

Abstract
Objective. Several studies have reported risk factors for hydroxychloroquine (HCQ) retinal toxicity, but data are limited for patients of Asian ancestry. The aim of this study was to investigate the rate of and factors for HCQ retinal toxicity in the Korean population.
Methods. There were 123 patients enrolled in this study who were using or had used HCQ. Retinal toxicity was detected using spectral domain optical coherence tomography, fundus autofluorescence, multifocal electroretinography, and automated visual field testing. Binary logistic regression analysis was performed to identify factors associated with HCQ retinal toxicity.
Results. Mean duration of HCQ use and mean HCQ dose in study participants was 10.1 years and 6.4 mg/kg, respectively. We found 17 patients (13.8%) with HCQ retinal toxicity among 123 patients. Patients with retinal toxicity took HCQ ranging from 6.7–21.9 years and daily dosage ranging from 4.9–9.1 mg/kg. Only 1 patient had retinal toxicity among patients with daily dose < 5.0 mg/kg. These factors increased the risk of HCQ retinal toxicity: longer duration of HCQ use [adjusted OR (aOR) = 4.71, 95% CI 2.18–10.15 for duration of HCQ use in 5-yr increments], higher daily HCQ dose (aOR = 3.34, 95% CI 1.03–10.80 for daily HCQ dose in 100-mg increments), and the presence of kidney disease (aOR = 8.56, 95% CI 1.15–64.00).
Conclusion. HCQ retinal toxicity is associated with duration of HCQ use, daily HCQ dose, and presence of kidney disease. Proper dosing of maximum 5 mg/kg and regular screening according to risk factors are important in HCQ use.
Hydroxychloroquine (HCQ) is an antimalarial drug commonly used in autoimmune diseases such as systemic lupus erythematosus (SLE) and rheumatoid arthritis. Despite the beneficial effect of HCQ for preventing SLE flares and reducing mortality, retinal toxicity is a major concern1,2. There is no specific treatment for HCQ retinal toxicity other than discontinuing the drug. Retinal toxicity may progress even after cessation of HCQ, leading to increased risk of visual loss3,4. If retinal toxicity is recognized and the drug is stopped prior to retinal pigment epithelial damage or bull’s eye maculopathy, retinal findings may remain stable without progression5. In addition, most patients with retinal toxicity have no visual symptoms until severe damage is done. Therefore early screening is essential. New objective screening modalities including spectral domain optical coherence tomography (SD-OCT), fundus autofluorescence (FAF), and multifocal electroretinography (mfERG) can detect early ocular changes, and have become useful screening techniques with automated visual field testing6.
Recommendations on screening for chloroquine and hydroxychloroquine retinopathy by the American Academy of Ophthalmology were revised in 20167. These revised recommendations suggest several risk factors, including high dose and long duration of use, renal disease, and use of tamoxifen. Recommended maximum daily dose is based on real body weight rather than ideal body weight. These recommendations are based mainly on a study of white people. Patterns of HCQ retinal toxicity vary by race and the pericentral pattern of retinal toxicity is predominant in Asian patients8. Risk of retinal toxicity and the recommended dosage threshold in Asian patients may differ from those of patients of other races. Few studies are available regarding the risk of HCQ retinal toxicity in Asian populations9,10.
In our study, we used new screening modalities to demonstrate the overall risk of retinal toxicity in Korean patients who were longterm HCQ users. We also investigated factors for HCQ retinal toxicity in the Korean population. The results will help determine drug use in clinical practice.
MATERIALS AND METHODS
Study population
This study enrolled patients from Daegu Catholic University Medical Center, a tertiary care hospital in Korea that has a regional rheumatology center. Inclusion criteria were patients with rheumatic diseases who were taking or had taken HCQ and visited an ophthalmologist for screening of retinopathy from August 2015 to September 2016. Exclusion criteria were concomitant retinal diseases including underlying macular degeneration. The study was approved by the Institutional Review Board committee of Daegu Catholic University Medical Center (CR-16-140-L).
Data collection
We investigated demographic features, primary indication for using HCQ, presence of concomitant kidney and liver disease, hypertension (HTN), and diabetes mellitus (DM) by retrospectively reviewing medical records. Duration of HCQ use, and daily and cumulative HCQ dose were calculated using the data from medical records. Kidney disease was defined as reduced estimated glomerular filtration rate below 60 ml/min per 1.73 m2. Liver disease indicated chronic hepatitis with exclusion of transient elevation of liver enzymes and drug-induced hepatitis.
Ophthalmological examination
Ophthalmological examination included 10-2 visual field testing (Humphrey perimeter; Carl Zeiss Meditec Inc.), SD-OCT (Heidelberg Engineering), FAF (Heidelberg Engineering), and mfERG (Retiscan, Roland Consult). Findings of visual field loss varied from subtle defects on the pattern deviation plot to partial or complete ring scotoma sparing central fovea11. SD-OCT examines cross-sectional images of retinal layers. Disruption of perifoveal photoreceptor inner segment/outer segment junction is an early sign of HCQ retinal toxicity. This can be accompanied by thinning of the photoreceptor outer nuclear layer in more advanced retinal toxicity12. FAF imaging detects photoreceptor damage as hyperautofluorescence by accumulated lipofuscin or hypoautofluorescence due to retinal pigment epithelial cell loss13,14. MfERG records multifocal electroretinographic responses, and ring ratio analysis is helpful in detecting early retinal changes15,16. MfERG, which is recommended as an additional useful screening test, is less useful after evident outer retinal disruption appears on SD-OCT14. MfERG is as sensitive as automated visual fields, but it is difficult to perform and interpret well.
Combining the results of examinations, HCQ retinal toxicity was determined by 1 ophthalmologist, an expert in retinal diseases. The pattern of retinal toxicity was described as a parafoveal pattern, pericentral pattern, or mixed pattern of retinal toxicity, according to the location of retinal damage. Severity of retinal toxicity was graded as early (patchy extrafoveal damage shown on visual field or objective testing), moderate (50–100% extrafoveal ring of damage and marked thinning of retina on SD-OCT without retinal pigment epithelial damage), or severe (bull’s eye damage with retinal pigment epithelial damage)5.
Statistical analysis
Data are shown as mean (SD) or median (interquartile range) for continuous variables, and number (percentage) for categorical variables. Normality of data distribution of continuous variables was assessed by Shapiro-Wilk analysis. Characteristics between patients with and without retinal toxicity were compared using the Student t test and the Mann-Whitney U test for continuous variables, and the chi-square test and Fisher’s exact test for categorical variables. Factors associated with retinal toxicity were determined by binary logistic regression analysis. Results are shown as OR with 95% CI. All statistical analyses were performed by IBM SPSS Statistics 18.0 (IBM Corp.). A p value < 0.05 was considered statistically significant.
RESULTS
Risk and pattern of retinal toxicity
Mean duration of HCQ use and mean HCQ dose for study participants was 10.1 years and 6.4 mg/kg, respectively. Among the 123 study participants who received HCQ, 17 patients (13.8%) had retinal toxicity. Most patients had a pericentral pattern (n = 13) of retinal toxicity, and the remaining patients had a mixed pattern (n = 2) or a parafoveal pattern (n = 2). The pericentral pattern of retinal toxicity represented retinal damage in a region > 7° from the center of the fovea, whereas parafoveal pattern of retinal toxicity occurred in a region 2–6° from the center of the fovea8. The mixed pattern of retinal toxicity had both a pericentral and a parafoveal pattern with relatively normal retina in between. Pericentral, mixed, and parafoveal patterns of retinal toxicity in our study population are described in Figure 1. Retinal toxicity was found as the thinning of the outer retinal layer with loss of inner segment/outer segment junction on SD-OCT, hyperautofluorescence on FAF images, and patchy field loss or ring scotomas on visual fields.

Ocular findings of (A) pericentral pattern, (B) mixed pattern, and (C) parafoveal pattern of hydroxychloroquine retinal toxicity. (A) Top to bottom: Superior field loss is located peripherally in pattern deviation plot (10-2 visual field). FAF image shows broad range of hyperautofluorescence in inferior retina. SD-OCT image shows loss of photoreceptor layer in pericentral area (arrow). (B) Top to bottom: 10-2 visual fields (threshold and pattern deviation plot) are showing full ring scotomas. FAF image shows ring-shaped hyperautofluorescence in parafoveal area (dashed curves) with diffuse hyperautofluorescence in pericentral area (dashed curves). SD-OCT image shows disruption of photoreceptor layer with loss of outer nuclear layer in both parafoveal and pericentral retina (arrows). RPE damage is combined at the extrafoveal region. (C) Top to bottom: 10-2 visual fields (threshold and pattern deviation plot) are showing patchy parafoveal scotomas. Hyperautofluorescence are shown at a region just inferior to macula on FAF image. SD-OCT image shows parafoveal disruption of photoreceptor layer with loss of outer nuclear layer (arrow). RPE damage is suspected within the parafoveal retina. FAF: fundus autofluorescence; SD-OCT: spectral domain optical coherence tomography; RPE: retinal pigment epithelium.
Characteristics of the patients with and without retinal toxicity
Demographic and clinical characteristics of patients with and without retinal toxicity are compared in Table 1. Patients with retinal toxicity were older than patients without retinal toxicity (mean age 56.2 vs 50.3 yrs, p = 0.045). Sixteen patients (94.1%) and 102 patients (96.2%) were women in each group, respectively. Body weight was not significantly different between patients with and without retinal toxicity. Mean daily HCQ dose was 7.2 mg/kg (range 4.9–9.1) and mean duration of HCQ use was 15.2 years (range 6.7–21.9) in patients with retinal toxicity. Patients with retinal toxicity had a higher daily HCQ dose (p = 0.019), daily HCQ dose adjusted by body weight (p = 0.035), cumulative HCQ dose (p < 0.001), and a longer duration of HCQ use (p < 0.001) than patients without retinal toxicity. Kidney disease (p = 0.011) and HTN (p = 0.017) were more common in patients with retinal toxicity. The primary indication for HCQ use, presence of liver disease, and presence of DM were not significantly different between groups. Table 2 gives demographic features, clinical diagnosis for drug use, and drug use of patients with retinal toxicity. Results of ophthalmologic screening tests were also described with the severity of retinal toxicity.
Comparison of characteristics between patients with and without retinal toxicity.
Characteristics of patients with retinal toxicity.
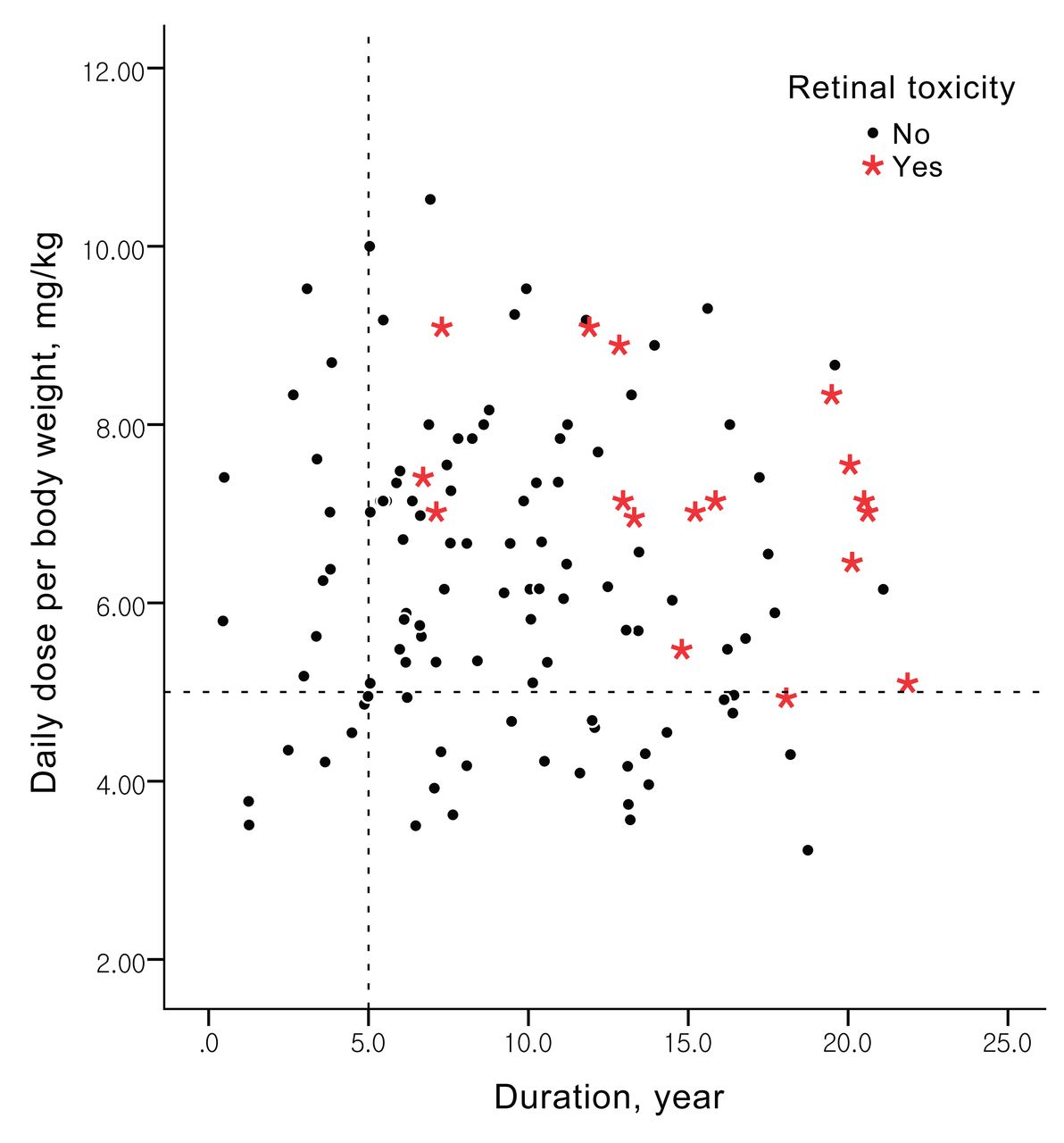
Distribution of study participants was marked according to the duration of their HCQ use and daily dose per body weight (Figure 2). There was only 1 patient with retinal toxicity among patients who received an HCQ dose below 5 mg/kg. She took 4.9 mg/kg for a long duration (18.1 yrs). Patients with retinal toxicity took HCQ for at least 6 years. There was no retinal toxicity among patients who took HCQ for < 5 years.

Distribution of study participants according to duration and daily dose per body weight of hydroxychloroquine. Red stars and black dots indicate patients with and without retinal toxicity, respectively. Dashed lines indicate 5 years of duration (X axis) and a 5-mg/kg daily dose per body weight (Y axis).
Factors associated with retinal toxicity
These factors were associated with retinal toxicity on univariable logistic regression analysis (all p < 0.05): duration of HCQ use, cumulative HCQ dose, daily dose adjusted by body weight, presence of kidney disease, and presence of HTN. We performed multivariable logistic regression analysis on factors with difference of p value < 0.2 by univariable analysis. Increasing the risk of retinal toxicity were longer duration of HCQ use [adjusted OR (aOR) = 4.71, 95% CI 2.18–10.15 for duration of HCQ use in 5-yr increments], higher daily HCQ dose (aOR = 3.34, 95% CI 1.03–10.80 for daily HCQ dose in 100-mg increments), and presence of kidney disease (aOR = 8.56, 95% CI 1.15–64.00; Table 3). Age and body weight were not associated with retinal toxicity.
Factors associated with retinal toxicity (multivariable logistic regression analysis).
DISCUSSION
An early study documented 0.65% of definite or probable retinal toxicity with HCQ use17. Retinal toxicity was identified by questioning patients on whether they had been diagnosed with retinal toxicity and confirming when there was bull’s eye maculopathy or visual field loss. As sensitive screening methods have been introduced, retinal toxicity is found earlier and seems to have become more common. Our present study showed a 13.8% retinal toxicity among longterm users of HCQ, who were often overdosed relative to ophthalmologic guidelines. A long duration of HCQ use, a high daily HCQ dose, and the presence of kidney disease were associated with retinal toxicity.
A large retrospective study enrolled 2361 patients who had used HCQ for at least 5 years and demonstrated an overall rate of 7.5% retinal toxicity18. With intermediate daily dosage, the risk was < 2% within the first 10 years. However, the risk increased to almost 20% after 20 years of HCQ use. With a higher daily dosage, the risk of retinal toxicity approached 40% after 20 years of use. Our study enrolled longterm HCQ users and has a higher rate of retinal toxicity compared to the aforementioned study, which can be attributed to the higher daily HCQ dosage of our study population. Two reasons may account for the higher daily dosage observed. One reason was that we did not consider drug compliance. Using the prescribed dosage rather than consumed dosage likely gives a higher daily dosage than real consumption of HCQ. Another reason was the lower body weight of the study population, and they were often highly overdosed without considering the weight of individuals. The same HCQ dosage in patients with lower body weight results in a higher daily dosage per body weight.
Several studies have emphasized daily dosage as a risk factor for retinal toxicity. A study from Melles and Marmor reported that using real body weight for calculating daily dose is a better predictor of retinal toxicity, with 5.0 mg/kg of real body weight as the maximum recommended dose18. The risk of retinal toxicity predicted by daily dose per real body weight was independent of body habitus. Our present study showed that daily dosage was associated with retinal toxicity after adjusting other confounding factors such as duration of HCQ use, presence of concomitant diseases, age, and body weight. No retinal toxicity was identified in patients with daily dosage < 5.0 mg/kg in our study, except for 1 patient. Daily dosing should be determined individually by body weight.
Even at recommended doses, long-duration HCQ use contributes to retinal toxicity. In a prospective cohort study, retinal toxicity was assessed among patients who received the recommended dose19. They had no retinal toxicity during a followup period of 6 years. HCQ retinal toxicity developed in 2 patients at 8 years and 6.5 years of treatment, despite taking the recommended dose of HCQ. We reported duration of HCQ use was still associated with retinal toxicity (4.7 of OR in 5-yr increments of duration of HCQ use) after adjusting other confounding factors including daily dose. There was no retinal toxicity before 5 years of HCQ use in our present study. Our study supports the current recommendations that suggest starting annual screening after 5 years of HCQ use and earlier if other major risk factors exist7.
Concomitant diseases may affect the development of retinal toxicity because of HCQ. Kidney disease is known as a risk factor for retinal toxicity18. In our present study, patients with kidney disease had OR 8.6 for retinal toxicity compared with those who did not have kidney disease. Because HCQ is cleared primarily by the kidneys, decreased renal function can easily lead to retinal toxicity. A patient with SLE and renal failure who was administered HCQ < 6.5 mg/kg developed retinal toxicity before 5 years of HCQ therapy20. Our study also found a possible relationship between HTN and retinal toxicity. HTN was more common in patients with retinal toxicity than those without retinal toxicity. However, the mechanism of this relationship is unclear. Oxidative stress and endothelial dysfunction were speculated as promoters of toxicity in a study that also reported a positive relation between HTN and retinal toxicity21. Physicians should be aware of the risk in patients with kidney disease or HTN and perform early screening for retinal toxicity.
There are several limitations in our study. First, the study was performed in a relatively small study population at a single center. Second, no consideration of drug compliance might have overestimated the daily dosage of HCQ use. Third, automated visual field testing should have been performed in wider patterns (24-2 or 30-2) rather than 10-2 visual fields. Asian patients with retinal toxicity are likely to have peripheral defects beyond the macula8. Early toxicities may have been unrecognized until definite sign of toxicity appears inside 10° from the macula.
Despite these limitations, our study has important implications. Risk factors for HCQ retinal toxicity were well evaluated in an Asian population and the results were mostly consistent with those of the large study from Melles and Marmor18. Our study shows that duration and dosage are the main factors associated with HCQ retinal toxicity. Concomitant diseases such as kidney disease should be considered in patients receiving HCQ. Additionally, our study confirms the use of the recommended dose of 5 mg/kg and to start annual screening after 5 years of use. Informing rheumatologists of these findings is important.
HCQ retinal toxicity is infrequent in proper dose and short duration of HCQ use. However, the toxicity is increased with longer duration of HCQ use, higher daily HCQ dose, and presence of kidney disease. Rheumatologists should focus on the recommended dosage of HCQ ≤ 5 mg/kg and start regular ophthalmologic screening according to the risk factors. Effective screening is important for early detection of retinal toxicity and proper decision making about drug discontinuation.
- Accepted for publication June 1, 2017.








{kind=link}
{kind=link}