

Abstract
Objective. The aim of our study was to determine whether an automated capture and analysis system could detect differences in structure and function of sublingual microvessels in patients with systemic sclerosis (SSc) compared to healthy controls.
Methods. Intravital microscopy of the sublingual microcirculation was automatically captured and analyzed in 40 patients with SSc and 10 age-matched healthy controls.
Results. Total and perfused microvascular density were lower in patients with SSc compared with controls (total microvascular density: 2471 ± 134 µm/mm2 vs 3067 ± 197 µm/mm2, p = 0.020; perfused microvascular density: 1708 ± 92 µm/mm2 vs 2192 ± 144 µm/mm2, p = 0.009). However, the relative percentage of perfused to total microvascular density was similar between SSc and controls (72 ± 2% vs 71 ± 2%, respectively, p = 0.429). Mean red blood cell (RBC) fraction, which indicates the longitudinal tube hematocrit of microvessel segments, was lower in patients with SSc compared with controls (69 ± 1% vs 77 ± 1%, respectively, p < 0.001). Perfused boundary region (PBR), a marker of endothelial glycocalyx barrier properties, was higher in patients with SSc compared with controls (2.1 ± 0.0 µm vs 1.9 ± 0.0 µm, respectively, p = 0.012), suggestive of a dysfunctional glycocalyx. There was an inverse association of PBR with perfused microvascular density (r = −0.40, p = 0.004) and RBC fraction (r = −0.80, p < 0.001).
Conclusion. Our results indicate that automated capture and analysis of sublingual microvessel segments produces detailed, objective microvascular structural and functional data that have allowed us to distinguish patients with SSc from controls. These data suggest that microvascular structural and functional abnormalities present in patients with SSc could be at least partly due to a dysfunctional glycocalyx.
Systemic sclerosis (SSc, scleroderma) is a rare multiorgan, autoimmune disease characterized by activation of immune cells, production of autoantibodies1, and progressive fibrosis2. Although there is considerable heterogeneity in the extent of organ involvement between patients with SSc, microvascular abnormalities appear in most patients2,3. Currently, nailfold videocapillaroscopy (NVC) is used to characterize microvessel structural abnormalities (i.e., capillary size and density, and presence of microhemorrhage), and is useful in SSc diagnosis4. NVC is noninvasive and time-efficient, but it has limited ability to measure the functional properties of the microvasculature. Because functional disturbance likely precedes changes in the structure of microvessels5, microvascular function may be a better target and a time-sensitive means of assessing pathophysiological SSc microvascular changes. Therefore, a clinical tool that assesses the changes in microvascular function may have clinical value in the management of patients with SSc. Measurements of microvascular function could also be useful to assess the efficacy of therapeutic interventions. Accordingly, a noninvasive and time-efficient method to assess microvascular function in patients with SSc is needed.
Currently, intravital videomicroscopy can be used to noninvasively assess the function of the sublingual microvasculature, but it is largely dependent on manual analysis6. This method is labor intensive, yields limited data from a small number of microvessels, and introduces the risk of investigator bias. A validated automated capture and analysis system overcomes these limitations, allowing for a quick and reliable analysis of thousands of microvessel segments7. Markers of microvascular health assessed by this system include markers of perfusion, such as the number and longitudinal fraction of microvessel segments that are filled with red blood cells (RBC). This automated system also performs an indirect measurement of the barrier function of the endothelial glycocalyx. The endothelial glycocalyx is a gel-like structure that projects from the endothelial cell wall toward the vessel lumen, protecting the vessel and playing a role in mechano-transduction of shear stress. The automated system measures glycocalyx barrier function by examining the lateral movement of RBC as they flow through microvessel segments, indicating their encroachment into the glycocalyx. Thus, greater encroachment of RBC into the glycocalyx is indicative of a thin or diminished glycocalyx, which in turn may contribute to endothelial dysfunction8,9.
Automated capture and analysis of videomicroscopy recordings has identified microvascular dysfunction in patients with cardiovascular disease10, endstage renal disease11, sepsis12, and diabetes13. Because microvascular abnormalities are a prominent feature of SSc, we sought to investigate the potential of an automated capture and analysis system to detect microvascular dysfunction in patients with SSc. Specifically, we wanted to determine whether differences in markers of microvascular perfusion, as well as glycocalyx barrier function, could be detected between patients with SSc and healthy age-matched controls using the automated capture and analysis of sublingual microvessel segments. This automated system allows for assessment of microvascular function at each individual microvessel segment lumen diameter, therefore we also sought to determine whether the postulated microvascular dysfunction in SSc was present across all microvessel segment lumen diameters.
MATERIALS AND METHODS
Subjects
Forty patients with SSc were recruited from the University of Utah SSc Clinic. Patients were previously diagnosed with SSc by the 2013 classification criteria14. Ten age- and sex-matched healthy controls were recruited from the general population. All procedures were approved by the Institutional Review Board of the University of Utah and Salt Lake City Veterans Affairs Medical Center (VAMC; IRB# 00077934), which serves as the ethics committee, and were performed at the University of Utah SSc Clinic or Salt Lake City VAMC from May 2015 to September 2016. Written informed consent was obtained prior to participation after a detailed explanation of the study.
Subject characteristics
Body mass index was measured. The following clinical features of patients with SSc were recorded: disease duration, modified Rodnan skin score (mRSS), history of vascular complications, antinuclear antibody, SSc-specific antibody status, and cardiovascular-acting medications.
Automated capture and analysis of the sublingual microcirculation
Intravital microscopy was performed with a handheld videocapillary CapiScope microscope (KK Technology) to view the sublingual microcirculation (Figure 1A). The intravital microscope has a sidestream dark field camera that uses green light-emitting diodes. The green light is primarily absorbed by hemoglobin in RBC in the microcirculation that allows RBC to be viewed in contrast to the background. Video of the sublingual microcirculation was recorded and analyzed using an automated capture and analysis system (GlycoCheck, MicroVascular Health Solutions LLC). Each trial lasts 2–3 min and consists of several ∼2-s video recordings that are 40 frames in length. In each recording, sublingual microvessels with a 5–25 µm lumen diameter are identified by differences in contrast between RBC and the background, and are subsequently divided into 10-µm microvessel segments. Video recordings are repeated until at least 3000 microvessel segments have been acquired, concluding the trial. Thereafter, the automated analysis system determines functional outcomes in perfused microvessel segments, defined as any segment with sufficient contrast that contains RBC in ≥ 50% of its length in the first frame of a 40-frame video recording session. Microvessel segments with insufficient contrast and RBC in < 50% of its length do not qualify as perfused and are identified as lowly perfused microvessel segments. At least 2 trials were performed for each subject with the entire data collection lasting 5 min or less. This system has been well validated, shown to be reliable in adults, and used to identify differences in the microvasculature between healthy cohorts and a range of clinical populations10,12,13,15,16.

Determination of sublingual microvascular health markers. Sidestream dark field (SDF) imagery is used to capture images of the sublingual microvasculature (A). In each recording, the GlycoCheck automated analysis software divides microvessels into 10 μm perfused (green) or lowly perfused (yellow) microvessel segments (B). To determine red blood cell (RBC) fraction, the automated system places 10 marker lines spaced 0.5 μm apart on each side of the perfused microvessel segment marker line (21 marker lines total). RBC fraction is calculated as the percentage of marker lines that are crossed by RBC (C). To determine perfused boundary region, the automated system identifies the median RBC column width and total perfused diameter in each perfused microvessel segment. Perfused boundary region is calculated as total perfused diameter − median RBC column width/2 (D). Using a separate manual method, we estimated glycocalyx thickness in sublingual recordings by calculating the difference in RBC perfused diameter before and immediately after the passage of a spontaneous leukocyte and subsequently dividing by 2 (E).
Total microvascular density
Total microvascular density represents the sum of perfused and lowly perfused microvessel segments. Total microvascular density is calculated using the following equation7:

Total microvessel segments are multiplied by 10 because each segment is 10 µm in length. Total microvascular density is reported as a sum across microvessel segments with a 5–25 µm lumen diameter.
Perfused microvascular density
The automated analysis algorithm identifies a perfused microvessel segment as one that contains RBC in at least 50% of its length in the first frame of a 40-frame video recording (Figure 1B). From this, perfused microvascular density is calculated using the following equation7:

Perfused microvascular density represents the cumulative length of perfused microvessel segments relative to a given area of tissue. Perfused microvascular density is reported as a sum across microvessel segments with a 5–25 µm lumen diameter at each microvessel segment lumen diameter, and by size group of small (5–9 µm), medium (10–19 µm), and large (20–25 µm) lumen diameter microvessel segments. Additionally, the percentage of perfused microvessel segments relative to total microvessel segments was determined in each subject.
RBC fraction
RBC fraction represents an estimate of the longitudinal tube hematocrit of perfused microvessel segments (Figure 1C). To determine RBC fraction, the automated system places 10 marker lines spaced 0.5 µm apart on each side of the perfused microvessel segment marker line (21 marker lines total). RBC fraction is calculated as the percentage of marker lines crossed by RBC in each perfused microvessel segment. This is repeated in the same microvessel segment in all 40 frames of a video recording and then averaged. RBC fraction is reported as an average across microvessel segments with a 5–25 µm lumen diameter, at each microvessel segment lumen diameter, and by size group of small (5–9 µm), medium (10–19 µm), and large (20–25 µm) lumen diameter microvessel segments.
Perfused boundary region
Perfused boundary region (PBR) represents the depth of penetration of RBC into endothelial glycocalyx and is taken as a marker of glycocalyx function (Figure 1D), with a larger PBR indicating greater perturbation of the glycocalyx. The automated analysis algorithm identifies the median RBC column width and total perfused diameter in each perfused microvessel segment. PBR is calculated from those variables using the following equation7:

Perfused boundary region is reported as an average across microvessel segments with a 5–25 µm lumen diameter, at each microvessel segment lumen diameter, and by size group of small (5–9 µm), medium (10–19 µm), and large (20–25 µm) lumen diameter microvessel segments.
Glycocalyx thickness
Using a different method from the GlycoCheck system, we derived an estimate of glycocalyx thickness by manually measuring the change in width of flowing RBC before and after the passage of a spontaneous leukocyte in individual capillaries (Figure 1E), as described and validated previously17,18. Similar to RBC, leukocytes cannot freely penetrate the glycocalyx; however, because leukocytes are larger than RBC, as they flow through microvessels the glycocalyx is compressed, increasing the width of flowing RBC. Glycocalyx thickness was calculated using the following equation18:

Statistical analysis
Intersession coefficient of variation (CV) was determined in controls on 2 nonconsecutive days. Statistics were performed using SPSS software version 22 (IBM). Unpaired t tests were used to compare differences in subject characteristics between SSc and controls. A 2-way repeated-measures ANOVA was used to evaluate differences across microvessel segment lumen diameters between SSc and controls, and a least significant difference unpaired t test identified values that were significantly different. Bivariate correlational analysis was performed between selected variables. Statistical significance was set at p < 0.05 for all analyses. Data are presented as mean ± SEM, unless indicated otherwise.
RESULTS
Subject characteristics
Characteristics of patients with SSc and controls are presented in Table 1. There were no differences in age or body stature between groups. One-third of the patients with SSc had evidence of severe vasculopathy, including pulmonary arterial hypertension, scleroderma renal crisis, or digital ulceration.
Subject characteristics.
Total microvascular density
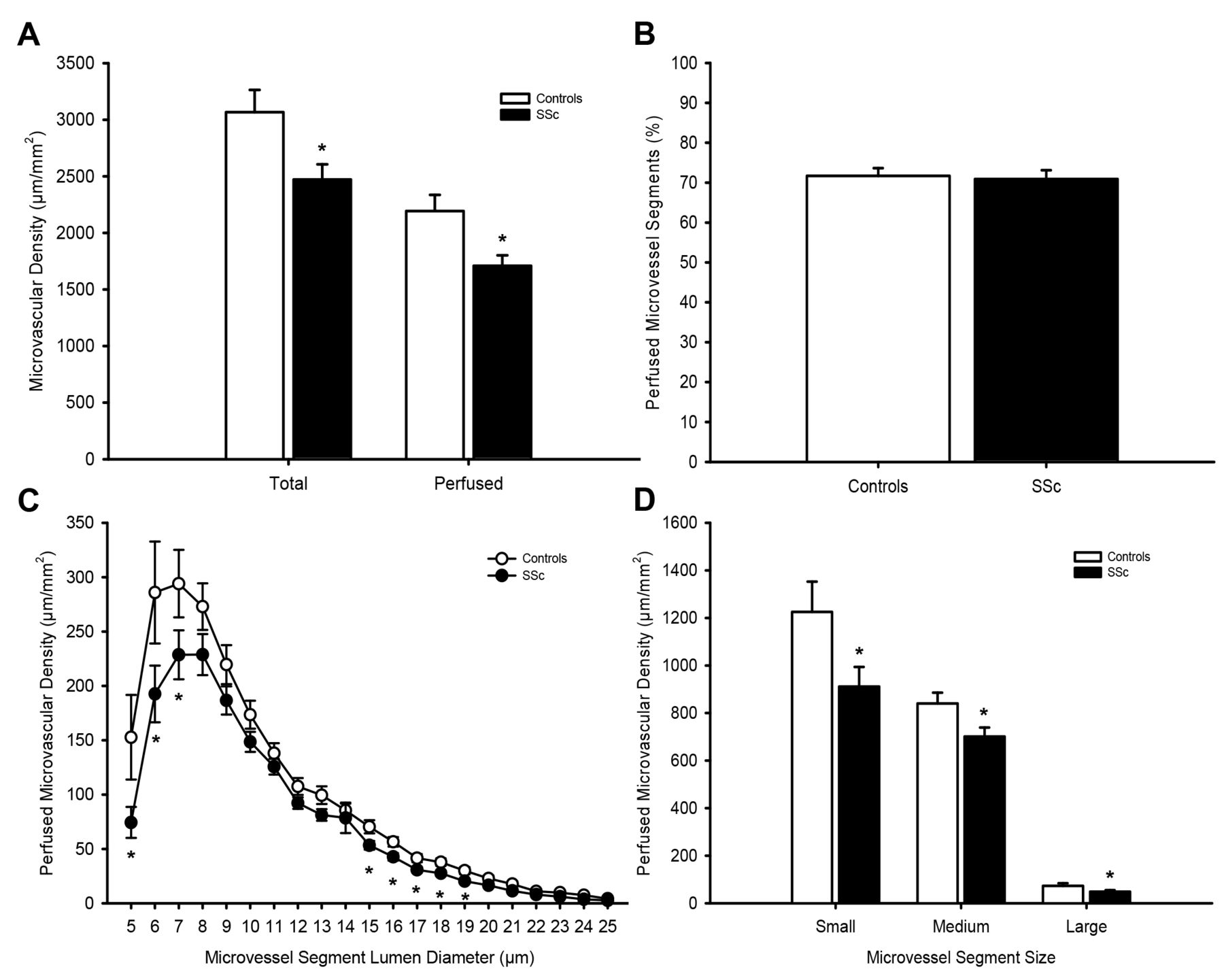
Total microvascular density was lower in patients with SSc compared with controls (Figure 2A; p = 0.020). Intersession CV for total microvessel density was 7.9 ± 1.6%.
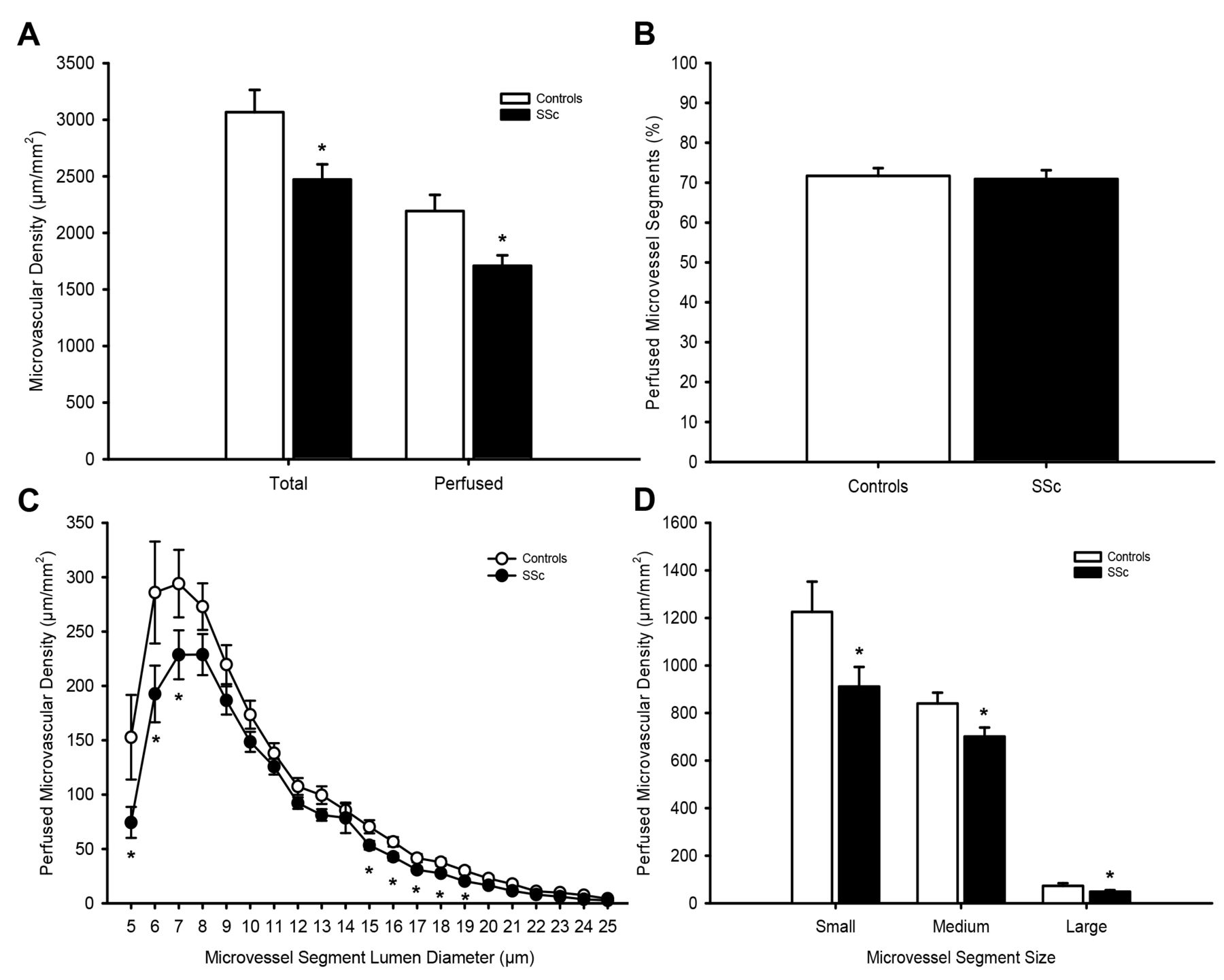
Microvascular density. Total and perfused microvascular density in microvessel segments of the sublingual mucosa (A) and percentage of total microvessel segments that were perfused (B) in healthy controls (white) and patients with systemic sclerosis (SSc; black). Detailed analysis of perfused microvascular density in microvessel segments (C) and grouped by small (5–9 μm), medium (10–19 μm), and large (20–25 μm) microvessel segment lumen diameter (D) in controls and SSc. *p < 0.05, significant difference between controls and SSc.
Perfused microvascular density
Perfused microvascular density was lower in patients with SSc compared with controls (Figure 2A; p = 0.009). There was no difference in percentage of perfused microvessel segments between patients with SSc and controls (Figure 2B; p = 0.429).
Analysis by microvessel segment lumen diameter revealed that differences in perfused microvascular density between SSc and controls were present in microvessel segments with a small, medium, and large lumen diameter (Figure 2C and 2D; p = 0.043–0.044). Intersession CV for perfused microvascular density was 6.4 ± 2.5%.
RBC fraction
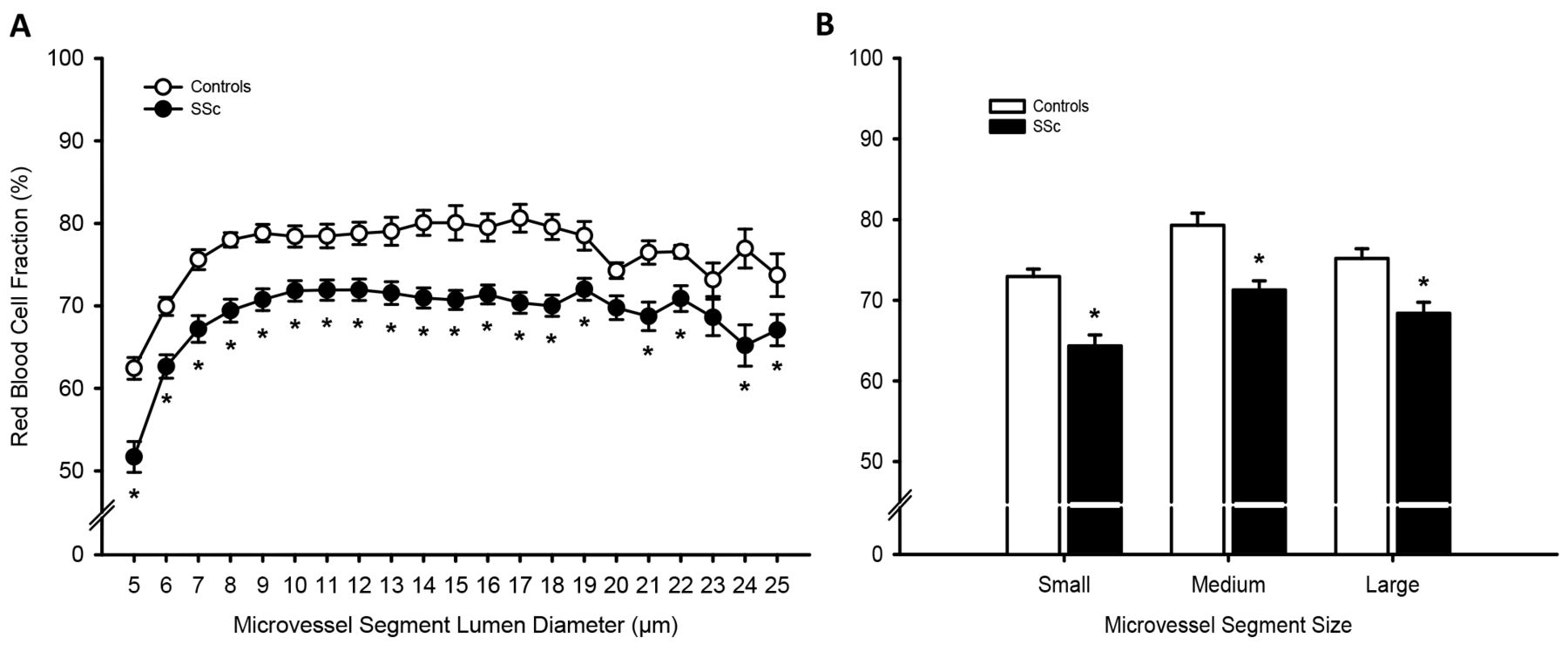
Mean RBC fraction across all microvessel segments was significantly lower in patients with SSc compared with controls (69 ± 1% vs 77 ± 1%, respectively, p < 0.001). Analysis by microvessel segment lumen diameter revealed that differences in RBC fraction between SSc and controls were present in all microvessel segments sizes (Figure 3A and 3B; p = 0.001–0.010). Intersession CV for mean RBC fraction was 1.4 ± 0.3%.

Red blood cell (RBC) fraction. RBC fraction in microvessel segments of the sublingual mucosa (A) and grouped by small (5–9 μm), medium (10–19 μm), and large (20–25 μm) microvessel segment lumen diameter (B) in healthy controls (white) and patients with systemic sclerosis (SSc; black). *p < 0.05, significant difference between controls and SSc.
PBR measures
Mean PBR across all microvessel segments was significantly higher in patients with SSc compared with controls (2.1 ± 0.0 µm vs 1.9 ± 0.0 µm, respectively, p = 0.012). Analysis by microvessel segment lumen diameter revealed that differences in PBR between SSc and controls were present only in microvessel segments with a medium to large lumen diameter (Figure 4A and 4B; p = 0.003–0.044). Intersession CV for mean PBR was 2.3 ± 0.9%.
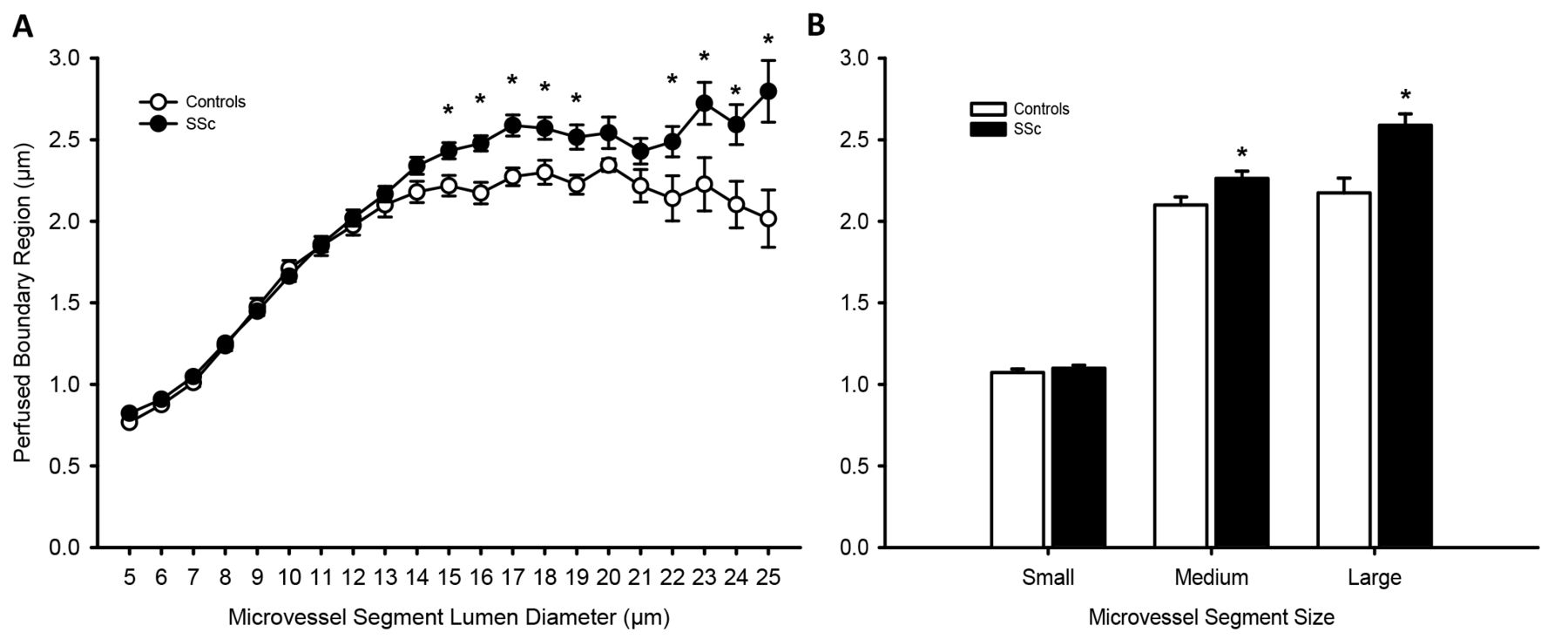
Perfused boundary region (PBR). PBR in microvessel segments of the sublingual mucosa (A) and grouped by small (5–9 μm), medium (10–19 μm), and large (20–25 μm) microvessel segment lumen diameter (B) in healthy controls (white) and patients with systemic sclerosis (SSc; black). *p < 0.05, significant difference between controls and SSc.
Glycocalyx thickness and its relation to glycocalyx barrier function
Glycocalyx thickness was significantly lower in patients with SSc compared with controls (Figure 5A; p < 0.001). Additionally, PBR was significantly, inversely associated with glycocalyx thickness (Figure 5B; r = −0.41, p = 0.003).
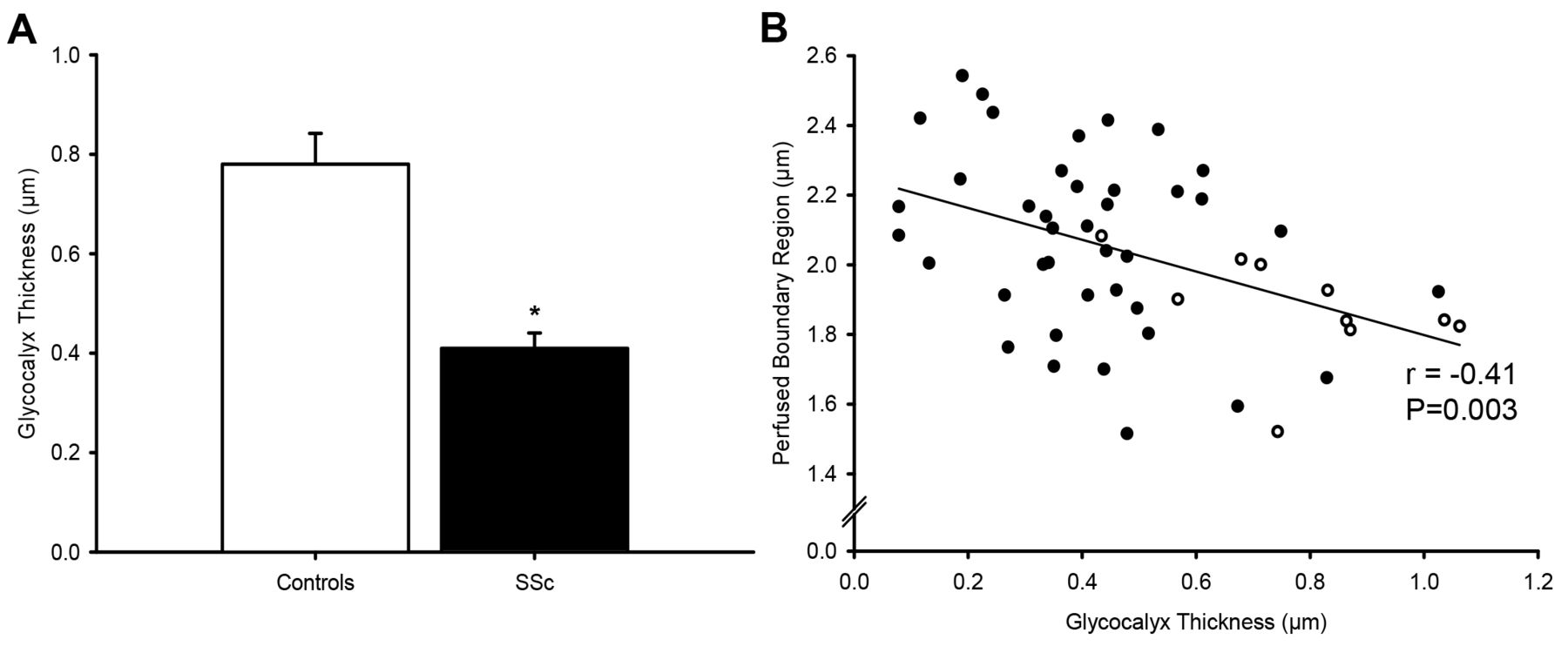
Glycocalyx thickness. Glycocalyx thickness (A) is significantly higher in healthy controls (white) compared with patients with systemic sclerosis (SSc; black). Perfused boundary region is significantly inversely associated with glycocalyx thickness (B) in the combined cohort of healthy controls (white circles) and patients with systemic sclerosis (SSc; black circles). *p < 0.05, significant difference between controls and SSc.
Association of glycocalyx barrier function with markers of microcirculatory perfusion
PBR was significantly inversely associated with perfused microvascular density (r = −0.40, p = 0.004) and to a greater degree, RBC fraction (r = −0.80, p < 0.001).
DISCUSSION
Use of an automated system to capture and analyze sublingual microvessel segments produced detailed and objective microvascular data that detected a number of differences in microvascular structure and function between patients with SSc and controls. The main findings are that compared with controls, sublingual microvessel segments in patients with SSc exhibited (1) a lower total and perfused microvascular density; (2) a lower RBC fraction; (3) a higher PBR, suggestive of a dysfunctional glycocalyx; and (4) an inverse relationship of PBR to glycocalyx thickness and markers of sublingual microcirculatory perfusion. Further analysis of microvessel segments by lumen diameter revealed that perfused microvascular density and RBC fraction was lower in small, medium, and large diameter microvessel segments, while PBR was higher only in microvessel segments with medium and large lumen diameters. These findings support the notion that microvascular abnormalities are present in patients with SSc, but indicate that microvascular abnormalities may not be uniform across all microvessel segment lumen diameters in the sublingual mucosa of patients with SSc.
Microvascular perfusion abnormalities in SSc
We found that the perfused microvascular density and RBC fraction were lower in patients with SSc compared with controls. Although perfused microvascular density was different between controls and SSc, the magnitude of difference tended to become greater as microvessel segment lumen diameter decreased. This finding is important because oxygen exchange takes place in the smallest microvessels (i.e., capillaries), which might explain why dysfunction in the smallest microvessels has the greatest association with adverse health outcomes19,20. In contrast, the magnitude of difference in RBC fraction between controls and SSc was similar across all microvessel segment lumen diameters. Nevertheless, lower perfused microvascular density and RBC fraction likely indicate an impairment in microvascular tissue perfusion. Additionally, the finding that differences in perfused microvascular density between SSc and controls tend to become greater with decreasing microvessel segment lumen diameter suggests that abnormalities in the tissue area of perfusion become more pronounced as microvessel size decreases.
We also found that total microvascular density was lower in patients with SSc, suggesting that there is a lower number of microvessel segments available per given area of tissue. However, the percentage of total microvessel segments that were perfused was similar between patients with SSc and controls, suggesting that despite total and perfused microvascular density being lower in SSc, the ratio of total to perfused microvessel segments in patients with SSc is normal. Because of the cross-sectional design of our current study, we cannot determine whether lower total and perfused microvascular density in SSc is due to microvascular remodeling. However, it is possible that abnormal vasodilator and vasoconstrictor function is related to lower total and perfused microvascular density in patients with SSc.
Glycocalyx barrier function in SSc
In our present study, we have found a higher PBR in patients with SSc compared with controls, suggestive of impaired endothelial glycocalyx barrier function. Although a previous study has reported lower glycocalyx thickness in SSc6, to our knowledge we are the first to identify impaired glycocalyx barrier function in the sublingual microvasculature of patients with SSc using automated, objective measurement of a large number of microvessel segments. A functioning glycocalyx is important for vascular health because it promotes endothelium-dependent dilation by mechano-transducing shear stress8,9 and because it is a functional barrier between the blood and the cell wall21. Indeed, glycocalyx degradation is accompanied by impaired endothelium-dependent dilation22 and abnormal glycocalyx dimensions or function has been reported in cardiovascular disease10, endstage renal disease11, sepsis12, diabetes10,13,23, obesity24, and hypercholesterolemia25.
We also performed a manual analysis of glycocalyx thickness independently of the GlycoCheck system by measuring the change in the width of flowing RBC after the passage of a leukocyte18. We found that glycocalyx thickness was lower in patients with SSc compared with controls, confirming previous findings6. There was a modest inverse relationship between PBR and glycocalyx thickness, most likely because both measurements, although fundamentally different, are indicative of glycocalyx health. Importantly, this finding provides support for the automated capture and analysis software used in our study to determine some aspect of glycocalyx integrity.
A dysfunctional microvascular environment is now known to be one of the earliest changes in the pathogenesis of vascular-related diseases26, and findings indicate that modification to and dysfunction of the endothelial cell glycocalyx play major roles24. We have previously reported endothelial dysfunction in SSc, indicated by impaired reactive hyperemia and endothelium-dependent dilation27. Although we did not measure these markers of endothelial dysfunction in our present study, it is likely that a dysfunctional glycocalyx and endothelium coexist in patients with SSc. Further research is needed to determine the pathological role that a dysfunctional glycocalyx plays in the progression of endothelial dysfunction (or vice versa) in SSc and other states that are accompanied by endothelial dysfunction.
Effect of glycocalyx barrier function on markers of microvascular perfusion
We report an inverse relationship between PBR and RBC fraction and perfused microvascular density in the combined cohort, as well as in patients with SSc as a separate group. To our knowledge, we are the first to confirm these associations in patients with SSc, although this concept has been shown previously in a large cohort of healthy adults12. A major role of the glycocalyx is to form a barrier to flowing blood8,9 because an intact glycocalyx prevents RBC from penetrating into its domain28. A less penetrable glycocalyx requires conformational changes in RBC, such as RBC elongation, to pass through small microvessels. RBC elongation increases the likelihood that RBC are present in microvessel segments, increasing perfused microvascular density and RBC fraction. This is one potential explanation for the strong inverse relationship between PBR and markers of microvascular perfusion.
We also observed an inverse relationship between PBR and total microvascular density. Unlike our markers of perfusion, total microvascular density is a structural measurement of the number of microvessel segments per tissue area and is not dependent on the presence of a minimum number of RBC. Therefore, an inverse relationship between PBR and total microvascular density suggests that glycocalyx function may affect the number of microvessels in a given area. Changes in vascular function likely precede changes in structure5, therefore it is possible that glycocalyx dysfunction impairs microvascular perfusion, which could lead to a reduction in the number of total microvessel segments in a tissue area.
Clinical implications
In our study, we used a new instrument to detect sublingual microvascular abnormalities in patients with SSc that requires minimal time and training and provides automated capture and analysis, eliminating investigator bias. There is currently sparse evidence for effective therapeutics for the treatment of SSc; however, microvascular damage and dysfunction are present in nearly all cases29. Therefore, the automated capture and analysis of the sublingual microcirculation used in our present study could have clinical utility in assessment of therapeutic interventions in SSc. However, this technique has limitations. The automated capture and analysis system identifies microvessels by differences in contrast between RBC and background. When no RBC are present in a microvessel, it would not be identified as a microvessel. Although capillary rarefaction occurs in the skin30 and nailbeds31,32 of patients with SSc, it is possible that lower total microvascular density in these patients may be due to the inability of the automated analysis system to identify empty microvessels. An additional limitation of our present study is the disparity in sample size between patients with SSc and healthy controls. Patients with SSc have a high degree of variability in the extent of vasculopathy. Therefore, a higher number of patients were included in our study to provide greater assurance that both groups were representative of their populations. Despite this we did not have the statistical power to investigate the effect of sublingual frenulum abnormalities33 and other clinical features of SSc such as disease duration, vascular and gastrointestinal complications, and antibody status on sublingual microvascular function. Our present study, however, provides the basis for further work to assess the diagnostic and prognostic value of this method in relation to clinical features of vasculopathy and gastrointestinal symptoms in SSc.
Our present findings indicate that automated capture and analysis of sublingual microvessel segments produces detailed, objective microvascular structural and functional data that have allowed us to distinguish patients with SSc from controls. Indeed, we have shown that markers of sublingual microvascular perfusion and glycocalyx function are lower in patients with SSc. We have also shown that microvessel lumen diameter is an important consideration in the interpretation of microvascular functional measurements, which indicates that microvascular function cannot be generalized across the entire range of microvessel lumen diameters. Collectively, our findings demonstrate a new method to assess the microvasculature in SSc and contribute additional evidence that microvascular disturbance is present in patients with SSc.
Footnotes
Supported by the US National Institutes of Health (R01 AG040297 to AJD, K23 AR067889 to TMF, and K02 AG045339 to AJD); and the US Department of Veterans Affairs (I01 CX001183 to TMF). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. HV is chief scientific officer at MicroVascular Health Solutions LLC and reports personal fees from GlycoCheck BV and MicroVascular Health Solutions LLC outside the submitted work. In addition, HV has a patent (WO2009068685): Diagnostic and Therapeutic Tools for Diseases Altering Vascular Function.
- Accepted for publication June 21, 2017.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}