

Abstract
Objective. To assess 1-year persistence and adherence rates with drug therapy among patients with fibromyalgia (FM) and to identify factors associated with therapy discontinuation.
Methods. This retrospective, cohort study included members ≥ 21 years old from the Maccabi Healthcare Services, a large health maintenance organization in Israel, who were diagnosed with FM from 2008 through 2011. Medications of interest included the anticonvulsant pregabalin, antidepressants [selective serotonin reuptake inhibitor (SSRI), serotonin/norepinephrine reuptake inhibitor (SNRI)], and tricyclic antidepressants (TCA). Time to treatment discontinuation and proportion of days covered (PDC) with FM-specific therapies during the year from first dispensed were analyzed. PDC < 20% was considered low adherence and PDC ≥ 80% was considered high adherence. Logistic regression models were constructed for multivariable analyses.
Results. Overall, 3932 patients with FM were included; 88.7% were female. Pre-diagnosis use of medication of interest was documented in 41% of the study population. Of the remaining 2312 patients, 56.1% were issued a prescription, 45.0% were dispensed at least 1 medication in the year following diagnosis, and only 28.8% had prescriptions filled twice within the first year from diagnosis. Among newly prescribed patients, 1-year discontinuation was highest for TCA (91.0%) and lowest for SSRI/SNRI antidepressants (73.7%). Over half of the patients (60.5%) had fewer than 20% of the days covered by any medication during the year and only 9.3% were very adherent (PDC ≥ 80%).
Conclusion. This study clearly shows that in an Israeli “real-life” population of patients with FM, persistence and adherence with FM therapy in the year following diagnosis is remarkably low.
Fibromyalgia (FM) is a chronic disorder affecting about 2% to 5% of the female adult population worldwide1,2,3. It is characterized by widespread musculoskeletal pain, often accompanied by fatigue, allodynia, and hyperalgesia4,5,6. Treatment is focused on alleviating pain, increasing restorative sleep, and improving physical function. It includes nonpharmacologic approaches such as exercise- or cognitive-based therapies and pharmacologic treatments7. All the medications have a neuromodulatory function, such as tricyclic antidepressant (TCA) compounds, selective serotonin reuptake inhibitor (SSRI), and serotonin/norepinephrine reuptake inhibitor (SNRI) antidepressants, or the anticonvulsant pregabalin.
The literature is scarce regarding patient acceptance of the disorder and adherence to therapy. Arnold, et al5 observed that 33% of patients prescribed duloxetine were considered very adherent, with greater adherence at lower dosages. Adherence levels tend to be better with acute pain conditions compared to chronic disorders8,9. Patients with chronic conditions that require ongoing therapy, such as allopurinol for gout, often stop taking their medication once they feel that their disease has stabilized10. Improving adherence to medical therapy decreases health service use and costs, and results in improved quality of life8,9.
In addition to lack of effectiveness or intolerance, poor adherence to therapy can be due to patient characteristics, including a belief that pain is an inherent part of the disease; cognitive barriers, such as concerns regarding analgesic use (fear of addiction and adverse events); and with certain medications, such as antidepressants, fear of family and societal reactions. Other factors that increase the risk of nonadherence to medication include psychological problems, particularly depression, poor patient-clinician communication, short duration under a rheumatologist’s care, comorbidities, and lack of familial or social support8,9,10,11. Poorly controlled symptoms can evolve into frequent encounters with primary and secondary healthcare services, as well as hospitalizations, resulting in excessive laboratory and imaging use and higher medical expenditures12. It seems that patients with FM may experience all these factors, as demonstrated by Kim, et al13, who used a large population-based US cohort study of more than 70,000 patients with FM. These authors showed that only one-fifth of the patients continued with their prescribed therapy for more than a year. In our study, we assessed adherence and persistence with therapy among patients with FM and identified factors associated with low compliance in a real-world setting.
MATERIALS AND METHODS
Setting
In Israel, all citizens are entitled to complete healthcare through 1 of 4 public health maintenance organizations (HMO). These HMO cover all aspects of primary, secondary, and tertiary care, with a minimal copayment for services. They are obligated to accept any citizen who wants to join. Maccabi Healthcare Services (MHS) is the second largest HMO in the country, providing healthcare to over 2 million enrollees (about 25% of the population in Israel). MHS maintains comprehensive electronic health records. Data automatically updated in this database are all physician visits, medical diagnoses, prescribed and dispensed medications, laboratory data, imaging, procedures, and hospitalizations. In addition to clinical information, all relevant logistic and economic data are available and can be analyzed, primarily for medical management purposes. The diagnoses in this database are valid and have been used by us in several previous studies10,14,15,16,17.
Study population
Using the MHS database, we identified and included all members at least 21 years of age, diagnosed with FM from January 1, 2008, through December 31, 2011, by rheumatologists, neurologists, psychiatrists, pain specialists, primary care physicians (≥ 2 diagnoses given on different dates), or during hospitalization. Diagnosis of FM was defined by the International Classification of Diseases, 9th ed (ICD-9) code 729.1 or an equivalent internal MHS code. To ensure identification of incident cases only, patients with prior diagnosis of FM were excluded from the study, as well as patients with less than 2 years of MHS membership and/or less than 16 months of followup (Figure 1). Analyses of persistence with treatment were confined to patients’ first prescribed FM medications during the year after diagnosis. A total of 4680 patients with FM were assessed for study eligibility. Excluded were 437 suspected of being non-incident cases and another 311 who did not fulfill the required period of MHS membership.
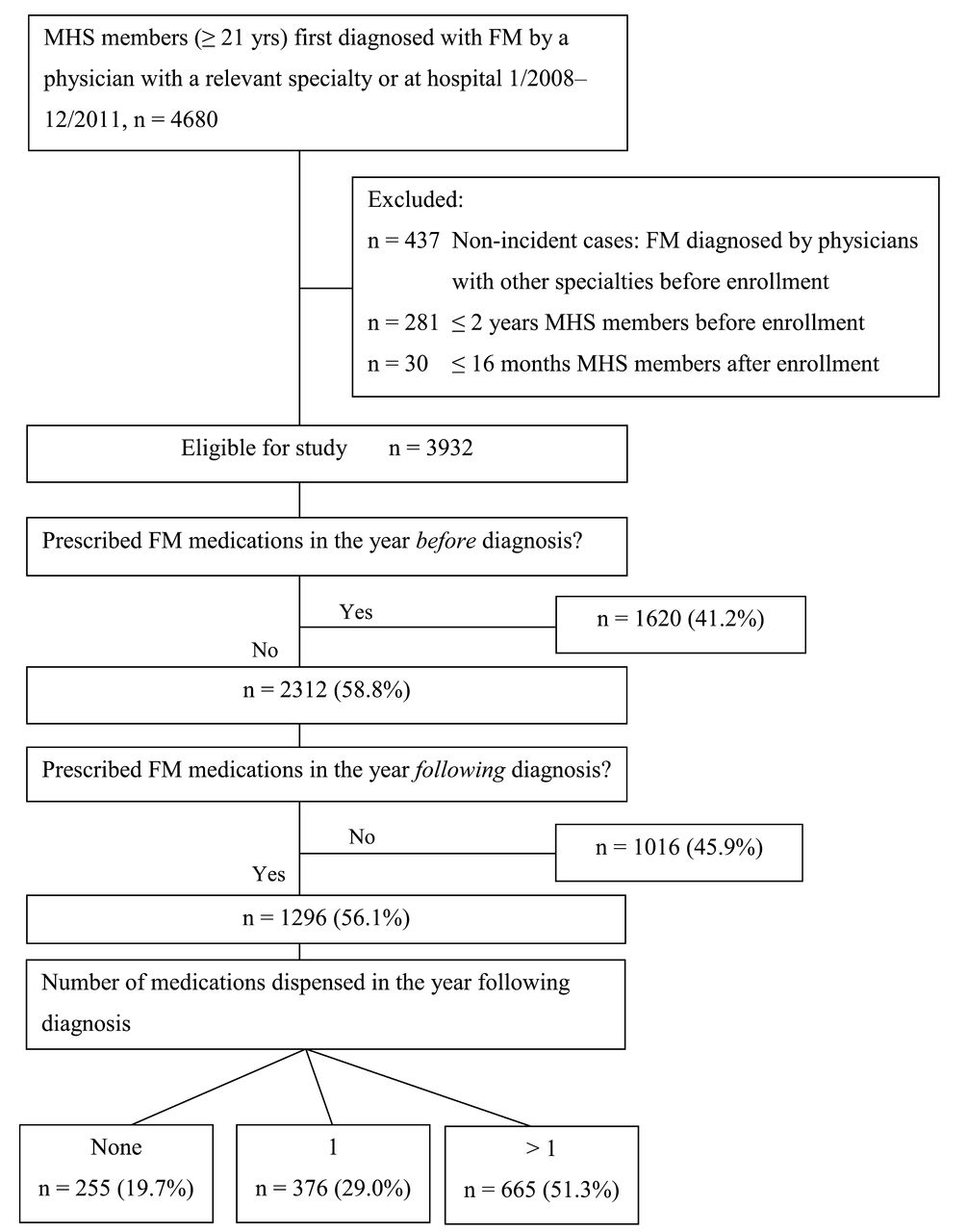
Attrition of patients from the study and distribution of eligible study patients according to FM medications prescribed and actually dispensed. FM: fibromyalgia; MHS: Maccabi Healthcare Services.
Adherence and persistence
The index date for analyses was defined as the date FM medications were first dispensed. Medication groups included antiepileptics (gabapentin, pregabalin) or antidepressants including SSRI/SNRI (venlafaxine, duloxetine, milnacipran citalopram, escitalopram, fluoxetine, paroxetine), or TCA (amitriptyline). It should be mentioned that the personal expenses (“out-of-pocket”) required for purchase of duloxetine or pregabalin in Israel are relatively high, reaching US$20–$60 a month, whereas the costs of the other medications are almost entirely covered by the health insurance. The total followup period for each patient was 485 days from date of first dispense, allowing 1 full year and an additional 120 days, because discontinuation was defined as a minimum gap of 120 days in treatment (see below). For patients who were prescribed but did not dispense medications, the index date was the date of diagnosis. Combination of treatments from more than a single medication group was defined by dispensing different medication groups on the same date.
Data collection
Patient data collected at the index date included demographics [age, sex, socioeconomic status (SES), and date of immigration] and the following clinical characteristics presented with the specific ICD-9 codes: anxiety (300.00, 300.01, 300.02), depression (300.4, 311, 296.2x, 296.3x), anxiety and depression-unified diagnosis (300.4, 300.09), fatigue (780.7), migraine (346.x), osteoarthritis (OA; 715.x), arthritis (716.9), irritable bowel syndrome (564.1), systemic lupus erythematosus (695.4), or restless leg syndrome (333.94). Treatment data included the dates the medications were prescribed and dispensed, amounts, and the number of treatment days. SES was defined according to the poverty index of the member’s residence area as defined during the 2008 national census. The poverty index is based on several variables, including household income, education, crowding, material conditions, and car ownership, and ranges from 1 to 20 based on cluster analysis with 1 as the lowest SES and 20 the highest18. Similar to the definition of FM, baseline medical conditions related to FM conditions were counted if diagnosed by a physician of relevant specialty or by a primary physician during visits on at least 2 different dates.
Statistical analysis
The chi-square test for categorical variables and the nonparametric Mann-Whitney U test for continuous variables were used to compare baseline characteristics between patient groups.
Persistence with therapy was assessed by time to treatment discontinuation and adherence by proportion of days covered (PDC) during 1 year from the date first dispensed. Patients with no medication dispensed within 1 year of diagnosis were assigned PDC of 0%. Discontinuation with FM therapy was defined as a gap of at least 120 days between drug supplies or end of followup. Days to discontinuation of treatment overall and by drug group (antiepileptic, antidepressants, TCA) are presented using medians, interquartile ranges (IQR), and Kaplan-Meier plots. PDC by any medication and by drug group were divided into quintiles of 0%–19%, 20%–39%, 40%–59%, 60%–79%, and 80%–100%, and the proportion of patients within each group is presented. We characterized patients at lowest level of adherence (PDC < 20%) versus more adherent patients (PDC ≥ 20%), and those at the highest level of adherence (PDC ≥ 80%) versus patients with lower adherence (PDC < 80%)10. Logistic regression models were constructed for multivariable analyses. Minimum Akaike information criteria were used to determine which baseline variables to include in the final model. Finally, OR and 95% CI were calculated and p for trend using the chi-square test for trend was used to assess the association of ordinal variables with adherence, using the medians of independent variable categories as category values.
We have received the approval of the MHS ethics board to conduct this study (approval number 2/2013).
RESULTS
There were 3932 eligible patients (88.7%, n = 3486 women; mean age 49.2 yrs). Among these, 1620 (41.2%) received a prescription for an FM medication in the year prior to diagnosis. Of the remaining 2312 patients, 1296 (56.1%) were issued a prescription in the year after diagnosis, and 1041 (45.0%) had at least 1 medication dispensed during this year (Figure 1). Of these, 50% initiated treatment within 14 days from diagnosis and 75% within 3 months. Only 665 (63.8% of 1041) had at least 1 additional prescription within a year from the diagnosis. However, of 376 patients with only 1 prescription, 93 (24.7%) had medications dispensed in the second year after the first prescription.
Patients prescribed in the year preceding FM diagnosis (n = 1620) were on average 3 years older than those not prescribed [n = 2312, mean (SD) years: 50.9 (12.4) vs 48.0 (12.7), respectively; p < 0.001] and were slightly more likely to be immigrants (21.2% vs 17.6%; p = 0.005). Anxiety and/or depression at baseline were much more prevalent among patients who were prescribed treatment prior to FM diagnosis than among those not previously prescribed (72.5% vs 32.8%, respectively; p < 0.001). Among the 2312 patients who were not previously prescribed FM medications, factors associated with receiving a prescription after diagnosis were baseline anxiety and/or depression (36.5% prescribed vs 28.1% non-prescribed patients; p < 0.001). They were more likely to be diagnosed by a primary care physician (47.0% vs 39.7%) and less likely to be diagnosed during hospitalization (0.8% vs 6.4%; p < 0.001). Among prescribed patients, 59.1% received TCA, 46.7% antidepressants (SSRI/SNRI), and 24.1% antiepileptics (Table 1).
Medications prescribed and dispensed in the first year from diagnosis and proportion and time to discontinuation in the year following first time dispensed (n = 1296). Values are n (%) unless otherwise specified.
Combination of treatments from more than 1 group was rare, as indicated by same-date dispenses of medication from 2 or more treatment groups. During the year post first dispense of any treatment, only 52 of 1041 patients (5.0%) dispensed combinations of 2 medication groups. Half of these patients (n = 25) dispensed both SSRI/SNRI and TCA, 21 patients dispensed antiepileptics and SSRI/SNRI, and another 6 patients dispensed antiepileptics and TCA. For the majority of these patients (n = 31, 59.6%), this was a single dispense of 30 supply days, with no difference between specific combinations, and only 9 persisted with > 90 supply days.
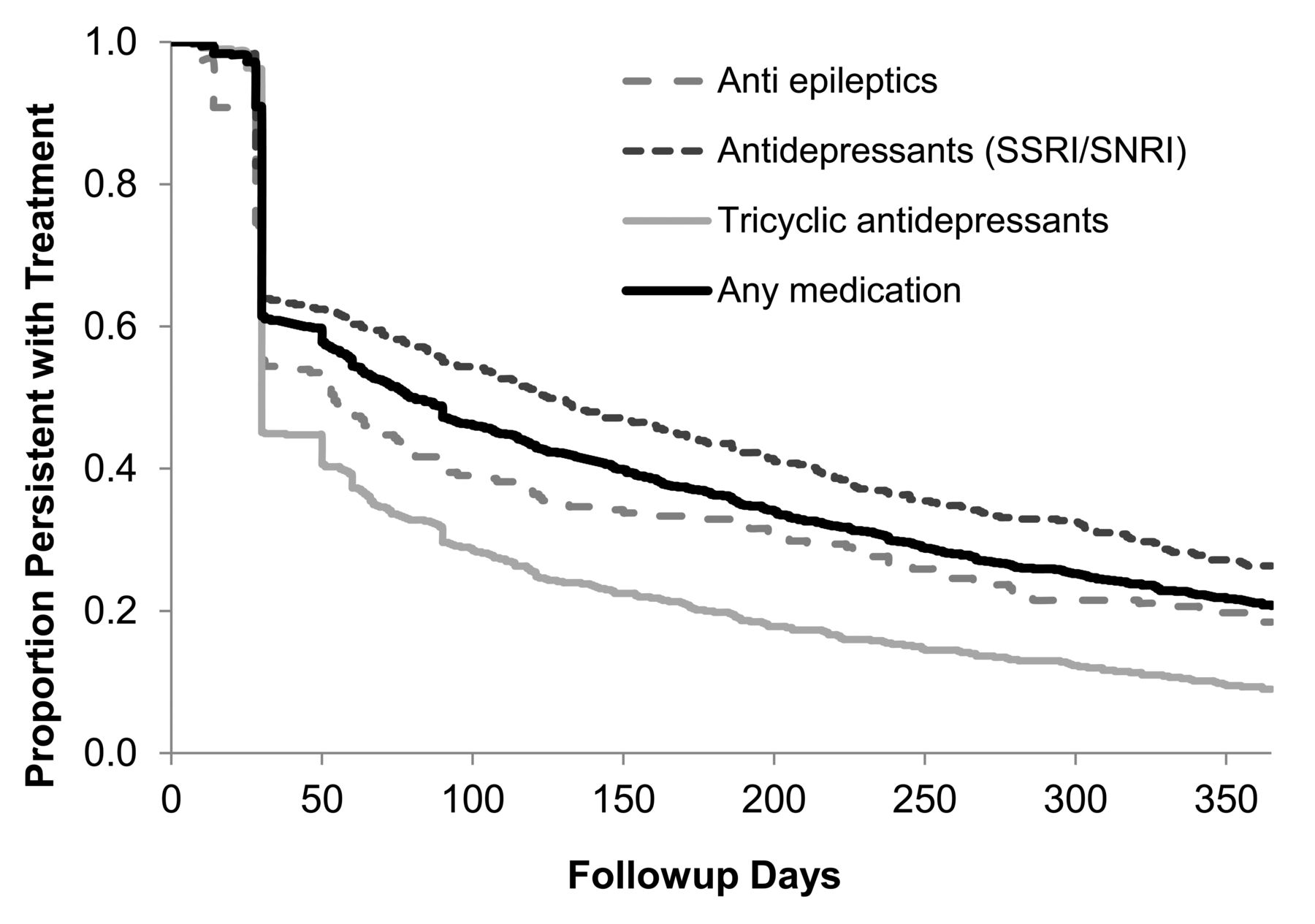
Overall, 80.3% (n = 1041) of the patients newly prescribed post-diagnosis filled a prescription within 1 year of diagnosis. Of these, 825 (79.3%) discontinued therapy during the year following the first dispense (Table 1, Figure 2). The highest discontinuation rate was seen among patients prescribed TCA (91.0%) and the lowest rate among those prescribed antidepressants (SSRI/SNRI; 73.7%). After 1 year from initiation of SSRI/SNRI antidepressants, TCA, or anti-epileptics, 26.3%, 18.4%, and 9.0%, respectively, were still medically treated. Only 20.7% still received any medication 1 year after initiation of treatment.

Kaplan-Meier plot for time from first dispensed to discontinued, overall, and by drug group among patients with at least 1 dispense (n = 1041). SSRI: selective serotonin reuptake inhibitor; SNRI: serotonin/norepinephrine reuptake inhibitor.
Out of a total of 1153 patients prescribed any antidepressant during the year post-diagnosis, 36.4% had a diagnosis of anxiety and/or depression prior to prescription, and of those who realized a prescription, 45.5% had such a diagnosis.
Among prescribed patients, baseline characteristics were compared between those with any FM medication dispensed at least twice to those who had none dispensed or who stopped treatment after a single prescription. In multivariate analysis, having at least 2 dispensed FM medications was associated with anxiety and depression at baseline versus none or either of these conditions (OR 1.86, 95% CI 1.33–2.60; p < 0.001) and with migraines at baseline (OR 1.34, 95% CI 1.03–1.73).
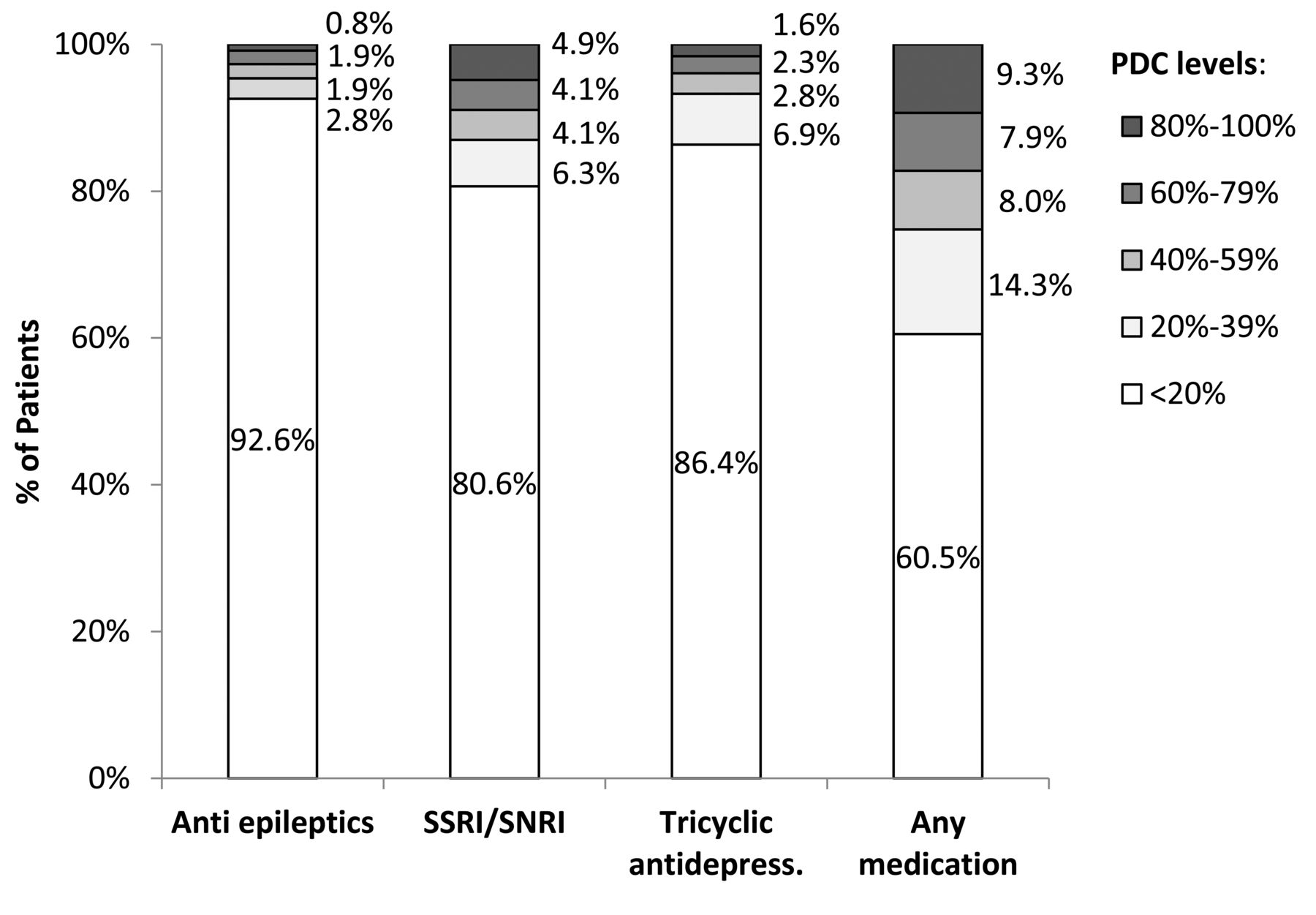
Among prescribed patients, the mean (SD) PDC by any medication during 1 year from first time dispensed was 26.0% (28.6%), median 14.9% (IQR 7.7–40.2%), corresponding to 3.1 and 1.8 months, respectively. Over half of the patients (60.5%) had fewer than 20% of the days covered and only 9.3% were regarded as adherent (PDC ≥ 80%; Figure 3). Although patients prescribed with antidepressants were more adherent to therapy, the median PDC for these medications was low (Figure 3).
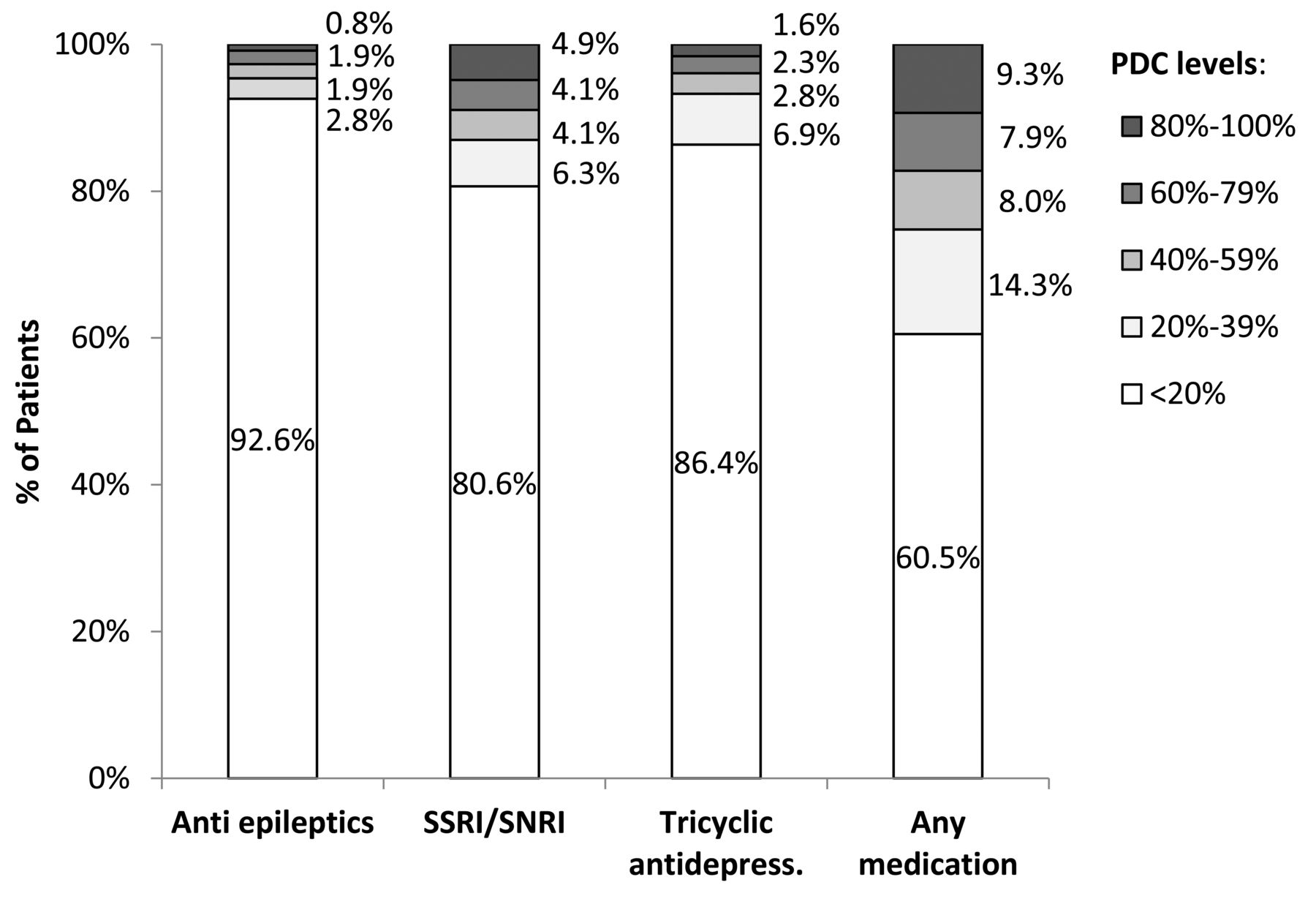
Proportion of patients within PDC categories during 1 year after index date, overall, and by treatment group (n = 1296). PDC: proportion of days covered; SSRI: selective serotonin reuptake inhibitor; SNRI: serotonin/norepinephrine reuptake inhibitor.
Patients with higher SES, immigrants, and those diagnosed with anxiety, depression, or migraines were more likely to adhere (PDC ≥ 20%; Table 2). In multivariate analysis, being an immigrant, and having anxiety and depression, and migraines increased the chance for adherence, with OR 0.73, 0.55, and 0.62, respectively. Patients in the highest SES quintile were also more likely to adhere compared with those in the lowest quintile, with a borderline linear trend across quintiles (p for trend = 0.108).
Univariate and multivariate associations between patient characteristics and low adherence (PDC < 20%; n = 1296).
For any FM medication, the only factor associated with PDC ≥ 80% versus PDC < 80% was SES (Table 3), although even in the highest SES quintile, only 32 patients out of 282 (11.3%) were adherent compared with 16 patients out of 282 (5.7%; p for trend = 0.022).
Univariate associations between patient characteristics and adherence with treatment (PDC ≥ 80%) for any FM medication in the year post first dispense (n = 1296). Values are % (n) unless otherwise specified.
DISCUSSION
The results of our real-world data study indicate relatively poor prescription fill rates for FM medications among naive patients, and poor persistence and adherence rates with therapy among those initiating treatment. Coexistent migraines and diagnosis of both anxiety and depression were associated with a lower likelihood of low adherence, possibly representing patients with different presentations of FM or different severity of symptoms19. High adherence rates (PDC ≥ 80%) were associated with SES only. Although overall persistence and adherence rates were very low, financial constraints may have prevented some patients from purchasing medications. However, adherence rates for TCA, which are inexpensive, were similar to those of other, more expensive drugs.
Recently, treatment patterns among adults with a first diagnosis of FM were retrospectively assessed using US health insurance claims20. Only 31% initiated treatment, and many patients received less than the recommended dose. Duloxetine had the highest mean PDC (59%), which was below 50% for all other agents. Similarly, in a retrospective cross-sectional study from the United States, Cui, et al21 reported low levels of adherence to therapy among patients with FM. Among 4660 patients, only 33% had high adherence with duloxetine. Factors associated with high adherence included older age, prior antidepressant or anticonvulsant use, and comorbid dyslipidemia or OA. In another study, among 4869 patients with FM with commercial insurance and 566 with Medicare, two-thirds had low adherence. Higher average daily dose of duloxetine was associated with increased adherence12.
Similar to previous studies, we found differences in compliance when comparing different types of medications, though after 1 year from first prescription, only 21% were still taking any medication. TCA were more quickly abandoned compared to other drug groups, possibly because of higher rates of side effects or lower efficacy. Persistence and adherence were higher for SSRI and SNRI antidepressants compared with the other drug groups. Our results differ from previous reports that patients with chronic disorders who also have comorbid depression are less compliant with medical therapy9. DiMatteo, et al11 reported that in general, depressed patients were 3× more likely to be noncompliant with medical treatment than the nondepressed. Our report supports previous observations that improvement of a depressive episode may contribute to accepting the potential benefit of therapy and ultimately to higher adherence rates22. However, in our analysis we focused on treatment patterns among newly prescribed patients, thus excluding those already receiving antidepressants at diagnosis.
Robinson, et al23 analyzed 1700 patients with FM and observed that those treated with duloxetine and milnacipran had fewer outpatient visits during their 12-month followup study as compared with those treated with pregabalin or TCA. These findings are complementary to ours, demonstrating superior outcomes with antidepressants compared with antiepileptics and TCA, probably because of better persistence rates.
Low compliance rates may indicate low levels of satisfaction with treatment. Our data corroborate the report by Wolfe, et al24, who described in an 11-year longitudinal study the changing patterns of analgesic and centrally acting drugs used in FM (pregabalin, duloxetine, milnacipran). These authors observed that the 25th and 50th discontinuation percentiles of these drugs were following 1 and 2.5 years, respectively. Other reviews revealed that the improvement of patients with FM treated with these new medications was only marginal. Different metaanalyses have demonstrated that significant clinical improvement by the newer approved medications for FM was evident in only 10% of the patients on average while the rate of adverse events ranged between 70% and 90%25,26,27,28. These data are in line with our results showing extremely low persistence rates in real-life use, implying that only a small minority of patients who achieve clinical benefit are willing to continue with these medications for intervals longer than a year.
Our current study has several limitations. First, as in any database study, medical conditions were identified based on ICD-9 diagnostic codes recorded in the MHS database, which may be subject to inaccuracies. However, only diagnoses from relevant sources were included in our study and over half of the patients were diagnosed in secondary care. In addition, compliance was assessed only among prescribed patients, increasing the chance that only actual FM cases were identified. Second, evaluating persistence and adherence with treatment is challenging. We used real-world data from the MHS database regarding prescribing and dispensing medications, including detailed information on type of drug, number of pills, and number of treatment days10,14,15,16. This data source allowed us to study a large, population-based cohort of patients, but limited our ability to determine whether patients actually took the medications. Another limitation was the small sample of prescribed patients, which did not allow evaluation of combinations of treatments. An important limitation was that data pertaining to severity or duration of FM, pain levels, ethnicity, employment status, and familial status were not available, and we could not assess the use of over-the-counter medications for pain relief or of nonpharmacological treatments. Such variables may be associated with adherence and persistence outcomes and their inclusion might have resulted in improved identification of key patient subgroups. We emphasize that our report is valid for the Israeli population and might differ in other ethnicities.
Finally, it should be remembered that patients with FM may present with symptoms of anxiety or depression; thus it is an inherent question whether such symptoms should be viewed as a comorbid condition or part of the FM syndrome. Even though we examined treatment patterns in newly prescribed patients, we cannot definitively state that the antidepressants were prescribed in this population for FM treatment and not for comorbidities such as depression or anxiety. Among patients with FM lacking a diagnosis of concomitant anxiety or depression, 65% were prescribed antidepressants, likely for FM therapy. Only review of text, which was not accessible for a study of large data analysis could shed more light on the reason for prescribing these antidepressants.
One of the main strengths of our study originates from the non-selected population. Our results reflect the real-life population of the second largest HMO in Israel, with a population closely reflecting the entire Israeli population and including all ethnic minorities, socioeconomic strata, and geographic locations.
Our findings stress the need for monitoring therapy adherence in patients with chronic diseases, particularly patients with FM. It is imperative to identify patients at higher risk of nonadherence, who may require additional intervention. Moreover, physicians should launch proactive, interventional actions for deterring noncompliance that address low-income individuals.
Nonadherence to therapy is usually multifactorial and may be predicted by several variables, including medication costs, level of education, or the availability of the prescribing physician. Patient-physician relationship, communication, and satisfaction with the visit are extremely important influences on medication compliance; an integral part of the clinical interaction9,10,11. Our results clearly indicate that there is an urgent need for new therapies with improved effectiveness and better tolerability for patients with FM. Physicians should keep in mind the problematic characteristic of adherence when evaluating and treating patients with FM, so that physicians can intervene and reach out to those who are at higher risk of nonadherence.
Footnotes
Supported by a research grant given by Pfizer.
- Accepted for publication May 26, 2017.








{kind=link}
{kind=link}
{kind=link}