

Abstract
Objective. To describe pulmonary involvement at time of diagnosis in antineutrophil cytoplasmic antibodies (ANCA)-associated vasculitis (AAV), as defined by computed tomography (CT).
Methods. Patients with thoracic CT performed on or after the onset of AAV (n = 140; 75 women; granulomatosis with polyangiitis, n = 79; microscopic polyangiitis MPA, n = 61) followed at a tertiary referral center vasculitis clinic were studied. Radiological patterns of pulmonary involvement were evaluated from the CT studies using a predefined protocol, and compared to proteinase 3 (PR3)-ANCA and myeloperoxidase (MPO)-ANCA specificity.
Results. Of the patients, 77% had an abnormal thoracic CT study. The most common abnormality was nodular disease (24%), of which the majority were peribronchial nodules, followed by bronchiectasis and pleural effusion (19%, each), pulmonary hemorrhage and lymph node enlargement (14%, each), emphysema (13%), and cavitating lesions (11%). Central airways disease and a nodular pattern of pulmonary involvement were more common in PR3-ANCA–positive patients (p < 0.05). Usual interstitial pneumonitis (UIP) and bronchiectasis were more prevalent in MPO-ANCA–positive patients (p < 0.05). Alveolar hemorrhage, pleural effusion, lymph node enlargement, and pulmonary venous congestion were more frequent in MPO-ANCA–positive patients.
Conclusion. Pulmonary involvement is frequent and among 140 patients with AAV who underwent a thoracic CT study, almost 80% have pulmonary abnormalities on thoracic CT. Central airway disease occurs exclusively among patients with PR3-ANCA while UIP were mainly seen in those with MPO-ANCA. These findings may have important implications for the investigation, management, and pathogenesis of AAV.
Antineutrophil cytoplasmic antibodies (ANCA)-associated vasculitis (AAV) is a group of systemic inflammatory diseases in which a necrotizing vasculitis of the small blood vessels has the potential to attack multiple organ systems, but with a propensity for attacking the upper and lower respiratory tracts, eyes, skin, and kidneys1. AAV is divided into 3 clinicopathological entities: granulomatosis with polyangiitis (GPA), microscopic polyangiitis (MPA), and eosinophilic granulomatosis with polyangiitis (EGPA; formerly Churg-Strauss Syndrome). Two ANCA specificities are recognized, consisting of myeloperoxidase (MPO-ANCA) and proteinase 3 (PR3-ANCA)1. PR3-ANCA is most commonly associated with GPA while MPO-ANCA is more frequent in MPA. A genome-wide association study found that MPO-ANCA– and PR3-ANCA–associated vasculitis are genetically distinct entities, providing biological support for a disease classification based on serology2. ANCA specificities are associated with relapse risk, differences in disease extent and severity, and renal outcome, and have been proposed to be used in AAV classification3,4. Advances in diagnosis and treatment have transformed AAV from a rapidly fatal disease, with an untreated 1-year mortality of 80%5, to a relapsing and remitting disorder that still has significant morbidity and mortality over the longer term.
Pulmonary involvement from both acute and chronic disease processes is common in AAV and has been reported in 25%–80% of cases6,7,8,9,10. Some patterns of pulmonary involvement seen in AAV, such as nonspecific interstitial pneumonia, are themselves associated with a grave prognosis even without AAV with 10-year survival rates of 35%11. Pulmonary disease is increasingly recognized as an important contributing factor to the persistently raised morbidity and mortality in AAV, with early lung involvement being associated with severe organ damage and poor outcomes in GPA12,13. Imaging, mainly computed tomography (CT), is key for the diagnosis and prognostication of lung involvement, but the spectrum of radiological findings in AAV remains poorly defined. The limited evidence mainly focuses on GPA or is limited by small sample sizes14,15,16,17. Notably, as few as 18% of MPO-ANCA–positive patients have been shown to have normal thoracic CT studies in 1 study18.
Improved understanding of the characteristics and extent of pulmonary involvement in AAV is an essential step to better understand, and possibly intervene against, the role played by pulmonary disease in morbidity and mortality. Therefore, our study aimed to describe pulmonary involvement as defined by thoracic CT in a large cohort of patients with AAV and investigate the role played by ANCA seropositivity in pulmonary disease in AAV.
MATERIALS AND METHODS
Study cohort
Patients followed at the Vasculitis and Lupus Clinic, Addenbrooke’s Hospital, Cambridge, UK, and for a known diagnosis of AAV (n = 260 patients with 133 women; GPA, n = 122; and MPA, n = 138) with a thoracic CT study performed (54%) were eligible for participation. Demographics, clinical, and laboratory data were collected from time of AAV diagnosis. The diagnosis of AAV was verified by case record review. The classification of cases into GPA or MPA was based on the European Medicine Agency 2007 classification algorithm19. All patients were diagnosed between June 2000 and October 2012, and followed to either death or June 1, 2014.
In accordance with UK National Health Service Research Ethics Committee guidelines, ethical approval was not required for this work because it consists of retrospective data, and all treatment decisions were made prior to our evaluation.
Data collection
Demographics and clinical data including sex, age, and signs and symptoms at diagnosis were collected from case records. Organ involvement was recorded by the Birmingham Vasculitis Activity Score (version 3)20. Laboratory data were collected at the date of diagnosis, including ANCA positivity (MPO-ANCA or PR3-ANCA), C-reactive protein, and serum creatinine. Renal outcome was defined by endstage renal disease (ESRD). Organ involvement at any point during the disease course was assessed according to the Disease Extent Index (DEI)21.
Thoracic CT
Two thoracic radiologists, blinded to the patient’s clinical data, consensus-read all thoracic CT studies. The imaging findings were registered as specific diseases when interpreted as being most consistent with specific, predefined imaging patterns that were in accordance with internally accepted imaging criteria22.
Pulmonary involvement
Pulmonary involvement was classified according to zonal distribution (mid, upper, and lower) and centrifugal pattern (diffuse, central, or peripheral), and the severity of involvement was quantified as estimated percentage involvement. Parenchymal features included22 (1) consolidation, where increased attenuation obscured the underlying vessels, (2) ground glass opacity, area of hazy increased attenuation without obscuration of the underlying vascular markings, (3) reticulation, innumerable interlacing lines, suggesting a mesh, (4) honeycombing, clustered cystic airspaces of 3–10 mm in diameter with shared well-defined walls of 1–3 mm, with layering in the subpleural lung, and (5) atelectasis, focal reduction in volume, accompanied by increased attenuation in the affected lung (nondependent or dependent). For these abnormalities, the presence of architectural distortion was defined by abnormal displacement of bronchi, vessels, fissures, or septa. A nodule was defined as a rounded or irregular opacity, well or poorly defined, measuring up to 3 cm in diameter (mass when above 3 cm). Central airways involvement was detected as central airways thickening and stenosis. Bronchiectasis was diagnosed as bronchial dilatation with respect to the accompanying pulmonary artery, a lack of tapering of the bronchi and the identification of bronchi within 10 mm of the pleural surface (traction when there was surrounding architectural distortion). Only bronchiectasis was scored according to lobar distribution, and classed as mild (luminal diameter slightly greater than diameter of adjacent blood vessel), moderate (lumen 2–3× the diameter of the vessel), or severe (lumen > 3×)23. Peribronchial thickening was graded as mild (wall thickness equal to diameter of adjacent vessel), moderate (wall thickness greater than and up to twice the diameter of adjacent vessel), or severe (wall thickness > 2× the diameter). Small airway disease was detected by the presence of air trapping on expiratory scans, or if there were focal zones of both decreased attenuation and vascularity. Emphysema was defined as focal areas or regions of low attenuation without visible walls, which was graded as mild, moderate, or severe, and centrilobular or paraseptal. Pulmonary venous congestion was recorded when there was peripheral smooth interlobular septal thickening without architectural distortion, with or without central ground glass opacity and pleural effusions. Additional registered features included pleural effusion, pericardial effusion, and lymph node enlargement (> 10 mm).
Disease patterns
Usual interstitial pneumonitis was diagnosed when there was a reticular pattern with subpleural honeycombing of basal predominance with or without architectural distortion and traction bronchiectasis, or when there was a bilateral peripheral reticular pattern without honeycombing and with architectural distortion and traction bronchiectasis. Nonspecific interstitial pneumonitis was defined by ground glass opacity with fine reticulation, and with or without traction bronchiectasis, but no/limited honeycombing. Pulmonary hemorrhage was defined as areas of ground glass opacification with subpleural sparing, with or without crazy paving pattern, areas of consolidation, or smooth interlobular septal thickening, but no volume loss. Other patterns included (1) scarring when there was linear nondependent atelectasis, (2) bronchiectasis, when there was bronchiectasis without traction, (3) peribronchovascular nodularity with or without cavitation, (4) pulmonary venous congestion when there was dependent smooth interlobular septal thickening without volume loss or architectural distortion and with or without pleural effusions, and (5) other involvement, such as pneumonia.
Statistical analyses
Statistical analyses were performed using the Statistical Package for the Social Sciences; SPSS 22.0 for Windows (IBM SPSS). The differences in the frequency of organ involvement between groups were studied using the chi-square test. Patient and renal survival were studied by the Kaplan-Meier method, with differences between groups investigated using the log-rank test. Normally distributed variables are presented as means ± SD, and Student t test was used for comparisons. Continuous, not normally distributed data are presented as median with interquartile ranges (IQR), and the Mann-Whitney U test was used for comparisons. Differences in the frequency of pulmonary involvement were studied after stratifying patients according to the serology subtypes, positive PR3-ANCA versus MPO-ANCA and according to disease phenotypes (GPA vs MPA). A p value of < 0.05 was considered significant.
RESULTS
There were 140 (79 GPA and 61 MPA; 75 women) out of a total of 260 patients with AAV who had thoracic CT examinations available and could be included in our study (54%). Patients with thoracic CT studies were more likely to have been classified as GPA and PR3-ANCA–positive, and they had more ENT and chest symptoms. However, there were no differences in other organ manifestations or outcomes compared with the 120 patients with no available thoracic CT studies (Table 1).
Demographic, clinical, and laboratory characteristics of patients with ANCA-associated vasculitis with and without available CT studies.
Diagnosis of AAV was confirmed by histopathology in 103 (74%) of the included patients. The mean age at diagnosis was 60.1 ± 14.6 years. The median followup duration from AAV diagnosis to death or June 2014 was 70 months (IQR 42–98). Most patients had systemic disease with multiple organs involved at the time of diagnosis, with a mean DEI at diagnosis of 6.3 ± 2.5. Positive serology results were available for 129 patients (92%), 81 (63%) were positive for PR3-ANCA and 48 (37%) for MPO-ANCA. Ten patients had negative ANCA, and 1 patient was positive for both PR3- and MPO-ANCA (excluded from analyses). Selected demographics and laboratory characteristics of patients with PR3-ANCA and MPO-ANCA disease are shown in Table 2.
Demographic, clinical, and laboratory characteristics in patients with positive ANCA (n = 129).
Computed tomographic findings
Only 32 patients (23%) had a normal thoracic CT study. There were no differences in sex distribution, age at diagnosis, inflammatory activities, mean DEI, and mean creatinine at diagnosis between patients with normal thoracic CT examination compared with those with CT abnormality (data not shown). The most common radiological findings were nodular opacities (24%), with the majority being peribronchial in distribution, followed by bronchiectasis and pleural effusions (19%, each), pulmonary hemorrhage and lymph node enlargement (14%, each), emphysema (13%), and cavitating lesions (11%). Figure 1 shows a number of selected findings on CT studies in patients with AAV.
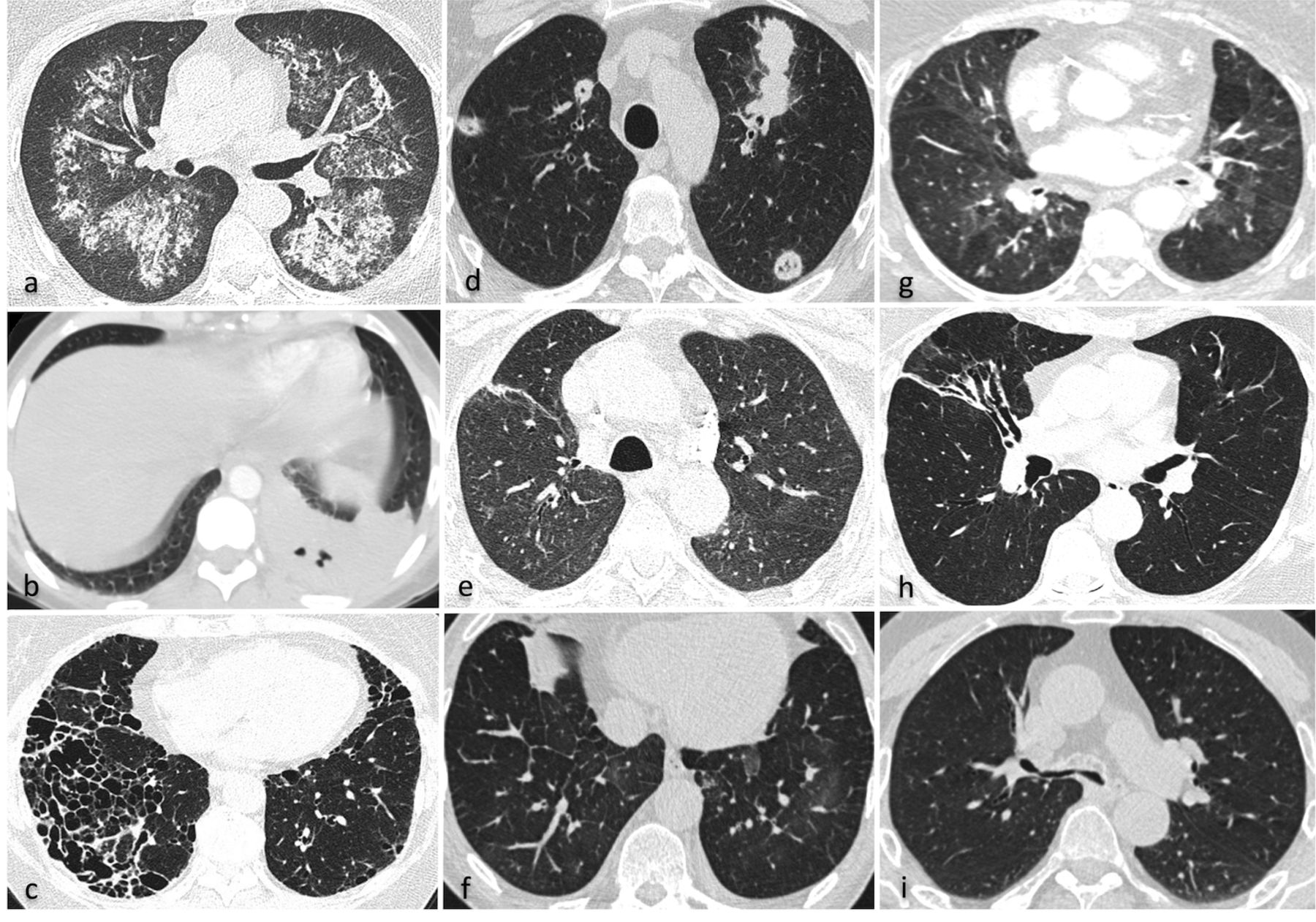
Lung involvement as indicated by computed tomography in a large cohort of patients with ANCA-associated vasculitis, including: (a) pulmonary hemorrhage, (b) necrotizing pneumonia, (c) usual interstitial pneumonitis, (d) cavitating lung nodules, (e) parenchymal scarring, (f) pulmonary venous congestion, (g) small airways disease, (h) bronchiectasis, and (i) large airways stenosis. ANCA: antineutrophil cytoplasmic antibodies.
Thoracic CT findings according to ANCA specificity
Thoracic CT findings among patients with ANCA positivity are shown in Table 3. No pulmonary abnormality was present in 28 of 129 patients with positive ANCA (PR3-ANCA in 19, 24% and MPO-ANCA in 9, 19%; p = 0.5). Clinically evident involvement of respiratory symptoms or signs was evident in 33% among those with normal CT studies compared to 60% of patients with at least 1 CT abnormality (p = 0.01). No other differences were found in demographics or clinical features between the 2 groups.
Thoracic computed tomography in patients with ANCA-associated vasculitis according to ANCA serotype. Values are n (%) unless otherwise specified.
ANCA specificity and parenchymal involvement
As shown in Table 3, peripheral reticulation and honeycombing were found exclusively among patients with MPO-ANCA. Although nodular opacity in general was more common among patients with PR3-ANCA, the difference was not significant. However, nodular disease with cavitation and peribronchovascular nodules was more common with PR3-ANCA (Table 3). Central airways disease was found exclusively in PR3-ANCA–positive patients (p = 0.01) whereas bronchiectasis was more prevalent among patients with MPO-ANCA (p = 0.02; Table 3).
ANCA specificity and disease patterns
Usual interstitial pneumonitis (UIP) occurred exclusively in MPO-ANCA– positive patients (p < 0.001; Table 3). Imaging findings indicative of pulmonary hemorrhage were present in 14%, and did not segregate according to ANCA specificity. Similarly, emphysema was found in 12% with PR3-ANCA compared with 13% with MPO-ANCA.
ANCA specificity and additional findings
Pleural effusions were found in 20% of patients, most commonly bilateral and small, and more frequent in MPO-ANCA–positive patients (Table 3). Four patients (2 MPO-ANCA and 2 PR3-ANCA) had pleural plaques and 2 others had noncalcified pleural thickening (1 MPO-ANCA and 1 PR3-ANCA). Pericardial effusion was present in 6 patients (5%), of which 4 were PR3-ANCA–positive. There was no difference in the prevalence of lymph node enlargement between patients with positive PR3-ANCA and MPO-ANCA.
Thoracic CT findings according to disease phenotype
The pattern and frequencies of pulmonary abnormalities on thoracic CT for patients classified with GPA and MPA are summarized in Table 4. Central airway disease and subglottic stenosis were found exclusively in patients with GPA. Further, nodular disease pattern with cavitation and peribronchovascular nodules were also more common in GPA. Peripheral reticulation, UIP, and honeycombing were significantly more prevalent in patients with MPA.
Thoracic computed tomography in 140 patients with ANCA-associated vasculitis comparing patients with GPA and MPA. Values are n (%) unless otherwise specified.
Patients and renal survival
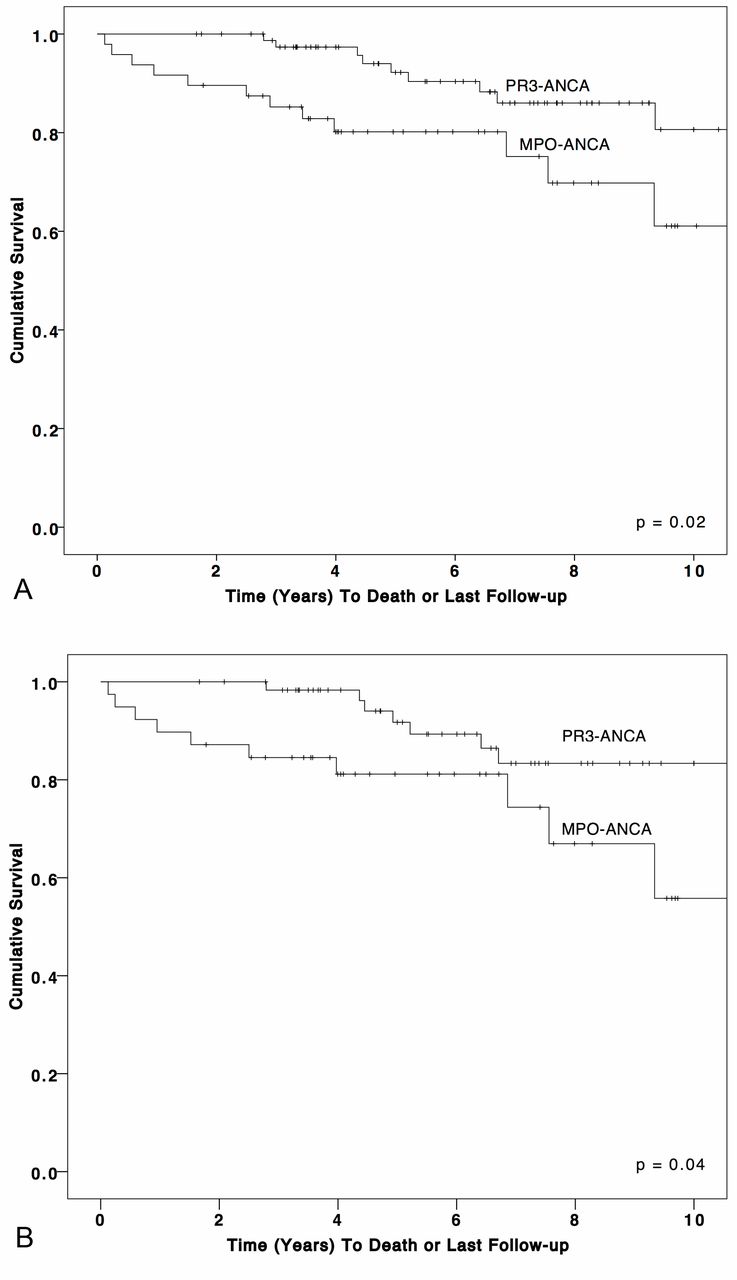
The median duration of followup was 5.8 years (IQR 3.5–8.1), during which 26 patients died (19%). The 1-, 5-, and 10-year survival rates were 97.1%, 85.3%, and 71.5%, respectively. Survival was inferior in MPO-ANCA–positive patients compared with PR3-ANCA (MPO-ANCA: 1-, 5-, and 10-yr survival was 91.7%, 80.2%, and 61.1%, respectively, vs PR3-ANCA: 100%, 92.2%, and 80.6%; p = 0.02; Figure 2A). These results were unchanged when only patients with abnormal thoracic CT scans were included (PR3-ANCA: 1-, 5-, and 10-yr survival was 100%, 91.7%, and 83.4%, respectively, vs MPO-ANCA: 89.7%, 81.2%, and 55.8%; p = 0.04; Figure 2B). There were no associations between survival and the type of pulmonary involvement (UIP, bronchiectasis, pulmonary hemorrhage, or nodular changes). Causes of deaths were infection (n = 7), malignancy (n = 3), renal failure (n = 3), ischemic heart disease (n = 2), pulmonary hypertension and heart failure (1 each), miscellaneous causes (n = 3), and unknown (n = 6; died in other hospitals). ESRD developed in 17 patients, with 14 testing positive for MPO-ANCA (Table 1 and Table 2). There was no difference in the occurrence of ESRD in relation to the presence or absence of abnormalities on CT studies. Similarly, there was no association between type of pulmonary involvement on CT studies and renal survival (data not shown).

(A) Survival curve for 129 patients with ANCA-associated vasculitis. (B) Survival curve for 101 patients with abnormal thoracic computed tomography and positive ANCA. ANCA: antineutrophil cytoplasmic antibodies; PR3: proteinase 3; MPO: myeloperoxidase.
DISCUSSION
To our knowledge, ours is the largest study to date to define the frequency and pattern of thoracic CT abnormalities in AAV. Among 140 patients with AAV who had a thoracic CT performed, almost 4 of 5 patients had abnormal imaging findings that covered a range of chronic and acute disease manifestations, with differences demonstrated in prevalence and type of involvement between ANCA serotypes. While UIP and bronchiectasis were found in patients with positive MPO-ANCA, nodular disease with cavitation and small airway disease were more common among patients with positive PR3-ANCA. Generally, there were no major differences in CT findings when comparing disease phenotype versus ANCA serotype. Previous studies on patients with AAV have shown abnormal CT chest findings in 69%–82% of patients18,24.
Idiopathic pulmonary fibrosis (IPF) is a rare disease with a prevalence estimate ranging from 0.7 to 63.0/100,00025,26,27. Interstitial lung disease (ILD) was found in 21% of our patients with positive MPO-ANCA. Patients with IPF may occasionally develop positive MPO-ANCA and be diagnosed with MPA during the course of their disease. In a prior prospective study, the prevalence of positive MPO-ANCA increased from 5% to 15% in a cohort of patients with IPF28. Pulmonary fibrosis occurs frequently in MPA, and may precede other disease manifestations29 or it can be diagnosed at the same time as AAV30. It is, therefore, important to test for ANCA in patients with evidence of ILD, especially in those with coexisting extrapulmonary manifestations. In our study, thoracic CT was performed after the onset of AAV and we cannot exclude the possibility of the occurrence of ILD before the onset of AAV. In a multicenter report of 49 patients with pulmonary fibrosis and AAV, 88% were MPO-ANCA–positive31. The prognosis was worse among patients treated only with glucocorticosteroids compared with those treated with cyclophosphamide or rituximab in combination with glucocorticosteroids. Detailed data on therapy given at induction, maintenance, or relapse are not available in our study for comparison. The absence of differences in the survival rates based on the presence of UIP in our study may be related to the small number of affected patients. However, in a recently published study from Japan, patients with ANCA-related UIP had better survival rates compared with those with IPF-related UIP32. It has been suggested that the use of immunosuppressives in treating patients with ANCA-associated UIP may explain this favorable prognosis.
Nodules, with or without cavitation, are the most common pulmonary finding in AAV as reported in 50%24,33, followed by lobar atelectasis, pulmonary bands, and infiltrates14,17. Pulmonary nodular disease is an important manifestation of GPA because it is considered as a surrogate marker for granulomatous disease in AAV and has a central role in the classification of AAV into different disease phenotypes19. Pulmonary nodules with cavitation were more common among patients with positive PR3-ANCA. Pleural effusion is a nonspecific finding, which in AAV may relate to the prevailing state of systemic inflammation, heart failure, or renal dysfunction. Pleural effusions were found in 19% overall and in 26% of patients with MPO-ANCA compared with previous reports of only 6% of 85 patients with MPA9. Pleural opacity was found in 9/77 (12%) patients with GPA; of them, 4 had pleural effusions34 while only 2 of another series of 30 patients with GPA from our hospital had pleural disease, 1 had pleural effusion, and 1 multiple calcified pleural plaque15.
Large airway disease, including tracheal and bronchial stenosis and bronchial wall thickening, was more prevalent with PR3-ANCA disease in our study and was found in 11% compared with none with MPO-ANCA. Central airway disease in GPA has been reported in 15%–25% in previous studies14. PR3-ANCA is genetically distinct from MPO-ANCA and is more likely to involve granulomatous inflammation2. Interaction with respiratory bacteria has been associated with PR3-ANCA disease whereas occupational exposure to silica has been associated with MPO-ANCA seropositivity35,36,37. As an indicator of chronic airways injury, bronchiectasis was found in almost 20% of our cases, and it was more prevalent among patients with positive MPO-ANCA and less than the 44% rate reported previously38. Speculatively, treatment given in AAV might modulate the risk of bronchiectasis because the development may relate to inflammatory changes in AAV39. Thus, the reported differences in imaging appearances may represent differences in the etiology and pathogenesis of PR3-ANCA and MPO-ANCA disease. Current treatments do not differentiate between these serotypes, but further understanding may lead to more specific therapies. In our study, survival was better for patients with positive PR3-ANCA. However, we are presenting nonadjusted data for age and renal disease, which are 2 factors that might explain the difference in prognosis.
Ours is a retrospective study from a single center and therefore may be affected by referral bias and missing data. Almost all patients were white, there was an absence of prediagnosis information, and not all thoracic CT studies were performed at the time of diagnosis. Referrals for CT were on a patient-by-patient clinical basis with a potential bias toward those patients with respiratory signs and symptoms or severe disease. All available thoracic CT studies were evaluated for our study by 2 thoracic radiologists, independently and using a predefined form; increasing the reliability of the findings and the consistency in descriptions of imaging appearances. Owing to the retrospective design of our study and our clinical practice during the study period, no correlation with invasive diagnostic methodologies such as lung biopsy or bronchoalveolar lavage was available. However, internationally acknowledged imaging definitions of disease patterns were deployed and all CT studies were systematically consensus-read by 2 radiologists into a context of “imaging patterns being most consistent with” rather than a definitive diagnosis. This approach is consistent with daily imaging practice. These possible limitations were, however, counteracted by strengths such as large sample size, inclusivity, and consistency of patient management strategies.
To our knowledge, ours is the largest study to characterize the frequency and pattern of the thoracic CT abnormalities in patients with AAV. Pulmonary involvement is frequent and among 140 patients with AAV who underwent a thoracic CT study, almost 80% have pulmonary abnormalities on thoracic CT. Central airway disease occurred exclusively with PR3-ANCA whereas ILD was mainly seen in MPO-ANCA with involvement relating to ANCA serotype. This difference in imaging appearances may reflect differences in pathogenesis, but this requires further study. Pulmonary involvement should, therefore, be considered in all patients at time of AAV diagnosis, and a heightened awareness of this manifestation is recommended to avoid underdiagnosis.
Footnotes
Supported by research grants from Governmental Funding of Clinical Research within the Faculty of Medicine, Lund University (ALF-medel), The Swedish Society of Medicine (Svenska Läkarsällskapet), and the UK National Institute for Health Research Cambridge Biomedical Research Centre.
- Accepted for publication May 17, 2017.








{kind=link}
{kind=link}