosing and intervals between immunizations, according to individual biological drug groups, and compared to responses in patients with RA treated with csDMARD.
MATERIALS AND METHODS
This 3-arm, randomized, parallel-group, open-label, phase III trial in patients with active RA receiving bDMARD treatment was investigator-initiated and conducted at 2 rheumatology outpatient clinics in the Region of Southern Denmark from 2014–2017.
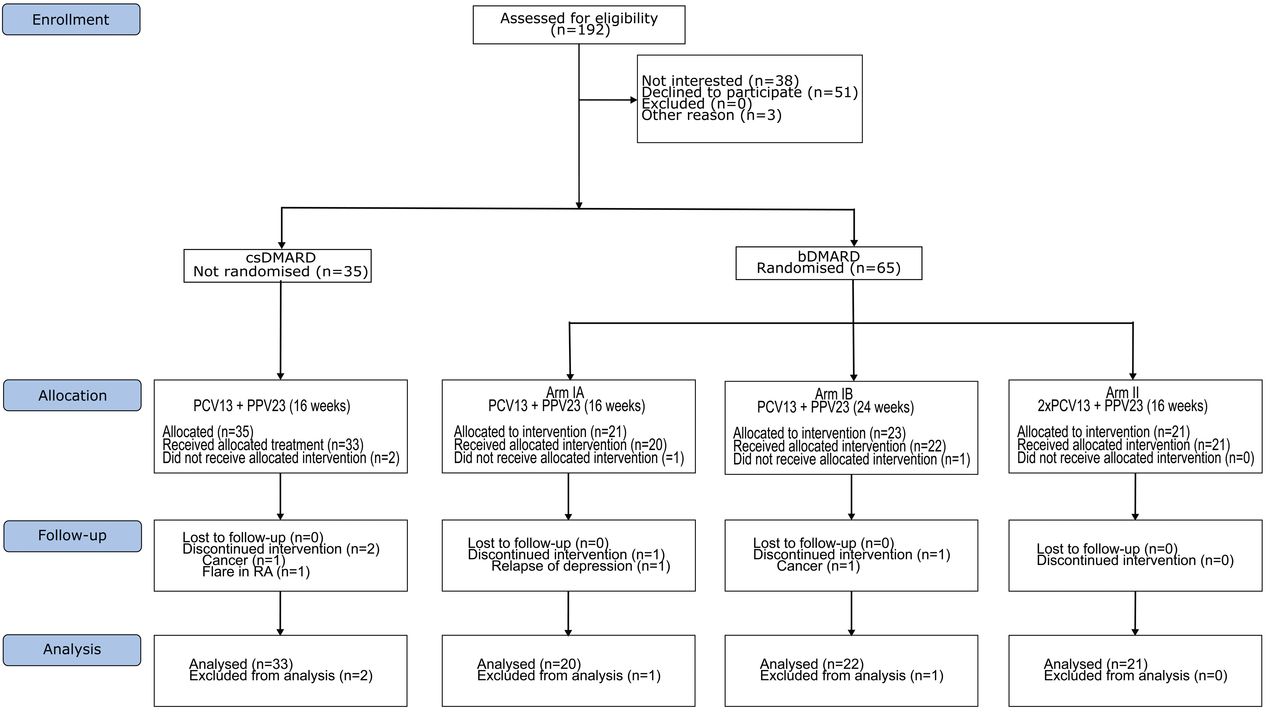
Participants receiving bDMARD treatment were randomized (1:1:1) to immunization with single doses of PCV13 followed by PPV23 after 16 or 24 weeks, or double dose PCV13 followed by PPV23 after 16 weeks (Figure 1). Block randomization ensured similar distributions of participants receiving anti-TNF-α and other bDMARD in each arm using a Web-based computer program hosted at the Odense Patient data Explorative Network (OPEN). A comparison group of patients with RA treated with csDMARD was immunized with a single dose of PCV13 followed by PPV23 after 16 weeks (Figure 1).

Enrollment and study flow of the participants. DMARD: disease-modifying antirheumatic drug; csDMARD: conventional synthetic DMARD; bDMARD: biological DMARD; PCV13: 13-valent protein-conjugated pneumococcal vaccine; PPV23: 23-valent polysaccharide pneumococcal vaccine; RA: rheumatoid arthritis.
We recruited participants through a previous survey about patient awareness of vaccinations26. Men and nonpregnant women aged > 18 years with RA treated with either csDMARD and/or bDMARD were enrolled.
Treatment with csDMARD included MTX, sulfasalazine, hydroxychloroquine, leflunomide, low-dose prednisolone (PSL), and their combinations27. For participants treated with csDMARD, a positive IgM rheumatoid factor or anticyclic citrullinated peptide antibodies was required to substantiate the RA diagnosis. Treatment with bDMARD included RTX, anti-TNF-α, anti-IL-6, or CTLA-4 inhibitors. Participants treated with bDMARD combined with a csDMARD were assigned to the bDMARD group. Exclusion criteria included pneumococcal vaccination within the last 12 months.
The PCV13 vaccine (Pfizer), 0.5 ml, contains polysaccharides of serotypes 1, 3, 4, 5, 6A, 6B, 7F, 9V, 14, 18C, 19A, 19F, and 23F. The PPV23 vaccine (Sanofi Pasteur), 0.5 ml, contains the same serotypes as PCV13 (except 6A) and 11 additional serotypes: 2, 8, 9N, 10A, 11A, 12F, 15B, 17F, 20, 22F, and 33F.
Both vaccines were administered as an intramuscular injection in the deltoid or the gluteus maximus muscle. For participants assigned to the double dose of PCV13, the second dose was administered simultaneously in the opposite side. At all visits, safety, adverse effects, and serious adverse effects were assessed.
Serum was collected before and 4 weeks after each vaccination for both vaccines and stored at −80°C.
Pneumococcal serotype-specific IgG concentrations were determined for 12 serotypes (1, 3, 4, 5, 6B, 7F, 9V, 14, 18C, 19A, 19F, and 23F) included in both the PCV13 and the PPV23 vaccines using an in-house Luminex method28. This method permits the simultaneous measurement of all 12 analytes in a single sample. Shortly described, pneumococcal polysaccharides purchased from LGC Standards (American Type Culture Collection) or from SSI Diagnostica were conjugated to poly-l-lysine, and then covalently bound to carboxylated microspheres (Luminex). Serum samples were incubated with the conjugated microspheres, followed by incubation with R-phycoerythrin conjugated anti-human IgG (Jackson Immuno-Research Laboratories). Finally, the microspheres were read on a Bio-Plex 200 system (Bio-Rad). Data were acquired using Bio-Plex Manager 5.0 (Bio-Rad). Pneumococcal polysaccharide serum calibrated to FDA89SF reference serum was used as a reference. Serum IgG concentrations were calculated using a standard curve of median fluorescent intensity against expected IgG concentration for FDA89SF and converted to μg/ml. Each sample was analyzed in duplicate, and repeated if the coefficient of variation between duplicate was > 20%.
At baseline, we obtained demographic characteristics and RA-related data from the survey and added data from the DANBIO registry, including data on sex, age, ethnicity, tobacco and alcohol consumption, comorbidities, medication for comorbidities, RA disease duration, Health Assessment Questionnaire score (HAQ), Disease Activity Score at 28 joints (DAS28), C-reactive protein (CRP), and prior and current RA treatment (drug name and duration of the treatment period). Data were collected and managed using REDCap electronic data capture tools (REDCap Software version 6.5.10) hosted at OPEN29.
The primary endpoint was proportion of participants in each treatment group responsive to ≥ 6 of 12 antipneumococcal antibody serotypes at Week 4 after completion of the prime-boost vaccination series. A positive serological response was defined as a 4-fold increase from baseline or achieving a level of > 0.35 mg/l30. Secondary endpoints included the proportion of participants responding to individual antipneumococcal antibody serotypes.
A sample size of 100 participants, 65 of whom were in the randomized controlled trial (RCT), was based on similar studies conducted with other RA treatments, and assumed serological response to ≥ 6 of 12 serotypes in 70%13,14,17,19,21,22,24,25. The study was designed to be able to demonstrate, with 80% statistical power and α = 0.05, a 10% difference in vaccine response (defined as the proportion achieving serological response to ≥ 6 of 12 antipneumococcal antibody serotypes) between the bDMARD and csDMARD treatment groups, and a 20% difference in vaccine response between the 3 randomized arms.
Descriptive statistics are presented along with 95% CI for vaccine response. For variables that were not normally distributed, the median (range) was reported. For binary variables, the number (%) of participants was listed relatively to the total number of participants.
Serological responses for pneumococcal antibodies were log-transformed and tested with Shapiro-Wilk test for normality. The geometric mean concentration (GMC) and geometric mean fold rise for each serotype were calculated before and 4 weeks after both vaccinations. Differences in serological outcome between the 3 randomization arms, the 2 treatment groups, and in subgroup analysis for the bDMARD were tested using 2-sample t test or Fisher’s exact test as appropriate. Data were analyzed in STATA version 14 (StataCorp LP).
The study was conducted in accordance with the Declaration of Helsinki and the International Conference on Harmonisation Tripartite Guideline for Good Clinical Practice. Signed informed consent was obtained from all participants.
The study was approved by the Danish Data Protection Agency (14/2736), the Regional Committees on Health Research Ethics for Southern Denmark (S-20140110), and the Danish Health and Medicines Authority (2014070478). The trial is registered at the European Clinical Trial Database (EudraCT 2014-001299-79).
RESULTS
We enrolled 100 participants into the study (Figure 1). The 65 participants treated with bDMARD were randomized to immunization with PCV13 followed by PPV23 after 16 weeks (arm IA, n = 21), immunization with PCV13 followed by PPV23 after 24 weeks (arm IB, n = 23), or immunization with double dose of PCV13 followed by PPV23 after 16 weeks (arm II, n = 21). The comparison group treated with csDMARD (n = 35) received immunizations similar to arm IA.
The per-protocol population (Figure 1) comprised 96 participants (63 of bDMARD treated participants: 20 in arm IA, 22 in arm IB, 21 in arm II; and 33 in the csDMARD comparison group). A total of 4 participants dropped out of the study owing to comorbidities.
Baseline demographics and disease characteristics were similar among participants in the 3 arms, and although PSL use ranged from 10–29%, the prevalence of MTX as comedication was comparable (Table 1) among the 3 arms. The majority of participants were women (65%) with a median age of 62 years (range 23–82), with low disease activity score (DAS28 median 2.45) and median disease duration of 12 years (range 0.5–33). The mean duration of current treatment was longest for participants treated with anti-TNF-α (61 mos), RTX (55 mos), and MTX (73 mos), and shorter for the bDMARD anti-IL-6 (15 mos) and CTLA-4 (12 mos).
Characteristics and demography of the participants at baseline.
While demographic characteristics were very similar for the csDMARD-treated group, disease duration was considerably shorter (median 7 yrs) compared with the bDMARD group (p = 0.02; Table 1). Prior number of bDMARD treatments was similar among the csDMARD and bDMARD group with a median of 1 (range 0–5).
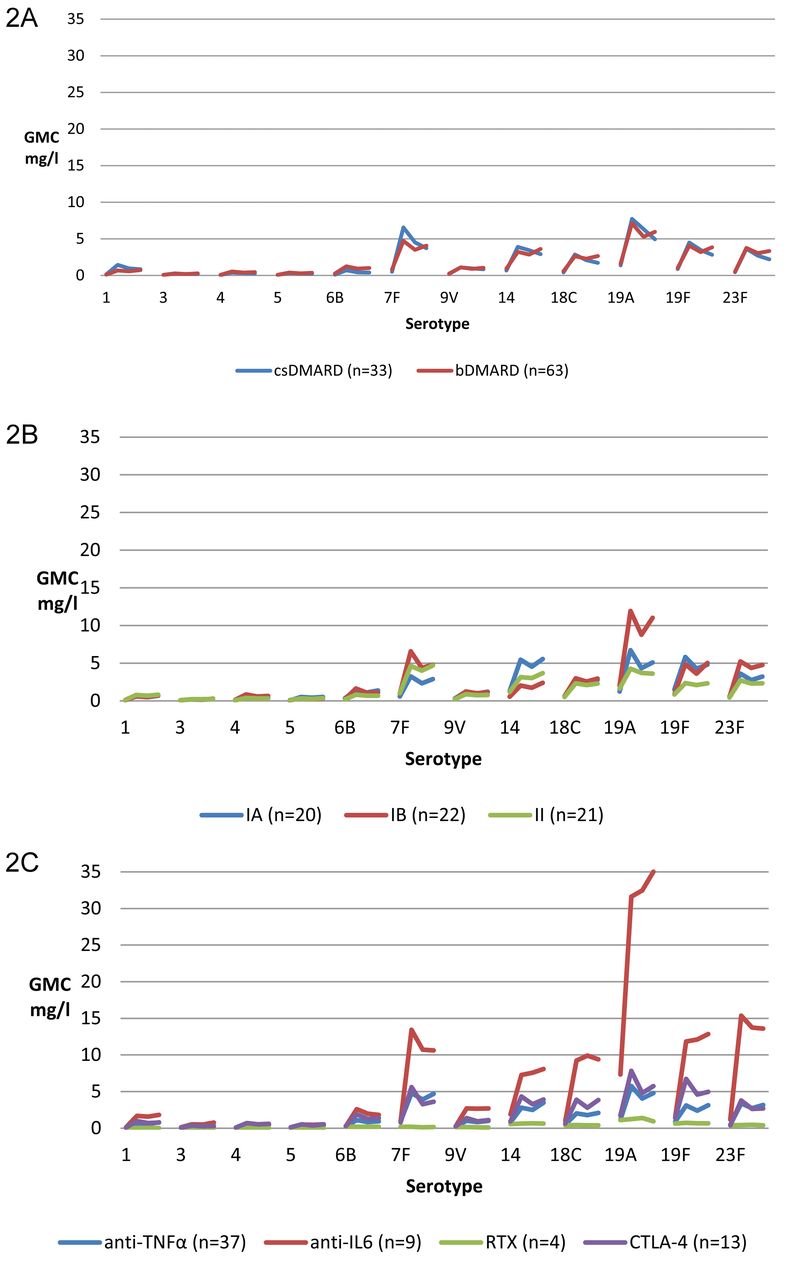
Proportions of participants responding to individual antipneumococcal antibody serotypes were comparable between the 2 treatment groups (< 10% difference between groups) for all serotypes (Figure 2A). The proportion of responders to serotypes 7F, 14, 19A, 19F, and 23F differed according to randomization arm (> 10% difference; Figure 2B), with lower responses observed for arm II (double PCV13 dose) compared to arm IA and IB. Participants treated with anti-IL-6 had the highest antibody titers in the bDMARD group (Figure 2C; Supplementary Table 1, available with the online version of this article). Overall, the initial prime PCV13 vaccination induced a significant increase in antipneumococcal antibody GMC, whereas the subsequent effect of boosting with PPV23 was limited (Figure 2A–C; Supplementary Table 2, available with the online version of this article).

Serotype specific IgG GMC pre-PCV13, post-PCV13, pre-PPV23, and post-PPV23 vaccination by pneumococcal serotypes (mg/l) according to (A) treatment with csDMARD or bDMARD; (B) randomization arm IA, IB, or II; and (C) to anti-TNF-α, anti-IL-6, RTX, or CTLA-4. GMC: geometric mean concentration; PCV13: 13-valent protein-conjugated pneumococcal vaccine; PPV23: 23-valent polysaccharide pneumococcal vaccine; DMARD: disease-modifying antirheumatic drug; csDMARD: conventional synthetic DMARD; bDMARD: biological DMARD; anti-TNF-α: antitumor necrosis factor-α; anti-IL-6: interleukin 6 inhibitors; RTX: rituximab, anti-CD20 monoclonal antibody; CTLA-4: abatacept, T cell lymphocyte costimulation inhibitor.
After completion of the vaccination series, 87% (95% CI 0.76–0.94) and 94% (95% CI 0.77–0.99), respectively, of participants treated with bDMARD and csDMARD had responded to ≥ 6/12 pneumococcal serotypes (primary endpoint), with insufficient evidence for any difference according to the RA-treatment group (7.0%, 95% CI −0.5 to 19; Figure 3A).

Proportions of participants responding to pneumococcal serotype combinations from 1–12 according to (A) treatment with csDMARD or bDMARD; (B) randomization arm IA, IB, or II; and (C) anti–TNF-α, anti–IL-6, RTX, or CTLA-4 treatment. Response defined as a 4-fold rise in geometric mean concentration from baseline or a geometric pneumococcal antibody concentration > 0.35 mg/l. DMARD: disease-modifying antirheumatic drug; csDMARD: conventional synthetic DMARD; bDMARD: biological DMARD; anti-TNF-α: antitumor necrosis factor-α; anti–IL-6: interleukin 6 inhibitors; RTX: rituximab, anti-CD20 monoclonal antibody; CTLA-4: abatacept, T cell lymphocyte costimulation inhibitor.
Among participants receiving bDMARD, there were no significant differences in reaching the primary endpoint between the 3 randomization arms with response in 85% (95% CI 0.80–0.89), 86% (95% CI 0.82–0.90), and 90% (95% CI 0.87–0.93), respectively (Figure 3B).
Participants treated with RTX, anti-TNF-α, CTLA-4, and anti-IL-6 responded to ≥ 6/12 serotypes in 25% (95% CI 0.04–0.96), 89% (95% CI 0.74–0.96), 92% (95% CI 0.53–0.99), and 100%, respectively. The overall number of participants in subgroups was small and the difference did not reach statistical significance (p = 0.4; Figure 3C). In additional posthoc analyses, serological responses among participants receiving anti-TNF-α or CTLA-4 with concomitant MTX (90%, 95% CI 0.73–0.97 and 100%, 95% CI 1.0–1.0 responding to ≥ 6/12 pneumococcal serotypes) were very similar to responses among recipients of anti-TNF-α or CTLA-4 without concomitant MTX (80%, 95% CI 0.11–0.99 and 80%, 95% CI 0.11–0.99; Figure 4). However, the differences were not statistically significant. There was no significant difference in serological response according to concomitant PSL use in combination with either bDMARD or other csDMARD (data not shown).
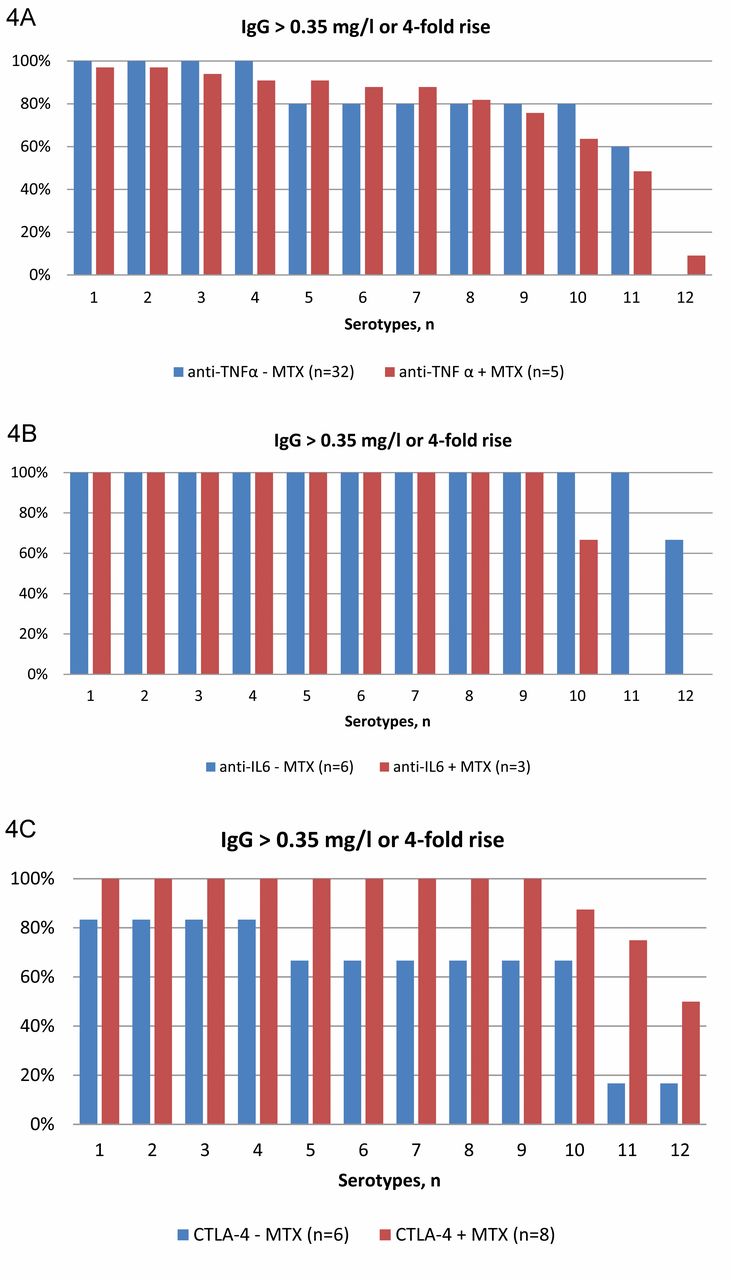
Proportions of participants responding to pneumococcal serotype combinations from 1–12 according to (A) concomitant MTX treatment ± with anti-TNF-α; (B) concomitant MTX treatment ± with anti-IL-6; and (C) concomitant MTX treatment ± with CTLA-4. Response defined as a 4-fold rise in geometric mean concentration from baseline or a geometric pneumococcal antibody concentration > 0.35 mg/l. MTX: methotrexate; anti-TNF-α: antitumor necrosis factor-α; anti-IL-6: interleukin 6 inhibitors; CTLA-4: abatacept, T cell lymphocyte costimulation inhibitor.
When stratified by age, participants aged > 60 years had 5% fewer responders compared to participants aged ≤ 60 years, irrespective of type of RA treatment, although the difference was not significant (p = 0.36). There were no significant associations of demographic or RA-related factors with vaccination response when tested in a logistic regression model (data not shown).
A total of 404 adverse events (AE) were reported in 93 participants within the first 6 months after both vaccinations, of which 248 were considered vaccine-related; 94% of the related AE were listed as common adverse effects associated with vaccination, including soreness (54%), swelling (9%), itching (3%), erythema (10%), and flu-like symptoms (18%). Four participants experienced arthralgia related to pneumococcal vaccination (1 after PCV13 vaccination and 3 after PPV23 vaccination) corresponding to 1.6% of the vaccine-related AE. Ninety-four percent of the related AE were resolved within 7 days after vaccination. Twenty-one serious AE (SAE) were experienced by 16 participants. None of the SAE were related to any of the study drugs, but rather were related to comorbidity.
DISCUSSION
Our results indicate that prime-boost pneumococcal vaccination of patients with RA receiving immunosuppressive therapy is safe and immunogenic, with a high prevalence of adequate early responses to vaccination in all assessed treatment groups, although notable differences were observed according to individual bDMARD. The early serological response to prime-boost vaccination with PCV13 followed by PPV23 was very similar among participants treated with bDMARD and csDMARD, with more than 85% responders to ≥ 6/12 pneumococcal serotypes in each group. Among participants treated with bDMARD, we observed similar serological responses irrespective of an interval of 4 or 6 months between prime PCV13 and boost PPV23 vaccination, and of single or double dose of the prime PCV13 vaccination.
In accordance with other studies, we found severely impaired serological response in RTX-treated participants, while initial responses to pneumococcal vaccination were generally good among participants treated with anti-TNF-α, anti-IL-6, CTLA-4, or csDMARD. The positive response in all participants treated with anti-IL-6 is consistent with the notion that IL-6 is not essential for antibody production in B cells. Further, anti-IL-6 treatment may not entirely inhibit IL-6 signaling in the lymphoid tissue where the vaccine response is induced13,22. In contrast to our study, previous studies have investigated either responses to PCV7/PCV13 or to PPV23, but not to the combined prime-boost series of both PCV13 and PPV23; however, despite this difference, the magnitude of the initial responses for participants treated with RTX, anti-TNF-α, anti-IL-6, or CTLA-4 in our study was very similar to those in earlier reports12,13,14,17,18,19,22,24,25.
Results from other studies of vaccine responses in patients with RA suggest that although humoral responses are reduced, T cell responses to vaccine antigens may be similar with RTX compared with other bDMARD. In our study, we found that RTX treatment significantly impaired the serological response after prime-boost vaccination with PCV13 and PPV23, with no notable change in GMC after each vaccination. Participants had received RTX infusion 15–146 days prior to the PCV13 vaccination. Other clinical trials have reported impaired serological response even 6 months after the last RTX infusion12,13,31,32.
While PPV23 induces only serotype-specific antibodies, PCV13 conceivably stimulates the formation of both serotype-specific antibodies and B memory cells, which are associated with a longer duration of vaccine-induced immune responses. Previous studies found lower persistence of protective immunity in patients treated with the combination of MTX and anti-TNF-α17,25,33. Here, we found that concomitant MTX treatment did not decrease early serological responses among participants receiving anti-TNF-α or CTLA-4. The findings are not necessarily at odds, and additional followup is warranted to analyze the persistence of the response observed in our study. However, potential discrepancies may be related to the prime-boost combination of PCV13 and PPV23 as applied in our study, differences in patient characteristics, and disease severity between studies. Further, there is an imbalance in the number of participants receiving bDMARD with or without concomitant MTX because the effect of concomitant MTX treatment on serological response was not part of our prespecified analysis plan. The numbers of participants included in these subgroup analyses were 32 and 5, respectively, receiving anti-TNF-α as mono- and combination therapy with MTX, and 3 and 6 participants received anti-IL-6 as mono- or combination therapy with MTX.
Surprisingly, we found that doubling the dose of PCV13 did not elicit an increased serological response 4 weeks after vaccination (arm II) compared to a single dose of PCV13 (arm IA and IB). This is in contrast with a previous study investigating the immunogenicity of 0.5 ml (conventional dose), 1 ml, and 2 ml of PCV7 in immunocompetent elderly aged 70–79 years. Our study showed that 1 ml of PCV7 elicited significantly higher antibody levels compared to 0.5 ml34. Hypothetically, our finding may reflect hyporesponsiveness, similar to reduced responses to PCV13 following PPV23 vaccination35. In our study, the additional PCV13 dose was administered in the opposite limb, and hence would lead to simultaneous stimulation of dendritic cells and subsequently of B cells in the draining lymph nodes bilaterally. To our knowledge, it has not previously been described that this type of co-administration should lead to impaired reaction in the germinal center, but our finding may merit further study. Sequential administration of PCV13 in opposite limbs during infant vaccination has not been associated with a decreased vaccination response36.
Current guidelines recommend an interval of at least 8 weeks between vaccination with PCV13 and PPV23. However, the recommendations are based on a study with a 1-year interval between prime PCV13 and booster PPV23 vaccination37. Another study investigated the serological response after boosting with PCV13 or PPV23 4 years after the initial PCV13 vaccination. This showed comparable or significantly higher antipneumococcal opsonophagocytic activity (OPA) than after the initial PCV13 vaccination. Our study did not find any difference in GMC after boosting with PPV23 after 4 months compared to 6 months. The recommendations for timing of the booster vaccination with PPV23 must ensure adequate time for maturation of the T helper cells in the T cell dependent response after PCV13 vaccination; our findings suggest that the current recommendations are adequate, although the duration of the memory response requires further study.
Our study had several limitations. Our sample size was restricted, and hence we had limited power in subgroup analyses. We assessed quantity but not the quality of the pneumococcal antibodies (OPA). Our baseline characteristics drawn from DANBIO were incomplete, with incomplete records of prior treatment history of csDMARD and bDMARD before January 2006. CRP and hence DAS28 were absent for some patients. However, we do not think that any of these factors have affected our results. Further, we did not include healthy controls.
The strengths of our study included the homogeneous group of participants all diagnosed with RA. Although the csDMARD comparison group was not randomized, the characteristics of participants in this group were very similar to the bDMARD group, the only difference being a shorter RA disease duration, but the HAQ and DAS28 were similar. The dropout rate was very modest, and thus we achieved almost complete followup of the enrolled participants.
Early responses to prime-boost pneumococcal vaccination in patients with RA treated with bDMARD or csDMARD were adequate when the vaccines were administered at standard doses and intervals. However, additional assessment of pneumococcal vaccinations with a special focus on the intervals between vaccinations in the context of combined conjugate/polysaccharide vaccine schedules is needed, in particular focusing on the durability of the vaccine response. Our finding of a similar or potentially better vaccination response in patients treated with MTX in combination with anti-TNF-α or CTLA-4 is intriguing, but requires followup for the assessment of persistence and also confirmation in larger studies.
Our data clearly indicate that — with the exception of RTX — sufficient early serological response to prime-boost pneumococcal vaccination could be achieved despite ongoing bDMARD treatment, and thus catchup vaccination is possible. However, because bDMARD may increase the risk of pulmonary infections while also delaying the diagnosis as a result of masking of inflammatory symptoms, we highly recommend providing vaccinations early on and preferably before initiating immunosuppressive treatment.
ONLINE SUPPLEMENT
Supplementary material accompanies the online version of this article.
Acknowledgment
We thank data manager Peter Bjødstrup Jensen from the Odense Patient data Explorative Network, study nurse Nete Bülow from the Department of Infectious Diseases, study nurse Henriette Cederholm from the Department of Rheumatology, and study nurse Susanne Leed Henriksen from the Department of Rheumatology at Odense University Hospital.
Footnotes
This study was funded by the University of Southern Denmark, the Region of Southern Denmark, and Odense University Hospital.
- Accepted for publication July 10, 2017.








{kind=link}
{kind=link}
{kind=link}
{kind=link}