

Abstract
Objective. To rank outcomes identified as important to patients with psoriatic arthritis (PsA) and examine their representation in existing composite measures.
Methods. Seven nominal group technique (NGT) meetings took place at 4 hospital sites. Two sorting rounds were conducted to generate a shortlist of outcomes followed by a group discussion and final ranking. In the final ranking round, patients were given 15 points each and asked to rank their top 5 outcomes from the shortlist. The totals were summed across the 7 NGT groups and were presented as a percentage of the maximum possible priority score.
Results. Thirty-one patients took part: 16 men and 15 women; the mean age was 54 years (range 24–77; SD 12.2), the mean disease duration was 10.3 years (range 1–40; SD 9.2), and mean Health Assessment Questionnaire was 1.15 (range 0–2.63; SD 0.7). The highest-ranked outcomes that patients wished to see from treatment were pain with 93 points (20.0%), fatigue 62 (13.3%), physical fitness 33 (7.1%), halting/slowing damage 32 (6.9%), and quality of life/well-being 29 (6.2%). Reviewing existing composite measures for PsA demonstrated that no single measure adequately identifies all these outcomes.
Conclusion. Pain and fatigue were ranked as the outcomes most important to patients receiving treatment for PsA and are not well represented within existing composite measures. Future work will focus on validating composite measures modified to identify outcomes important to patients.
Psoriatic arthritis (PsA) is an inflammatory arthritis affecting up to 20% of people with psoriasis1. PsA is now well recognized to be progressive and destructive in the majority with considerable effect on quality of life, and there is growing evidence from observational studies that delayed diagnosis is associated with worse radiographic and functional outcomes2,3,4. This has prompted the hypothesis that early detection and treatment may improve outcomes in the long term for patients. The “early detection to imPRove OutcoMe in patients with undiagnosed Psoriatic arthriTis” (PROMPT) study is a program of studies that investigates the effect of enhanced surveillance for the early detection of arthritis among patients with psoriasis (RP-PG-1212-20007). An important aspect of our study was to assess outcomes that were meaningful to patients.
Considerable efforts have been made in recent years to improve the assessment of treatment response in PsA. Work within the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis (GRAPPA) and the Outcome measures in Rheumatology (OMERACT) led to the development of a core set of domains of disease to be assessed in randomized controlled trials (RCT) and longitudinal observational studies (LOS) in 20065, updated in 20166. There is, however, no consensus as yet on the optimal method for assessing treatment response7,8. It is well established that PsA may affect many domains including arthritis, enthesitis, dactylitis, spondylitis, uveitis, and other extraarticular manifestations such as the metabolic syndrome. There have been efforts to develop a composite outcome measure of disease activity to identify all aspects of PsA in a continuous activity measure. It is important to distinguish an activity measure from a response criteria such as the minimal disease activity9, Psoriatic Arthritis Response Criteria10,11, or the American College of Rheumatology12 criteria that define a disease state that is either achieved or not. A disease activity measure has the benefit of grading response and tracking of activity over time; further, cutpoints of high, moderate, and low disease activity and remission can be developed to derive a response criteria. An activity measure is also distinct from an effect of disease measure, such as the Psoriatic Arthritis Impact of Disease (PSAID), which more widely covers concepts of activities and participation.
Several candidate activity measures have now been developed including the Composite Psoriatic Arthritis Disease Activity Index (CPDAI)13, GRAPPA Composite Exercise (GRACE) measure, Psoriatic Arthritis Disease Activity Score (PASDAS)14, and Disease Activity in Psoriatic Arthritis (DAPSA)15. It has become apparent that these measures were developed with little patient involvement. This raises the issue that without representation of the lived experience of PsA through patient involvement we may be missing important aspects of disease and thereby calling into question the validity of the composites16.
As part of the PROMPT program, we set out to establish whether existing composite activity measures identify outcomes of treatment important to patients or whether modifications may be necessary. Any modified versions would need validation in a prospective study and shortened, more feasible versions should be derived (based on sensitivity to change) for use in routine care. The first stage previously reported was to identify which outcomes from treatment were thought important by patients in a UK multicenter focus group study17. Qualitative data identified many outcomes important to patients, ranging from specific physical symptoms to the psychological, social, and emotional effect on well-being and daily life. The objective of our present study was to rank these outcomes identified as important to patients and examine their representation in existing composite measures.
MATERIALS AND METHODS
Nominal group technique
A nominal group technique (NGT) was applied for patients to rank the previously identified outcomes by importance. An NGT is a structured group process with a focus on solution generation and decision making. It encourages contributions from all participants by asking each individual for their opinion and their vote in the ranking exercise. To ensure an appropriately wide range of views and experience, patients who took part in the initial focus group studies to identify domains17 were not eligible to take part in our present NGT ranking study.
Seven NGT groups took place at 4 hospital sites in Bristol, Bath, Stoke, and Weston. Patients were identified from routine clinic appointments by their treating physician. To be eligible to take part, patients had to be over 18 years old, have a physician diagnosis of PsA, and have sufficient English language to participate in discussions. Efforts were made to recruit a sample of patients with a spectrum of phenotype and activity.
Prior to the start of the nominal groups, patients were asked to complete data on demographics, medications, and a Health Assessment Questionnaire score (HAQ)18 as a measure of physical function. Nominal groups lasted for about 1 h, were cofacilitated by 2 members of the study team (ED and SH), and were audio-recorded to keep an audit trail of the process. The nominal groups began with patients individually sorting a pack of laminated cards listing the 68 outcomes from previous UK focus group studies17, as well as 5 additional outcomes generated from a concurrent international focus group study6. Data from both these focus group studies contributed to the updated OMERACT PsA core set of domains6. The questions asked in these focus group studies addressed the same themes, but exact wording differed.
UK focus groups were asked:
Which symptoms have the most effect on your well-being?
What do you want from your treatment?
What are the benefits and drawbacks of treatment for you personally?
How do you know when you are in a flare?
International focus groups were asked:
How does PsA affect your life?
Has your life changed since PsA?
How do you know you are in flare/remission?
In round 1 of the NGT, patients were asked to rank with the instruction: “What outcomes would you want from a treatment for your psoriatic arthritis?” Outcomes were categorized into 4 groups: not important/not applicable, important, very important, and most important. In round 2, patients then identified the top 5 of their “most important outcomes” and these were shared with the group, listed on a board and each one discussed and debated by the group, supported by facilitators. In round 3, patients were asked to individually rank the top outcomes from the group list and overall ranking scores were calculated. The 5 top outcomes scored 5 points down to 1 according to priority order. Points were then summed across all 7 nominal groups giving a potential total of 465 points. Data are represented as total points and percentage of the maximum possible score.
This study was approved by the National Research Ethics Service Committee North West-Haydock (reference: 15/NW/0609) and has been conducted in accordance with the Declaration of Helsinki. All participants signed informed consent.
Representation in existing composite measures
The final ranked outcomes from the NGT were then mapped against those included in the CPDAI, PASDAS, DAPSA, and GRACE by 1 investigator (WT). These data were then presented at an investigator’s meeting to (1) discuss how each outcome was represented in the existing composite measures, (2) identify the highest-ranked outcomes important to patients that were missing, and (3) discuss which instruments could be added to identify these important missing domains to modify composites. The PASDAS, which was derived through a regression analysis and therefore cannot be modified retrospectively, was included in our study for completeness. The CPDAI, GRACE, and DAPSA are modular and hence amenable to modification. At the mapping meeting, there were 3 patient research partners (MB, JJ, JL), 4 clinicians (WT, NM, OFG, PH), and 2 qualitative researchers (ED, SH).
The CPDAI13
The CPDAI measures disease activity in 5 domains: peripheral joints (68 tender and 66 swollen joints, and HAQ19), skin [Psoriasis Areas and Severity Index (PASI)20 and Dermatology Life Quality Index21], enthesitis (Leeds Enthesitis Count22 and HAQ), dactylitis (number of tender dactylitic digits and HAQ), and spine [Bath Ankylosing Spondylitis Disease Activity Score (BASDAI)23 and Ankylosing Spondylitis Quality of Life index (ASQoL)24]. Within each domain, severity is graded as 0 (none), 1 (mild), 2 (moderate), and 3 (severe), according to predefined cutoffs. The GRACE measure14. The GRACE measure is derived from the tender and swollen joint count, HAQ, patient’s global, skin and joint visual analog scale (VAS) scores, PASI, and Psoriatic Arthritis Quality of Life (PsAQoL). Scores are transformed into linear functions ranging from 0 (totally unacceptable state) to 1 (normal) based on established desirability functions14. The 8 transformed variables are then combined using the arithmetic mean giving a score from 0 to 1; the GRACE measure is a transformed version where scores range from 0 (low disease activity) to 10 (high disease activity).
The DAPSA15
The DAPSA is a measure derived from the 68 tender and 66 swollen joint count, C-reactive protein, patient’s global, and pain VAS.
The PASDAS14
The PASDAS is a weighted index consisting of assessments of joints, function, acute-phase response, quality of life, and patient’s and physician’s global by VAS.
RESULTS
Nominal group technique
Thirty-one patients took part in 7 nominal groups at 4 hospital sites. There was a total of 16 men and 15 women, the mean age was 54 years (range 24–77; SD 12.2), the mean disease duration was 10.3 years (range 1–40; SD 9.2), and mean HAQ was 1.15 (range 0–2.63; SD 0.7). Patients had current or previous disease activity in the following domains: peripheral arthritis (n = 29), psoriasis (27), spondyloarthritis (5), enthesitis (5), and uveitis (1). The 68 outcomes important to patients discussed in round 1 are listed in Table 1. The round 2 shortlists from each of the 7 NGT are reported in Table 2. The final ranking of outcomes important to patients from round 3 are listed in Table 3. The top 5 ranked outcomes from treatment were pain with 93 points (20.0%), fatigue 62 (13.3%), physical fitness 33 (7.1%), halting/slowing damage 32 (6.9%), and quality of life/well-being 29 (6.2%).
List of 68 outcomes for discussion and ranking in round 1 of the nominal group technique.
Individual group shortlists of important outcomes from round 2 of the nominal group technique.
Final ranking of outcomes important to patients in round 3 of the nominal group technique.
Representation of outcomes in existing composite measures
It was not feasible to examine the representation of all 68 outcomes in the composite measures (CPDAI, PASDAS, GRACE, DAPSA). Examining the data, there appeared to be a natural separation in the prioritization of the top 10 ranked outcomes as compared to those ranked as less important (Table 3). As a result, the top 10 ranked outcomes from the NGT were mapped to the composite measures and compared to the OMERACT core set of domains in Table 4. None of the existing composite measures identified all 10 priority outcomes. Discussion at the investigators’ meeting focused on the 2 modular composites, the CPDAI and GRACE, which are amenable to the addition of new outcomes. The top 10 outcomes from the NGT are mapped to the CPDAI and GRACE in Figure 1 and Figure 2, respectively. Pain (93 points) and fatigue (62 points) were ranked considerably more important by patients than the other outcomes in the NGT, and it is notable that neither pain nor fatigue are represented independently in the CPDAI or GRACE composite measures.
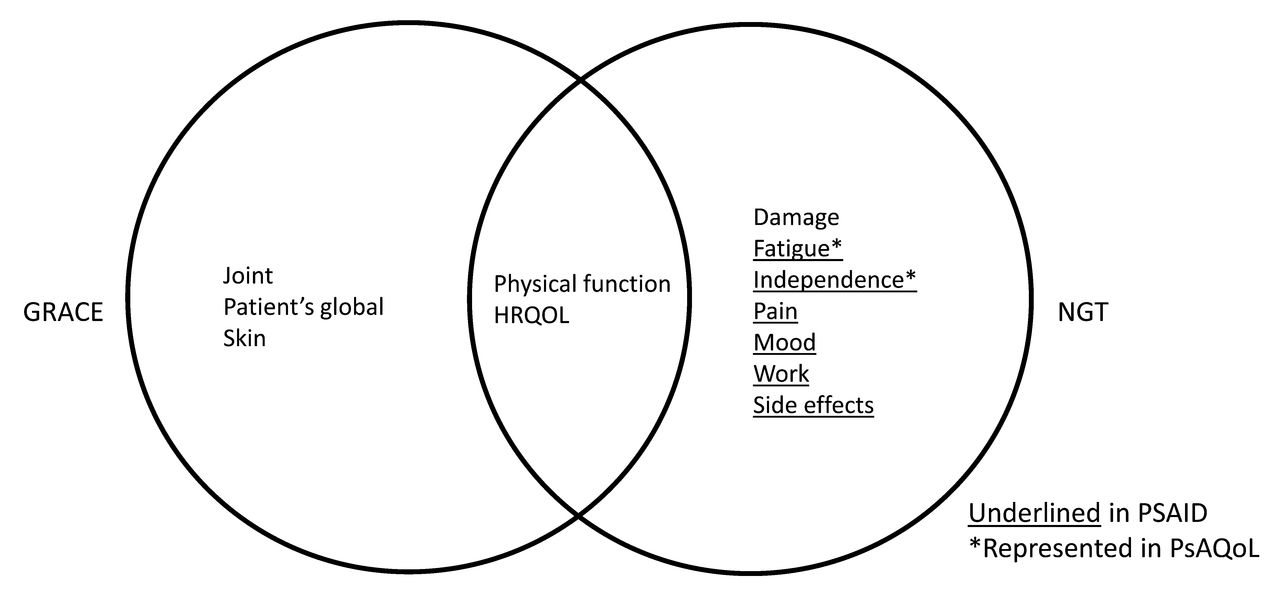
Representation of outcomes important to patients in the current NGT study and the GRACE measure. NGT: nominal group technique; GRACE: Group for Research and Assessment of Psoriasis and Psoriatic Arthritis Composite Exercise; HRQOL: health-related quality of life; PSAID: Psoriatic Arthritis Impact of Disease; PsAQoL: Psoriatic Arthritis Quality of Life.

Representation of outcomes important to patients in the current NGT study and the CPDAI measure. NGT: nominal group technique; CPDAI: Composite Psoriatic Arthritis Disease Activity Index; HRQOL: health-related quality of life; PSAID: Psoriatic Arthritis Impact of Disease; ASQoL: Ankylosing Spondylitis Quality of Life.
Map of the top 10 outcomes to the existing composite measures and updated OMERACT core set of domains.
The remaining 8 out of the top 10 outcomes identified in the NGT were then discussed. Physical function, quality of life, and fitness were considered identified within the HAQ, PsAQol, and ASQol. Damage is an important concept identified in the NGT and represented in the OMERACT core set of domains, but given the irreversible characteristic of damage, it was agreed that this was not suitable to include in an activity measure, rather it should be measured separately using a different instrument. Work, independence, and mood are not independently or well identified in the existing composite activity measures. Of interest, many of the outcomes not identified by the activity measures are reflected in the PSAID instrument that was developed as a measure of effect rather than activity (Figure 1 and Figure 2)25. Medication side effects are identified as adverse events in RCT, but not in LOS. The group recognized that it would not be feasible to add all outcomes into a modified composite measure and that pain and fatigue appeared clearly separate in the rankings from other outcomes. It was also noted that pain and fatigue were included in the OMERACT core domain set and therefore there was agreement that they should be represented in the composite measures in a planned validation study within the PROMPT program.
Potential measures for pain and fatigue were discussed. There are data supporting the use of the Functional Assessment of Chronic Illness Therapy Fatigue (FACIT-fatigue) patient-reported questionnaire for physical fatigue in PsA26. The PSAID instrument has fatigue and pain items (0–10), but the PSAID needs further validation as an activity measure25. A standard pain VAS 0–100 was also considered. It was agreed to include these measures in the prospective study and select the best performing measure (in sensitivity to change).
DISCUSSION
We report a multicenter study ranking outcomes important to patients and how they are represented in existing composite measures of disease activity in PsA. None of the composite scores in their existing form identify the top 10 outcomes important to patients identified in our study. Pain was ranked most highly by patients in our study and is not well represented in the existing composite measures. The DAPSA is the only composite to independently measure pain using a VAS. The CPDAI, GRACE, and PASDAS may identify pain indirectly, such as through the tender joint count, enthesitis/dactylitis counts, the patient’s global VAS score, or within a component questionnaire. For example, the CPDAI includes pain questions within the BASDAI23 and the ASQoL24. However, indirect measurement of an outcome in this way has disadvantages, such as the inability to perform specific analyses and reduced representation of an outcome within the overall score. The BASDAI, for example, is reported as a single score and not by its component parts, making separate analysis of pain difficult. Deterioration of other components within the BASDAI (such as stiffness or fatigue) may also mask improvement in another component, in this case pain. Indirect measurement in this way also diminishes the representation of pain within the total composite score. Pain (the most highly ranked outcome to patients in our study) is poorly represented in the CPDAI; as a subcomponent of the BASDAI, which is itself only 1 component of the CPDAI. Pain therefore contributes only a very small amount to the total CPDAI score, thereby affecting its face validity.
Fatigue was ranked second highest by patients, but similar to pain, is not well represented in composite measures. Fatigue is also represented indirectly in the CPDAI (in the BASDAI and ASQoL) and PASDAS (PsAQoL)27. The individual questions of the BASDAI, ASQoL, and PsAQoL are not designed to be separately reported and as a result fatigue cannot be easily studied independently. The same problem arises with independence which was ranked in the top 10 outcomes and is represented in PsAQoL and ASQoL, but not independently reported.
Skin disease was ranked as a low priority in our study, which is discordant with other qualitative studies of outcomes in PsA. The studies conducted for the development of the PSAID impact measure ranked skin symptoms as third highest behind pain and fatigue25. In an international study to update the PsA OMERACT core set, 24 focus groups were conducted to identify domains of PsA important for patients as part of the update of the OMERACT core set for PsA6. Skin psoriasis symptoms were ranked by patients as important, but as in our study, slightly lower than other outcomes (placed 17th out of 39 in the first Delphi round, and sixth out of 15 in the second round). The low ranking of skin symptoms in our study may reflect low levels of psoriasis among the cohort of patients in our study, but we did not specifically record participants’ levels of psoriasis activity before the focus groups. Regarding skin representation in the composite measures, skin activity is identified in the GRACE, PASDAS, and CPDAI, but not in the DAPSA measures.
We recognize that many of the outcomes important to patients in our study are identified in the PSAID impact measure. Outcomes identified as important to patients cover effect and activity, supporting the view that patients do not distinguish between the 2 concepts when describing the influence of the disease17. Only damage and treatment side effects are not included. The PSAID is a patient-reported questionnaire in 2 versions, 12 or 9 questions identifying aspects of PsA such as pain, fatigue, work, function, and participation. Therefore, should the PSAID be validated as a measure of disease activity as well as effect?
When interpreting the findings of our study, it is important to recognize that concurrent fibromyalgia (FM) or depression among study participants was not recorded for subanalysis. It is, therefore, not possible to determine the influence these comorbidities (or other contextual factors such as coping or self-management) have on the NGT rankings. In a recent study by Brikman, et al, concomitant FM was found to be associated with “worse” scores in all patient-reported, clinical, and composite PsA measures28. This is an important consideration when selecting (or modifying) a composite measure of disease activity where individual components of composite scores may be more susceptible to influence by contextual factors such as FM.
Composite activity measures are developed to identify all components of PsA disease activity, although component parts may be used to assess how individual aspects of disease are influenced by treatment. In a disease such as PsA with diverse manifestations, this is of considerable importance because, for example, a treatment may influence 1 domain, but not another. A well-constructed composite measure should, therefore, identify all domains of disease yet allow subanalysis of individual domains. Fatigue has been rated highly in our current study and now sits in the inner core of the recently updated OMERACT core set of domains6. Little is understood about the underlying cause of fatigue in PsA or the effect of treatment, in large part because fatigue is infrequently measured in RCT29. There is now an opportunity to incorporate pain and fatigue in a modified composite measure for PsA, either using the fatigue/pain VAS scores from the PSAID questionnaire or the FACIT-fatigue scale.
In our NGT study we ranked outcomes of treatment important to patients and examined their representation in existing composite outcome measures that have been developed without significant input from patients. The top 5 outcomes ranked by patients were pain with 93 points (20.0%), fatigue with 62 (13.3%), physical fitness 33 (7.1%), halting or slowing damage 32 (6.9%), and quality of life/well-being 29 (6.2%). Pain and fatigue were ranked most highly as outcomes important to patients and are not adequately identified within existing composite measures. Future work will focus on validating composite measures modified to identify outcomes important to patients.
APPENDIX 1.
List of study collaborators. The PROMPT Programme Management Group: Alison Nightingale, Helen Harris, Laura Coates, Catherine Fernandez, Sarah Brown, Claire Davies, Jonathan Packham, Laura Bjoke, Eldon Spackman, Catherine Smith, Anne Barton, Vishnu Madhok, Andrew Parkinson, and Gavin Shaddick.
Footnotes
This report is from independent research funded by the National Institute for Health Research (Programme Grants for Applied Research, Early detection to improve outcome in patients with undiagnosed psoriatic arthritis, RP-PG-1212-20007).
- Accepted for publication May 18, 2017.








{kind=link}
{kind=link}