

Abstract
Objective. Tenosynovial giant cell tumor (TGCT) is a rare benign proliferative and inflammatory disease arising from synovia of joints, bursae, or tendon sheaths. We aimed to estimate incidence rate and prevalence of TGCT in Denmark, to describe patient characteristics and treatment modalities among patients with TGCT, and to estimate risk of TGCT recurrence.
Methods. Using registry data on pathology examinations and inpatient and outpatient hospital diagnoses, we identified adult patients with diagnoses of diffuse TGCT (D-TGCT) or localized TGCT (L-TGCT) between 1997 and 2012, followed through 2012. We described patients’ characteristics, treatment modalities, and recurrence.
Results. We identified 2087 patients with L-TGCT and 574 patients with D-TGCT. Their incidence rates per million person-years were 30.3 (95% CI 29.1–31.7) and 8.4 (95% CI 7.7–9.1), respectively. At the end of 2012, prevalence per 100,000 persons was 44.3 (95% CI 42.4–46.3) for L-TGCT and 11.5 (95% CI 10.6–12.6) for D-TGCT. Women made up 61% of the patients with L-TGCT and 51% of the patients with D-TGCT. Median age at diagnosis was 47 years. Ten-year risk of recurrence was 9.8% (95% CI 8.4–11.3%) after L-TGCT and 19.1% (95% CI 15.7–22.7%) after D-TGCT.
Conclusion. This study contributes evidence about epidemiology of TGCT based on routinely collected population-based data gathered in a setting of universal equal access to healthcare and complete followup.
Tenosynovial giant cell tumor (TGCT), formerly known as pigmented villonodular synovitis (PVNS), is a benign proliferative and inflammatory condition arising from synovia of joints, bursae, or tendon sheaths1,2. Depending on the form, the estimated annual incidence rate of TGCT ranges from 1.8 per million1 to 50 per million3. TGCT affects primarily persons at ages 20–50 years2 and presents either as a single nodule [localized TGCT (L-TGCT)] or as multiple nodules [diffuse TGCT (D-TGCT)] along a synovial layer or tendon sheath2,4. TGCT mainly affects large joints such as the knee and the hip1,5, but may also affect fingers3 and rarely, the temporomandibular joint or the spine6. Etiology of TGCT is thought to have inflammatory and neoplastic components7,8. Clinical diagnosis is often challenging because of largely nonspecific symptoms. A definitive diagnosis is made histologically or by magnetic resonance imaging2. Treatment options are surgical open synovectomy, radio-synovectomy, external-beam radiotherapy, cryosurgery, immunotherapy, arthroplasty, or amputation2,9. Lifetime recurrence risk is up to 15% for L-TGCT and up to 55% for D-TGCT2. Complications include infections, osteoarthritis, pain, and worsened quality of life2,5,6. Because of its rarity and challenging diagnostics, evidence regarding TGCT comes primarily from case series2,4,6,10,11,12,13,14. Two population-based studies were based on routine radiology and pathology records in the Netherlands3,5.
In our cohort study, based on routinely recorded population-based registry data in Denmark, we aimed to estimate incidence rate and prevalence of TGCT, to describe patient characteristics and initial surgery, and to estimate risk of TGCT recurrence.
MATERIALS AND METHODS
Study setting, population, and period
Denmark is a welfare state with tax-funded universal healthcare. In the last quarter of 2012, the Danish population was 5.6 million, and the adult (age ≥ 18 yrs) population was 4.4 million (www.statistikbanken.dk). Our study population included patients with TGCT diagnosis, identified based on the definitions described below, from January 1, 1997, through December 31, 2012, followed through December 31, 2012. We excluded persons with a record of the International Classification of Diseases (ICD)-10 diagnosis of TGCT before January 1, 1997 (since January 1, 1994, because there was no ICD-8 code for TGCT), and patients with a diagnosis of a malignant soft tissue tumor recorded since 1977 before or on the date of TGCT diagnosis during the study period. The latter exclusion criterion was applied to reduce contamination by malignant disease. The study start date was selected to ensure completeness of both pathology and hospital diagnosis data during the entire study period.
Data sources
Data for this study were linked, on patient level, from 4 nationwide Danish registries, described in detail elsewhere15,16,17,18. The Civil Registration System was used to obtain patients’ unique identifier, vital status, sex, date of birth, and residence in Denmark. The Danish National Pathology Register16, which contains detailed records of all routine pathology specimens processed in Danish pathology departments since 1997, provided data on TGCT and its localization, recorded using the Danish version of the Systematized Nomenclature of Medicine (SNOMED) codes19. The Danish National Patient Registry17, an administrative registry of inpatient (since 1977) and outpatient (since 1995) hospital encounters, was used to obtain information on diagnoses (coded using the ICD-8 through 1993, and ICD-10 thereafter), and surgical procedures coded using the Nordic Medico-Statistical Committee classification20. The Danish National Health Services Prescription Database18 contains data on reimbursed outpatient dispensations from 2004, including date of dispensation and the active substance, coded according to the Anatomical Therapeutic Chemical (ATC) classification21. This database was used to identify use of prescription medication by patients with TGCT.
Definition of TGCT
TGCT definitions based on routine data were developed in consultation with orthopedic surgeons and pathologists, based on SNOMED and ICD-10 diagnostic codes. L-TGCT was defined using a specific SNOMED code for localized L-TGCT or a nonspecific code for benign synovioma, as recorded in the Danish National Pathology Register. The specific code was introduced in Denmark in 2011. To increase specificity of the L-TGCT definition, only diagnoses associated with plausible TGCT topography, indicating location in a joint, were included after tabulating the topographies recorded for all potential cases. Topography codes included are listed in the Supplementary Material (available with the online version of this article). D-TGCT was defined using either the specific SNOMED code for D-TGCT or the ICD-10 code for “pigmentous villonodular synovitis” (the term used at the time). Within each definition, the date of TGCT diagnosis was defined as the date of the first recorded eligible code.
Patients’ characteristics
The baseline period to describe characteristics of patients with TGCT extended 36 months before the date of TGCT diagnosis (inclusive), i.e., not earlier than January 1, 1994, to ensure uniform use of the ICD-10 classification in the Danish National Patient Registry (the malignancy exclusion criterion was applied since 1977). The following baseline characteristics were assessed (using categories as listed in Table 1): sex; age at TGCT diagnosis, calendar year of diagnosis, diagnostic or treatment procedures; history of musculoskeletal (MSK) injuries; fracture of upper or lower limbs; history of selected chronic diseases; history of chemotherapy; and indicators of healthcare use. Among the patients with a diagnosis of TGCT from 2004 onward and up to 36 months before the index date, we additionally assessed history of use of selected prescription medications and the number of drug classes as defined by the first letter (anatomic category) of the ATC code.
Incidence rates of tenosynovial giant cell tumor, overall and by calendar year, sex, and age group, Denmark, 1997–2012.
Initial surgery
We searched the Danish National Patient Registry for codes of operations on the MSK system from 15 days before through 30 days after the TGCT diagnosis date (inclusive). We allowed a 15-day pre-diagnosis period to accommodate a potential administrative delay in recording of diagnoses following a therapeutic operation. Exploratory analyses indicated that most operations were identified by this period. Operations on the MSK system were classified as exploratory procedures, including biopsy; operations assumed to be for TGCT treatment; and all other operations. The numbers and proportions of the patients with at least 1 operation in each of the 3 categories were reported, and a patient could contribute to more than 1 category. In the category “operations assumed to be for TGCT treatment,” each patient contributed only once, with the first-recorded operation. This category of operations was further subdivided into operations on synovia and joint surfaces; operations on muscles and tendons except in pelvis or hip/thigh; operations of fascia, ganglia, synovial sheaths and bursae; and operations for tumors. Each patient contributed only once to the overall category and the subcategory with the first-recorded operation. For the exploratory procedures and operations assumed to be for TGCT treatment, the distributions of skeletal regions of the first-recorded procedure were reported.
Recurrence
TGCT recurrence was defined as a new record of TGCT diagnosis more than 30 days after the date of the incident TGCT diagnosis. We constructed Kaplan-Meier curves of up to 10-year, recurrence-free survival after L-TGCT and D-TGCT using this definition. In a sensitivity analysis, we required more than 90 days to elapse from the incident diagnosis to define recurrence.
All codes used to identify the study variables are listed in the Supplementary Material (available with the online version of this article).
Statistical analysis
L-TGCT and D-TGCT were analyzed separately. The number and the proportion of patients younger than 18 years of age on the date of the TGCT onset were reported. All subsequent analyses were restricted to persons who were 18 years or older on the date of TGCT diagnosis.
The incidence rate of TGCT (overall, by calendar year, sex, and age) was estimated, per million person-years, as the number of incident adult TGCT cases in the corresponding underlying adult Danish population. Prevalence of TGCT was calculated as the proportion of people with the disease alive at the end of 2012, assuming that TGCT does not resolve and cannot be cured (complete prevalence22). Patients with a prior diagnosis who have recurrent or residual disease and those with amputation or tumor prosthesis are also included in this definition. The estimates of incidence rates and prevalence were reported with 95% Poisson CI.
We used SAS 9.2 (SAS Institute Inc.) software to analyze the data.
This study received approval by the Danish Data Protection Agency, required for all research in Denmark (journal number 2014-54-0922), and by the Department of Clinical Epidemiology, Aarhus University Hospital (journal number KEA-2015-7). The authors confirm that ethical/institutional review board approval for research based solely on registry data is not required by Danish law.
RESULTS
Between January 1, 1997, and December 31, 2012, we identified 2087 patients with L-TGCT and 574 patients with D-TGCT. Eighty-two patients with L-TGCT and 28 with D-TGCT diagnosed before 18 years of age were excluded from further analyses.
The overall incidence rate (95% CI) per million person-years was 30.3 (29.1–31.7) for L-TGCT and 8.4 (7.7–9.1) for D-TGCT. The incidence rates remained stable over calendar years, were greater for women than for men, and were highest among persons between 40 and 59 years of age (Table 1). At the end of 2012, prevalence (95% CI) per 100,000 persons was 44.3 (42.4–46.3) for L-TGCT and 11.5 (10.6–12.6) for D-TGCT (Table 2).
Prevalence of tenosynovial giant cell tumor in Denmark as of the end of 2012.
Table 3 shows baseline demographic and clinical characteristics of the patients with L-TGCT and with D-TGCT. The proportion of women was 61% among the patients with L-TGCT and 51% among the D-TGCT. About three-quarters of the patients in both groups were younger than 60 years at diagnosis; median age at diagnosis was 47 years (range 18–91 yrs) in both groups. Among the patients with L-TGCT, 9.7% had a history of injury to spine or limbs in 36 months preceding the diagnosis, including 3.1% with a history of a fracture. Among the patients with D-TGCT, prevalence of injury of the spine and limbs was 17.1%, and prevalence of history of fracture was 4.4%. Up to 60% of the patients with D-TGCT had a history of osteoarthritis. Nearly one-third of the patients had a history of dispensation of an antibiotic, an antiinflammatory, or antirheumatic agent. Premorbid history of hospitalization was lower among patients with L-TGCT than among patients with D-TGCT.
Baseline characteristics and healthcare use of the patients with L-TGCT and D-TGCT, Denmark, 1997–2012, ascertained starting January 1, 1994, and up to 36 months before and including the index date. Values are n (%) unless otherwise specified.
Table 4 shows distribution of operations and healthcare use, as recorded from 15 days before to 30 days after the TGCT diagnosis. Three percent of patients with L-TGCT and 14% of patients with D-TGCT had an exploratory operation on the MSK system, most frequently on the knee joint and lower leg. Twenty-eight percent of patients with L-TGCT and 43% of patients with D-TGCT had an operation on the MSK system assumed to be for TGCT treatment. For the patients with L-TGCT, the most frequent skeletal region of the first such operation was wrist and hand, followed by knee. For the patients with D-TGCT, the most frequent skeletal region was the knee, followed by the wrist and hand. Among all other operations on the MSK system, the most frequent were various operations on the joints, including primary prosthetic joint replacements. For the first-recorded procedure of that type, the most frequent skeletal region was knee joint and lower leg.
Surgical procedures recorded among patients with L-TGCT and D-TGCT from 15 days before through 30 days after the diagnosis, Denmark, 1997–2012. Values are n (%).
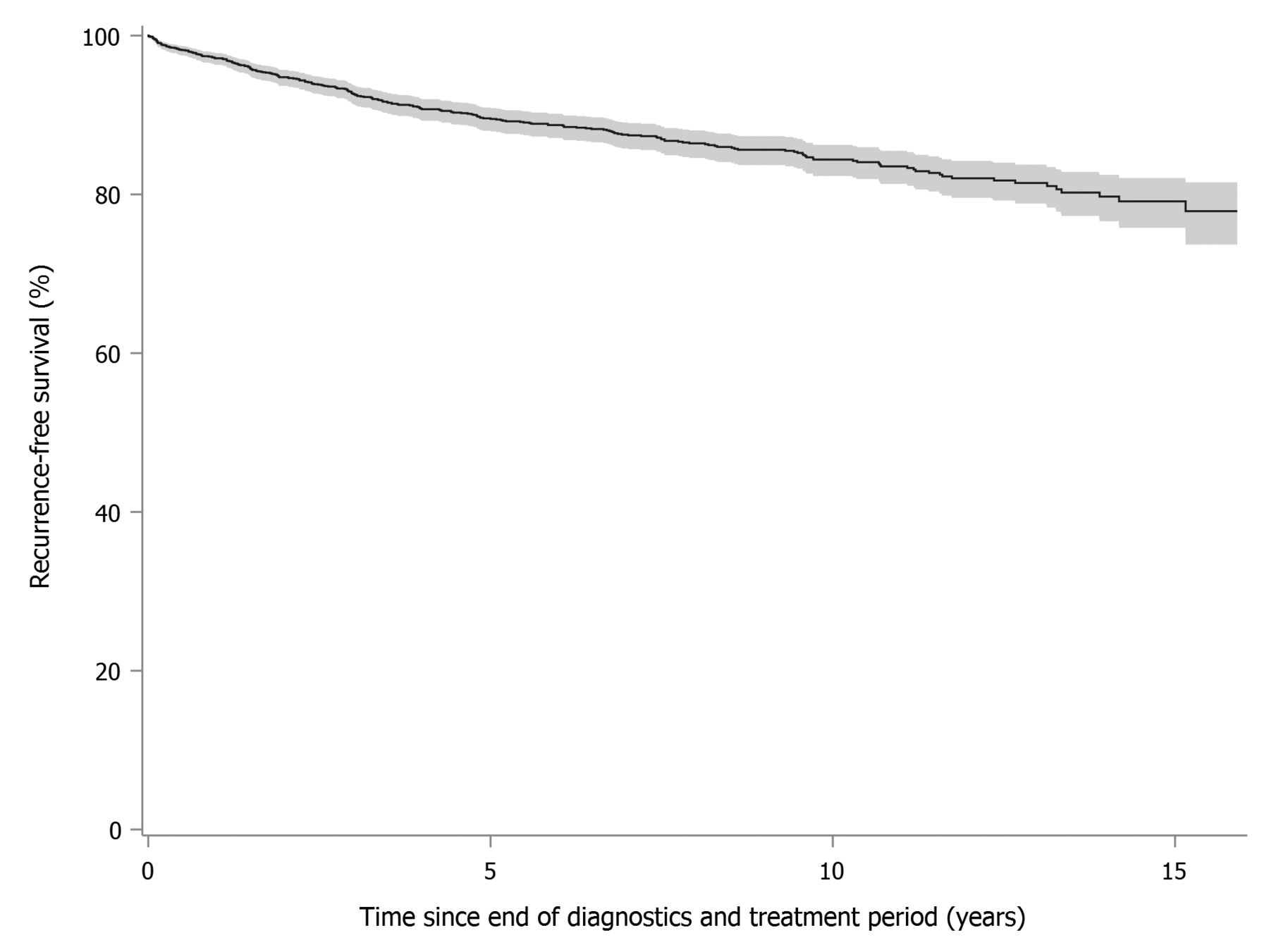
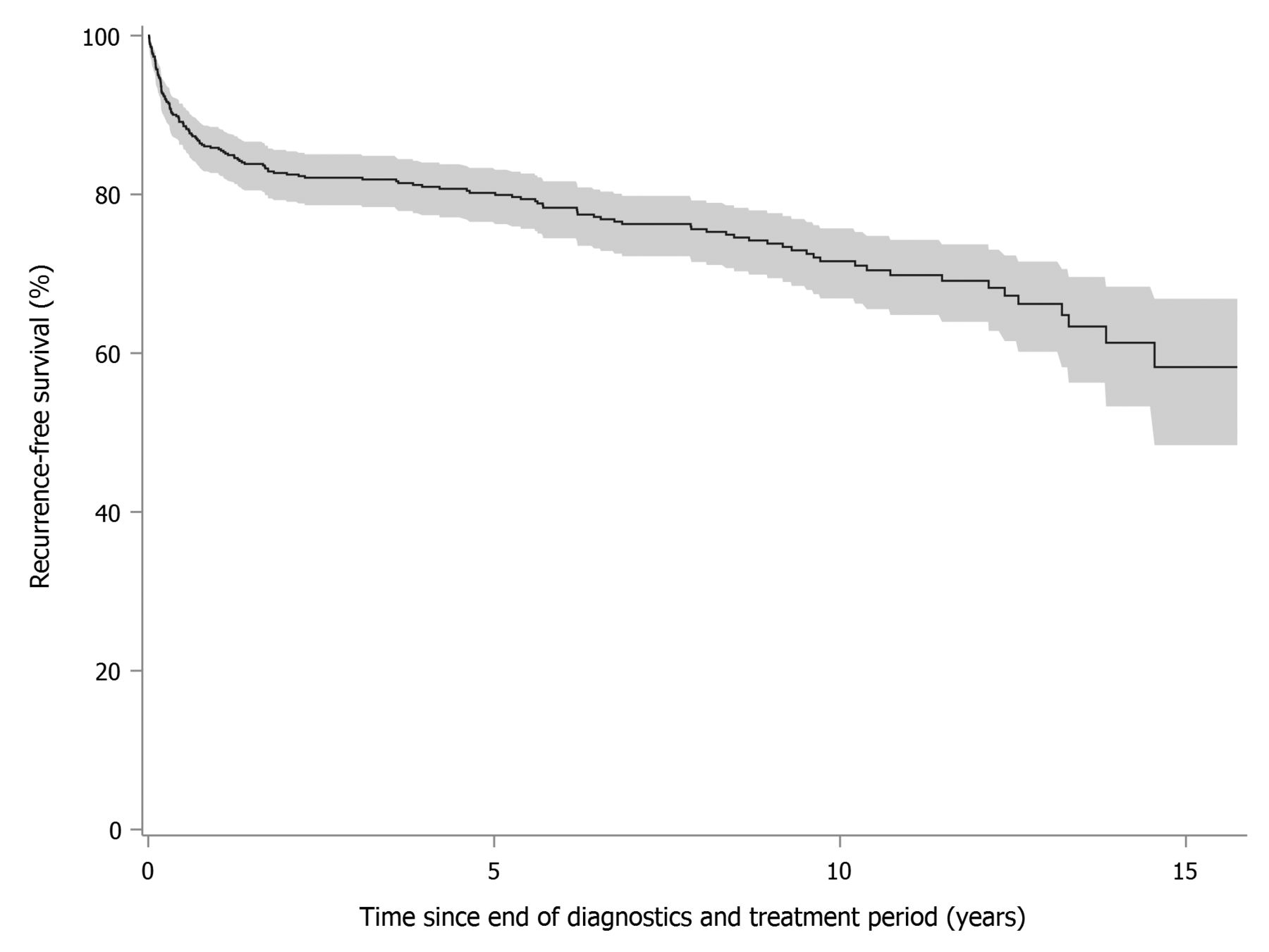
The 10-year risk of recurrence was lower for L-TGCT (9.8%, 95% CI 8.4–11.3%) than for D-TGCT (19.1%, 95% CI 15.7–22.7%). Figure 1 and Figure 2 show Kaplan-Meier curves for recurrence-free survival with 95% confidence bands among patients with L-TGCT and D-TGCT. In a sensitivity analysis requiring 90 days to elapse before a newly recorded diagnosis was considered a recurrence, the 10-year risk of recurrence was 8.9% (95% CI 7.6–10.4%) for L-TGCT and 15.5% (95% CI 12.4–18.9%) for D-TGCT.
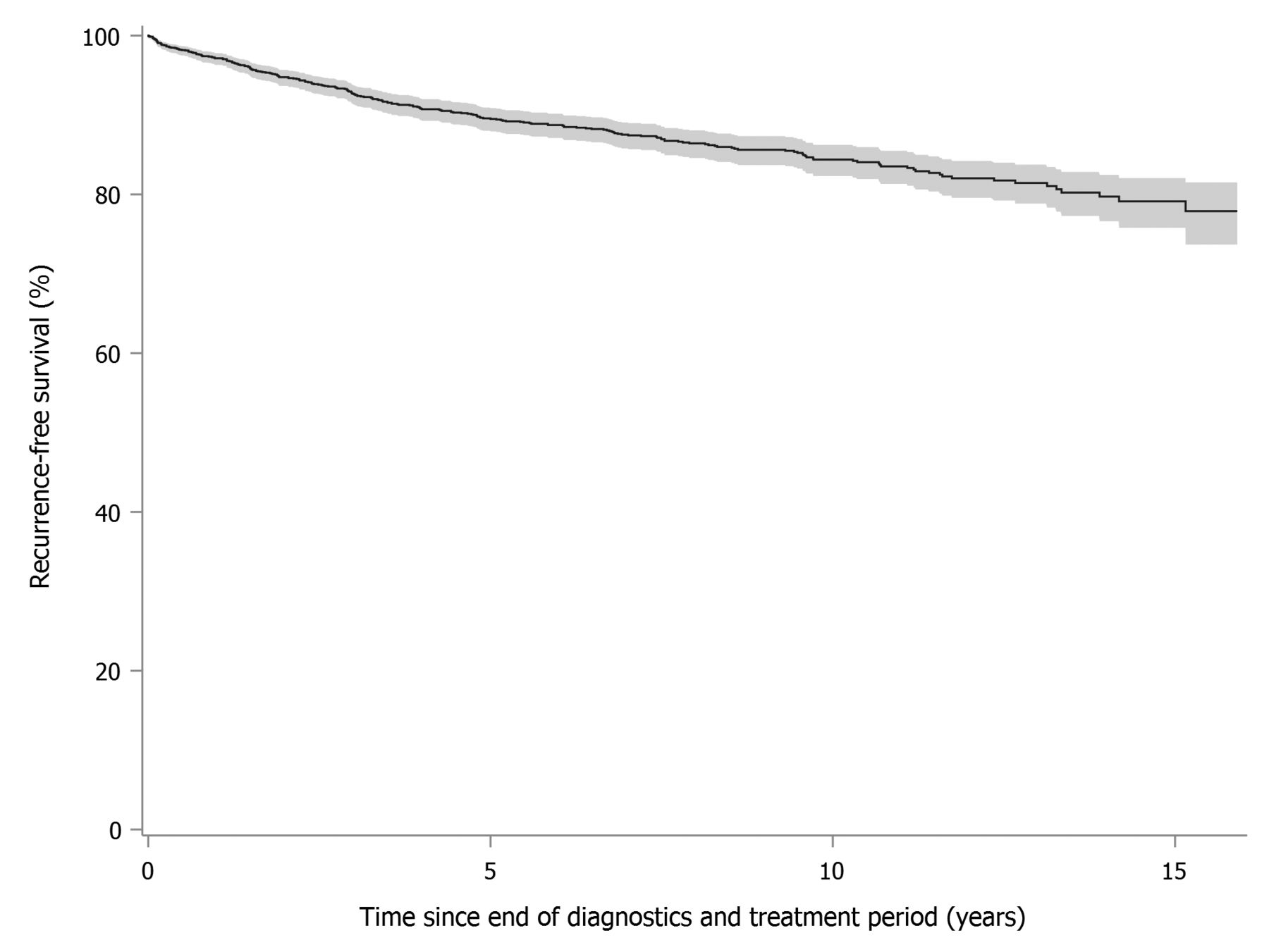
Kaplan-Meier curves for recurrence-free survival after L-TGCT, Denmark, 1997–2012. L-TGCT: localized tenosynovial giant cell tumor.
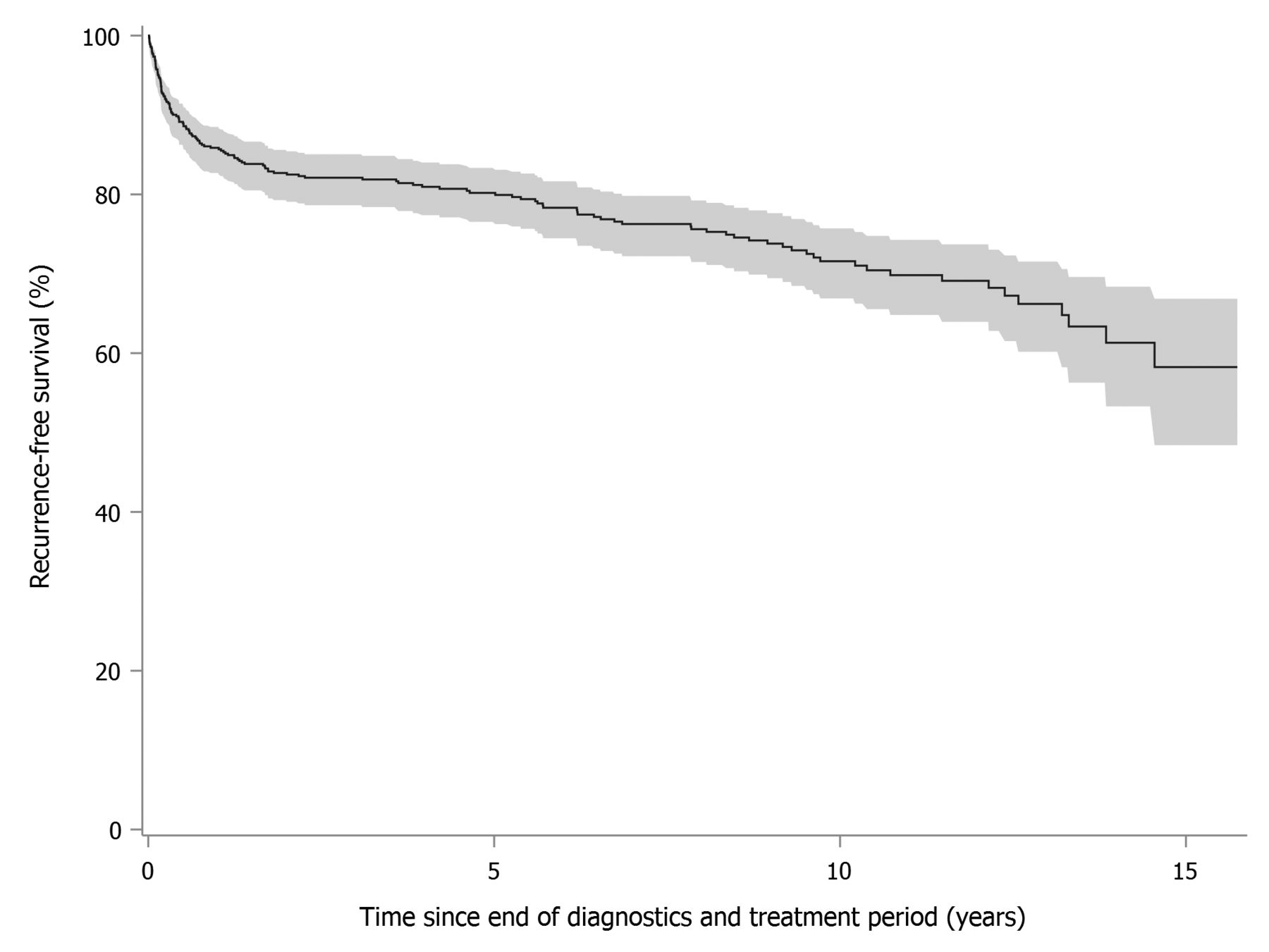
Kaplan-Meier curves for recurrence-free survival after D-TGCT, Denmark, 1997–2012. D-TGCT: diffuse tenosynovial giant cell tumor.
Supplementary Table 1 (available with the online version of this article) shows topography distributions for L-TGCT and D-TGCT.
DISCUSSION
In our nationwide cohort study based on routinely and prospectively collected data over a 16-year period in Denmark, the incidence rate was 30 per million person-years for L-TGCT and 8 per million person-years for D-TGCT. The population prevalence in 2012 was 44 per 100,000 for L-TGCT and 11 per 100,000 for D-TGCT. The 10-year risk of recurrence was lower for L-TGCT than for D-TGCT (9.8% vs 19.1%).
Our study was set in Denmark’s universal healthcare system, with a long tradition of registration, individual-level linkage, and virtually complete followup of the entire population. This setting virtually eliminates selection bias because of enrollment or attrition. Procedure codes in the Danish National Patient Registry have high validity and completeness, as do SNOMED codes in the Danish Pathology Register15,16. Limitations of our study are the lack of validated algorithms to identify TGCT and its subtypes (especially L-TGCT and the risk of reciprocal misclassification of the L-TGCT and D-TGCT), lack of clinical detail (such as symptoms) in the secondary data, and lack of imaging results, which are often used to diagnose TGCT14. It is possible that entered pathology diagnosis codes stem from intrasurgery pathologic evaluation and therefore reflect observations done during surgery. The study period lies before the adoption, in 2013, of the World Health Organization diagnostic criteria for TGCT23. Especially in the earlier calendar years (before 2005), the localized TGCT definition relies on nonspecific pathology codes, including codes for benign synovioma. Although we restricted the nonspecific codes to those likely to occur with TGCT (as listed in the Supplementary Material, available with the online version of this article), erroneous inclusion of benign synoviomas cannot be ruled out. Thus, the definition for L-TGCT may be relatively more sensitive pre-2005 in identifying true TGCT cases, but is relatively less specific in that it is likely to have included an unknown proportion of conditions that are not TGCT. At the same time, estimates of TGCT incidence and prevalence include only cases that have come to medical attention and/or were treated. Estimates of recurrence in our study were lower than those reported by others2, most likely because we based the definition of recurrence on diagnostic codes recorded at hospital encounters. It was not possible based on the available data to identify surgeries specific for recurrence of TGCT. Exclusion of code-identifiable malignant tumors of soft tissue has helped increase the specificity of all definitions. Cases of TGCT that were diagnosed based on imaging diagnostics alone, if identified, are likely reflected in the diffuse TGCT, because that definition includes ICD-10 codes, which could be assigned following diagnostic imaging. Because the ICD-10 code for PVNS (term used in the ICD-10 classification) has been available from 1994 onward, and people live long with the disease, an unknown proportion of prevalent TGCT cases could not be removed from the study population before the start of the inclusion period. Some prevalent TGCT cases may have been removed by excluding patients with a record of ICD-8 codes for benign neoplasms of bone, muscle, and connective tissue.
Estimated incidence of TGCT, patients’ demographic characteristics, and the distributions of the surgical operations assumed to be for TGCT treatment and their skeletal regions were consistent with those reported for patients with TGCT elsewhere3,5. Most notably, the distributions are consistent with the results of the 2014 population-based study from the Netherlands5. The 2 studies, originating from different research groups and different study populations, but concordant in showing a preponderance of women among the patients with L-TGCT and nearly equal proportions of men and women among the D-TGCT cases, agreed in the overall distribution of the lesions’ topography and yielded comparable estimates of recurrence-free survival, even though recurrence cannot be definitively discriminated from residual disease based on diagnostic codes alone. It is possible, however, that data completeness is lower for recurrences than for the primary disease. Similar to our study, the Dutch study relied on data from routine pathology records to identify TGCT, based on 107 cases of L-TGCT and D-TGCT combined5. There were also differences in the 2 studies. Our study identified a substantially greater number of patients in both L-TGCT and D-TGCT groups, despite a shorter study period and a smaller population size in Denmark. This difference may be attributable to under-ascertainment of the cases in the Netherlands and/or over-ascertainment of the cases in Denmark [although estimated combined incidence rate of L-TGCT and D-TGCT from another Dutch study (50 per million)3 was similar to that estimated in our study (38 per million)]. In contrast to the Dutch study, the L-TGCT group was more numerous in our study than the D-TGCT group; this is partially because of the lack of specificity of the L-TGCT definition applied in Denmark, owing to the absence of a specific code during most of the study period and to the inclusion, in Denmark, of hospital discharge diagnoses in addition to the pathology diagnoses. The sensitivity of the Danish definition is likely bolstered by use of the diagnostic ICD-10 codes, in addition to pathology diagnoses. ICD-10 codes were likely to identify TGCT cases diagnosed using imaging diagnostics alone (without pathology diagnoses, on which the case definition relied in the Dutch study). The reported prevalence, especially for L-TGCT, may be overestimated because it was computed based on the assumption of no cure, while L-TGCT may be cured after a single surgery.
Our study set out to determine the incidence rate and prevalence of this rare disorder using a large, well-maintained healthcare system. The results of our study are in line with the documented rarity of TGCT. Although pathophysiology of TGCT is probably universal, extrapolations of the age- and sex-specific results from Denmark to other populations should be done while accounting for differences in population structures. There is very little information available about the burden and clinical course of TGCT. This population-based study using routinely collected data may be used to guide future studies into this debilitating disease.
Our study, based on routine registry data in Denmark, contributes population-based evidence about the incidence rate and prevalence of pigmented villonodular synovitis and about selected patient characteristics.
ONLINE SUPPLEMENT
Supplementary material accompanies the online version of this article.
Acknowledgment
We thank Dr. Steen Bærentzen and Professor Peter Holmberg Jørgensen for expert advice regarding diagnostic codes, and Kelsey Biddle for support with literature review and study initiation.
Footnotes
This study was partially funded by a research grant from Five Prime Therapeutics Inc., issued to and administered by Aarhus University Hospital.
- Accepted for publication May 18, 2017.








{kind=link}
{kind=link}