

Abstract
Objective. Because the association and its clinical relevance between comorbidities and primary hand osteoarthritis (OA) disease burden is unclear, we studied this in patients with hand OA from our Hand OSTeoArthritis in Secondary care (HOSTAS) cohort.
Methods. Cross-sectional data from the HOSTAS study were used, including consecutive patients with primary hand OA. Nineteen comorbidities were assessed: 18 self-reported (modified Charlson index and osteoporosis) and obesity (body mass index ≥ 30 kg/m2). Mean differences were estimated between patients with versus without comorbidities, adjusted for age and sex: for general disease burden [health-related quality of life (HRQOL), Medical Outcomes Study Short Form-36 physical component scale (0–100)] and disease-specific burden [self-reported hand function (0–36), pain (0–20; Australian/Canadian Hand OA Index), and tender joint count (TJC, 0–30)]. Differences above a minimal clinically important improvement/difference were considered clinically relevant.
Results. The study included 538 patients (mean age 61 yrs, 86% women, 88% fulfilled American College of Rheumatology classification criteria). Mean (SD) HRQOL, function, pain, and TJC were 44.7 (8), 15.6 (9), 9.3 (4), and 4.8 (5), respectively. Any comorbidity was present in 54% (287/531) of patients and this was unfavorable [adjusted mean difference presence/absence any comorbidity (95% CI): HRQOL −4.4 (−5.8 to −3.0), function 1.9 (0.4–3.3), pain 1.4 (0.6–2.1), TJC 1.3 (0.4–2.2)]. Number of comorbidities and both musculoskeletal (e.g., connective tissue disease) and nonmusculoskeletal comorbidities (e.g., pulmonary and cardiovascular disease) were associated with disease burden. Associations with HRQOL and function were clinically relevant.
Conclusion. Comorbidities showed clinically relevant associations with disease burden. Therefore, the role of comorbidities in hand OA should be considered when interpreting disease outcomes and in patient management.
Hand pain and impaired function are major problems in patients with hand osteoarthritis (OA)1. A wide range of factors have been shown to be associated with these complaints. These are not limited to joint-specific factors such as bony enlargements, inflammation, and radiographic damage, but also include psychosocial factors such as coping and illness perceptions2,3,4,5. Another factor that could play a role is comorbidity. Comorbidity (i.e., any additional disease co-occurring with a primary disease) or multimorbidity (i.e., 2 or more co-occurring medical conditions in 1 patient) is associated with disease outcomes6 and has a clinical role in patient management, as was recently recognized by a European League Against Rheumatism initiative on comorbidities in chronic inflammatory rheumatic diseases7. Patients with OA could also benefit when comorbidities such as cardiovascular (CV) disease and osteoporosis are taken into consideration7.
Multimorbidity, including depression8,9, has been investigated in many population-based studies, showing associations between presence of multimorbidity and increased disease burden8,10,11,12. In these studies, disease burden was either defined as general burden [health-related quality of life (HRQOL)] or as disease-specific burden (e.g., functional ability6). Because many patients with hand OA are elderly, comorbidity in these patients is likely to occur13,14,15,16. Despite this situation, the relationship between comorbidity and disease-specific burden in hand OA, i.e., impaired hand function and hand pain, is scarcely studied.
In patients with OA at other sites, i.e., knee and hip OA, it is reported that musculoskeletal comorbidities such as back disorders and osteoporosis, but also nonmusculoskeletal comorbidities such as diabetes mellitus, chronic pulmonary disease, and depression, are associated with decreased HRQOL and increased disability and joint pain17,18,19,20,21,22. Although many patients with OA who consult a rheumatologist may have hand OA1,23, previous research only studied associations between hand OA and a few comorbidities, including generalized OA23, depression, upper extremity comorbidity24, and diabetes25. The clinical relevance of the role of these comorbidities was not studied.
Insight into the role of comorbidities in hand OA disease burden is not only important from a clinical perspective, but also from a methodological one. When comorbidities act as effect modifiers of disease outcomes, they can be considered as contextual factor(s). These factors, influencing outcome interpretation, should be taken into account in clinical trials and observational studies7,26,27.
Therefore, we aimed to study the association between comorbidities and general HRQOL, as well as disease-specific burden (hand function and hand pain) in patients with hand OA. First, we will describe the clinical characteristics and prevalent comorbidities in a large cohort of primary hand OA patients from our outpatient clinic. Second, we will estimate the cross-sectional association between presence and number of comorbidities or specific types of comorbidities and hand OA disease burden. Third, we will evaluate the clinical relevance of the results.
MATERIALS AND METHODS
Study population and recruitment
Baseline data from the Hand OSTeoArthritis in Secondary care (HOSTAS) study were used, an observational cohort aiming at investigating determinants of outcome and utility of clinimetric instruments in primary hand OA. Consecutive patients from the Leiden University Medical Center (LUMC) outpatient clinic were included between June 2009 and October 2015. Primary hand OA was diagnosed according to the clinical judgment of the treating rheumatologist. The LUMC serves both as a secondary and tertiary referral center for rheumatic diseases, enabling inclusion of patients with primary hand OA in all disease stages. Exclusion criteria included any pathological condition that could explain the patient’s symptoms (e.g., tendinitis, carpal tunnel syndrome, strain, fibromyalgia, arthritis due to other rheumatic diseases), secondary OA [including inflammatory joint diseases such as rheumatoid arthritis (RA), psoriatic arthritis, spondyloarthropathies, and current sarcoidosis; bone diseases such as osteitis deformans and osteochondritis, intraarticular fractures; metabolic diseases associated with joint diseases such as hemochromatosis, Wilson’s disease, and ochronosis; endocrine diseases such as acromegaly, major congenital or developmental diseases, bone dysplasias; and major local factors such as hypermobility and severe gout], and language barriers or psychological limitations that precluded giving informed consent or completing study visits. Written informed consent was obtained from all participants. The study was approved by the LUMC medical ethical committee (CCMO reference NL26201.058.08).
Patient characteristics and patient-reported outcomes
Demographic data and patient characteristics were collected using standardized questionnaires (Table 1). Education level was used as a proxy for socioeconomic status and divided into 3 groups: low (no education, primary school only, lower vocational education), middle (lower general secondary, secondary vocational education), and high (all higher education).
Baseline characteristics of a hand osteoarthritis (OA) population (n = 538) in secondary care — the HOSTAS cohort.
To study general disease burden, HRQOL was measured with the Dutch Research and Development (RAND) translation (version 1) of the Medical Outcomes Study Short Form-36 (SF-36)28. Because no norm values are available for the RAND-36 translation, we used the scoring algorithm and age- and sex-specific Dutch population-based norm scores from the Dutch SF-36 translation to apply norm-based scoring29. The 2 translations are different only in wording, and when using the right scoring algorithm, they are practically interchangeable. We calculated 2 summary component scores: physical health (PCS; further used to assess HRQOL) and mental health (MCS) and standardized scores: scale 0–100, mean 50, SD 10. Lower scores represent worse health. A minimal clinically important difference (MCID) of 2 was reported30. We compared mean differences to this value to evaluate clinical relevance.
To study the disease-specific burden, self-reported hand function (0–36) and hand pain (0–20) were assessed by the Australian/Canadian hand OA index (AUSCAN; Likert scale). Higher scores indicate worse health31. Clinical relevance was analyzed in 2 ways. First, mean differences were compared with a minimal clinically important improvement (MCII); MCII (95% CI) function 1.4 (0.1–2.2) and pain 1.6 (1.0–2.0) are on a scale 0–36 and 0–20, respectively32.
Second, we used age- and sex-specific cutoff values based on reference values of the 95th percentiles for ages 45, 50, 55, 60, and 65 years of the AUSCAN distribution in the general population33. This means that when a patient has a score above this 95th percentile value, 95% of the general population has a lower score. We considered it clinically relevant when a patient has a score that is in the highest 5% of the population. Only reference values for the ages 45, 50, 55, 60, and 65 were available. Therefore, we extrapolated the cutoff values to 5 age categories: < 47.5 years (corresponding to values for age 45), ≥ 47.5 to < 52.5 (age 50), ≥ 52.5 to < 57.5 (age 55), ≥ 57.5 to < 62.5 (age 60), and ≥ 62.5 (age 65), respectively.
Clinical assessment
Physical examination was performed by trained research nurses, assessing the distal interphalangeal (DIP), proximal interphalangeal (PIP), interphalangeal (IP), metacarpophalangeal (MCP), and first carpometacarpal joints of both hands (30 per patient) for tenderness upon palpation, bony and soft swelling, deformity, and limited range of motion (last 2 characteristics not in MCP). To study disease-specific burden, tender joints upon palpation were summated into tender joint count (TJC). Crepitus, bony tenderness, bony enlargement, and palpable warmth of the knee and internal rotation of the hip were also examined. Body mass index (BMI; kg/m2) was calculated using measured weight and height.
OA definition
The rheumatologist’s diagnosis of hand OA was used as an inclusion criterion in HOSTAS. Additionally, the number of patients fulfilling the American College of Rheumatology (ACR) criteria for hand OA was determined34. For patients not fulfilling these criteria, we ascertained whether they definitely had hand OA (radiographic and/or structural features). Knee or hip OA was assessed using the ACR criteria based on history and physical examination35,36. Also, joints with a prosthesis, arthroplasty, or arthrodesis with indication “OA, worn-out or pain” were regarded as having endstage OA. For the hands, endstage OA (i.e., arthrodesis/arthroplasty in a hand joint), meant that we considered the ACR criterion “hand pain, aching, or stiffness” fulfilled and considered the joint having bony swelling, limited range of motion, and deformity, but not soft swelling or tenderness.
Comorbidities
Seventeen of the 18 self-reported assessed comorbidities were assessed by a modified Dutch version of the Charlson index (total score range 0–33; Table 2)37. “Malignancy” was used instead of “any tumor, leukemia or lymphoma.” When “connective tissue disease” was reported, the medical chart was verified to ascertain rheumatic disease other than hand OA. Osteoporosis was the 18th self-reported comorbidity, but was not weighted in the Charlson score. Obesity (BMI ≥ 30 kg/m2) was determined using physical examination.
Prevalence of comorbidities and generalized osteoarthritis (OA) in a hand OA population (n = 538) in secondary care.
The total number of comorbidities was summed (0–19), i.e., self-reported comorbidities and obesity. Presence of any comorbidity was defined as having at least 1 of these 19 comorbidities. To study specific types of comorbidities, some comorbidities were grouped: myocardial infarction, cardiac failure, peripheral vascular disease, and cerebrovascular disease (stroke) into CV disease; ulcer disease, mild and severe liver disease into gastrointestinal disease; malignancy and metastatic disease into malignant disease; diabetes mellitus with and without end-organ damage into diabetic disease.
Because knee and/or hip OA could be considered phenotypes of OA (i.e., generalized OA), having knee/hip OA was not regarded as a comorbidity, but assessed separately.
In a subgroup (patients included after January 2011), the Hospital Anxiety and Depression Scale (HADS; range total scale 0–42) was assessed38,39. A total HADS score ≥ 16 was used to define depression-anxiety as a comorbidity22.
Radiographs
Joints of both hands (n = 30) were scored 0–4 on conventional dorsal-volar radiographs, according to the Kellgren-Lawrence (KL)40 grading scale. Osteophytes and joint space narrowing (JSN) were scored 0–3 (IP 0–1) following the Osteoarthritis Research Society International atlas (MCP scored as PIP)41. Erosive disease was defined as having ≥ 1 joint with an eroded or remodeled subchondral plate according to Verbruggen and Veys42. Radiographs were scored blinded for demographic and clinical data (WD). Intraobserver reliability, based on randomly selected radiographs (10%), was good; intraclass correlation coefficient was > 0.9 for different scores. Arthroplasty/arthrodesis was considered endstage radiographic OA (maximum score).
Statistical analysis
Patient characteristics were compared using Student t tests, chi-squared tests, or Mann-Whitney U tests when appropriate. Multivariable linear regression analysis was used to study cross-sectional associations between presence of any comorbidity, Charlson index score, and specific comorbidities (determinants) and HRQOL, self-reported hand function and pain, and TJC (outcomes). Data were presented as regression coefficients (95% CI), reflecting mean score differences when comparing 2 groups (e.g., presence/absence of comorbidity; Table 3). Thereafter, we evaluated clinical relevance by studying associations between presence of any comorbidity or specific comorbidities (determinant) and function or pain above the reference curve cutoff (outcome). For this we used a Poisson regression model with long link function and robust standard errors and presented results as risk ratios (RR) with 95% CI43. All analyses were adjusted for age and sex. Other variables were not known from theory to affect the association or did not act as a confounder in univariate analysis nor in stepwise regression and hence were not adjusted for. SPSS software for Windows, V.23.0 (IBM) was used.
Associations between specific types of comorbidities and physical health-related quality of life (HRQOL), self-reported hand function or hand pain and tender joint count in a hand osteoarthritis (OA) population in secondary care.
RESULTS
Study population
According to the clinical hand OA diagnosis, 629 patients were eligible for inclusion, of whom 80 did not consent to participate and 11 fulfilled exclusion criteria after medical chart verification. The remaining 538 patients were included (Figure 1, Table 1). Data were complete for age, sex, and physical examination. Less than 3% of data was missing for other variables, except SF-36 (5%), symptom duration (7%), and nutraceutical use (4%). Patients with complete data for all variables in Table 1 did not differ from the total population (not shown).

Flowchart for the HOSTAS study showing inclusion and completeness of data. HOSTAS: Hand OSTeoArthritis in Secondary care; OA: osteoarthritis.
Of the patients in our cohort, 90% (463/526, 12 patients missing data) fulfilled the ACR criteria for hand OA. They had a mean age of 61 years and the majority were women (463/538, 86%). One-fourth had a low education level (141/524, 27%). Two-thirds used medication for joint pain (351/538, 67%; predominantly acetaminophen).
Physical HRQOL was lower in our population than in the general population (p < 0.001), whereas mental HRQOL was similar. No sex differences were observed in PCS or MCS (not shown). The mean observed disease-specific burden as measured with AUSCAN was 15.6 for function and 9.3 for pain (Table 1). Women reported worse function and more pain than men (not shown).
Many joints had bony swellings (median 11), while few joints had soft swelling (median 0; Table 1). Mean (SD) TJC was 4.8 (5.2).
Ninety-nine percent of patients had at least 1 joint with KL score above zero, 97% had at least 1 joint with osteophytes, and 90% at least 1 joint with JSN, while almost 30% showed radiographic erosive disease. Seven hand joints in 6 patients had arthroplasty or arthrodesis at baseline.
Table 2 depicts prevalence of comorbidities. Patients with complete data (n = 511) did not differ from the total population (not shown). Any comorbidity (i.e., self-reported and obesity) was present in 54% (287/531) of patients, while 43% (222/519) had self-reported comorbidity. Thirty-one percent (161/526) of patients had knee and/or hip OA. As shown in Table 3, obesity was the most prevalent comorbidity, followed by CV and pulmonary disease.
Association of comorbidity with disease burden
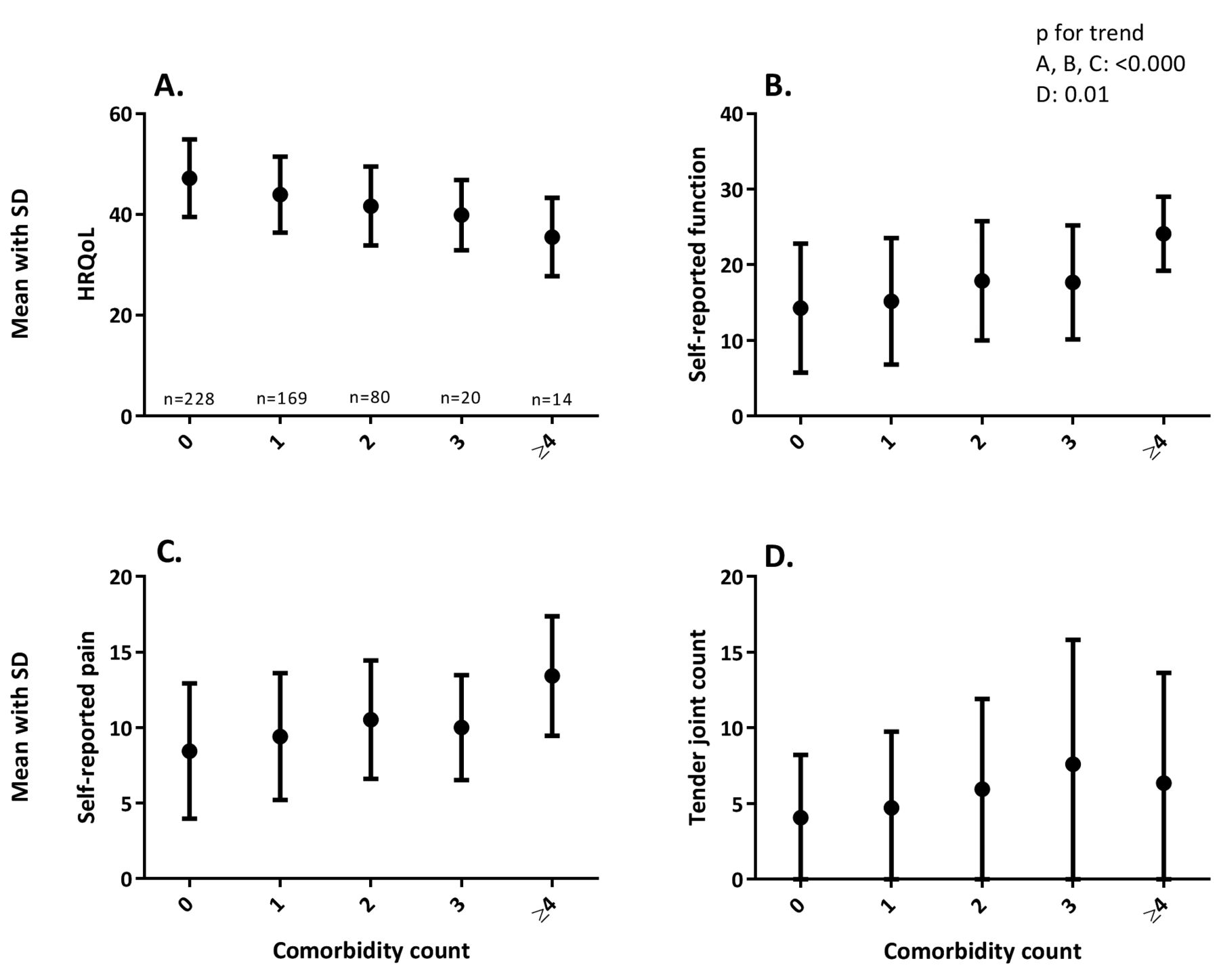
Presence of any comorbidity was associated with higher disease burden than when comorbidity was absent; adjusted mean score difference (95% CI) for HRQOL −4.4 (−5.8 to −3.0; MCID 2), hand function 1.9 (0.4–3.3; MCII 1.4), hand pain 1.4 (0.6–2.1; MCII 1.6), and hand TJC 1.3 (0.4–2.2). The number of comorbidities was associated with lower HRQOL and more hand complaints (Figure 2). Also, Charlson index score was associated; adjusted β (95% CI) for HRQOL −1.4 (−2.0 to −0.8), function 1.1 (0.5–1.7), pain 0.7 (0.4–1.0), and TJC 0.6 (0.2–0.9).

Mean scores with (SD) of (A) health-related quality of life (HRQOL; range 0–100, mean 50), as assessed by Medical Outcomes Study Short Form-36 physical component scale and normalized to the Dutch population; (B) self-reported hand function (0–36) and (C) self-reported hand pain (0–20), both assessed by the Australian/Canadian hand osteoarthritis Index; and (D) tender joint count (0–30) assessed by physical examination of patients with 0, 1, 2, 3, or ≥ 4 comorbidities. For HRQOL, a lower score means worse health. For the other outcomes, a higher score means worse health. Only patients with complete data on all comorbidities are depicted (n = 511).
In Table 3 we show associations between specific types of comorbidities and disease burden, presented as mean differences between groups of presence/absence of the comorbidity. Self-reported connective tissue disease, but also pulmonary disease and CV disease, were associated with both general and hand-specific disease burden. Obesity was only associated with HRQOL, while osteoporosis was only associated with self-reported function. Diabetes, malignant disease, and gastrointestinal disease were not associated with HRQOL or hand complaints.
Knee/hip OA was associated with both general and disease-specific burden [adjusted mean difference (95% CI)]: HRQOL −3.7 (−5.2 to −2.1), function 1.8 (0.2 to 3.4), pain 0.8 (−0.03 to 1.6), and TJC 1.7 (0.8 to 2.6).
Additional analyses in 381 patients with HADS data (same characteristics as total population) showed that depression-anxiety (n = 50, 13%) was associated with higher disease-specific burden; adjusted mean difference (95% CI) for HRQOL −2.2 (−4.7 to 0.2), function 4.4 (2.1–6.8), pain 2.2 (1.0–3.5), and TJC 2.5 (1.1–4.0). In this subgroup, the presence of any comorbidity (60% of patients when including depression-anxiety) and number of comorbidities were associated with high disease burden (data not shown).
Clinical relevance
The mean score difference in HRQOL and hand function in the presence of any comorbidity was higher than the MCII/MCID, but this was not found for self-reported hand pain. For the specific types of comorbidities, most mean differences in Table 3 that were statistically significant (bold) were also higher than the MCII/MCID, except for self-reported pain in patients with pulmonary and CV disease.
Poisson regression confirmed the clinically relevant role of presence and number of comorbidities: adjusted RR (95% CI) for hand function or pain above the age- and sex-specific cutoff for presence of any comorbidity was 1.2 (1.01–1.5) and 1.2 (1.02–1.5), and per additional comorbidity 1.2 (1.1–1.2) and 1.2 (1.1–1.2), respectively. For example, this means that patients with any comorbidity present have a 20% greater chance to have an AUSCAN function score in the highest 5% of their age and sex category than patients without any comorbidity. For the specific types of comorbidities, all mean differences in Table 3 that were statistically significant (bold) were associated in this analysis, except for the association between pulmonary disease and pain. For example, RR (95% CI) for function or pain above the cutoff for presence of connective tissue disease were 1.6 (1.2–2.0) and 1.6 (1.3–2.0), respectively; other data not shown.
DISCUSSION
In our large cohort of patients with primary hand OA from a rheumatology outpatient clinic, we studied the relationship between comorbidities and general and hand-specific disease burden and evaluated its relevance. We showed that comorbidity was associated with higher disease burden, both for musculoskeletal comorbidities such as connective tissue disease, as well as for nonmusculoskeletal comorbidities including pulmonary or CV disease and depression-anxiety. When compared to an MCII/MCID and to population-based reference values, we observed that the difference was higher. To our knowledge, this is the first report that describes such relations in a quantitative way.
Comorbidities were prevalent in our study: more than half had any comorbidity, while 40% had a comorbidity included in the Charlson index. Patients with knee OA in the Osteoarthritis Initiative, which also used this index, reported fewer comorbidities (28%). However, their study included fewer women and another OA type, which could explain the difference18.
The number of comorbidities was associated with higher disease burden. Contrary to our findings, a study in patients with thumb base (osteo)arthritis reported no association between number of comorbidities and worse function24. However, it is unclear whether that study used a validated comorbidity index and a different subset of hand OA was studied. In another cohort, presence of 3 or more comorbidities did not affect the association between hand OA and hand disability12. However, participants in this population-based study were older than in our study. Moreover, this study did not focus on hand OA patients and could, therefore, not be generalized to hand OA patients in primary or secondary care.
Our hand OA study is one of the first to report prevalence of separate comorbid conditions. We found that nonmusculoskeletal comorbidities such as pulmonary and CV disease were associated with disease burden. This is in accordance with studies in patients with several OA types that also report a role for nonmusculoskeletal comorbidities, such as diabetes, chronic pulmonary disease, and cardiac disease17,20,21. Because numerous papers in literature report on the unfavorable effect of multimorbidity on quality of life8,10,44, it seems difficult to attribute disease burden to 1 condition. To study the separate roles of concurrent conditions, one can analyze interaction in a population-based study, as was done for knee OA and obesity45 and for hand OA and several diseases12.
A strength of our study is the large number of well-described patients, including primary hand OA in different disease stages and subsets. This is illustrated in our data; this cohort includes patients with zero tender joints or without radiographic hand OA but also with 29/30 tender joints or erosive disease. Nevertheless, this population is patients with primary hand OA recruited from our rheumatology outpatient clinic in a secondary and tertiary referral center. Therefore, it should be acknowledged that this population could be different from a primary care population and that results should be extrapolated with caution. Another strength of our study is that we compared the values to the MCII/MCID and to age- and sex-specific reference values. Because age and sex are modifiers of clinical outcomes in hand OA, this adds to the validity of our results.
Not only from a clinical but also from a methodological perspective, comorbidity is of importance. Comorbidity could be a contextual factor, i.e., a factor that might influence (interpretation of) results, and was identified that way by the Outcome Measures in Rheumatology hand OA working group26,27. Our results confirm that comorbidity is a contextual factor to consider when interpreting core outcomes such as HRQOL, hand function, and hand pain, especially when the effect size of the studied intervention is small. If any recommendations could be given based on our study, perhaps the most important is to consider adjustment for the number of comorbidities or for presence of any comorbidity. Depending on the research question, adjustment for specific types of comorbidities could also be considered.
There are some limitations we need to address. First, because of our cross-sectional design, we were unable to draw any conclusions about the effect of comorbidity, or its treatment, on hand OA disease burden over time. Several papers indicate that multimorbidity could be related to under-treatment of hand OA, especially when seemingly unrelated conditions are present46,47. Therefore, we expect that adequate management of all morbidity of a patient would reduce disease burden over time. Future research could build upon our current study, e.g., by studying exercise and/or medication use to reduce comorbidity. Second, we only assessed psychiatric diseases in a subgroup and defined depression-anxiety by HADS score, which is not a diagnostic tool. However, HADS has shown to be a valid instrument to detect mood disorders in patients with OA22. Third, most comorbidities were self-reported. However, diagnostic accuracy of self-reported disease seems acceptable48, the Charlson is a validated index49, and prevalence of comorbidity in our population was mostly similar to another small hand OA population50. Therefore, we think the self-report is sufficiently reliable to reflect comorbidity burden in our population. Fourth, we assessed the MCID for HRQOL with a value derived from a study in lower extremity OA30. However, because no hand OA studies were available, we found this the best option.
In our large primary hand OA cohort, presence and number of comorbidities as well as separate comorbid conditions showed an association with both general and disease-specific burden that is larger than the MCID/MCII. We conclude that comorbidities have a role in the assessment of hand OA outcomes and may be considered as contextual factors as well as in clinical practice. To optimize disease management, a holistic view, taking all concurrent conditions of a patient into account, seems relevant. Future studies can analyze the longitudinal relationship between comorbidities and hand OA disease burden and can assess the effect of interventions.
Acknowledgment
We thank the patients of the HOSTAS cohort for participation in this study and research nurses B. van Schie-Geyer, A. Wongsodihardjo, and M. Janson, and data managers J. van Krol-Berkel and C. Kromme in the Rheumatology Department of the LUMC, and technicians in the Radiology Department of the LUMC for support in data collection.
Footnotes
Funding from the Dutch Arthritis Foundation (Reumafonds): LLP-24 for the HOSTAS cohort and appointment of the first author.
- Accepted for publication July 6, 2017.








{kind=link}
{kind=link}