

Abstract
Objective. To assess the efficacy and safety of the interleukin-1β (IL-1β) inhibitor canakinumab in all adolescent and adult patients with familial Mediterranean fever (FMF) identified from the Greek National Registry for off-label drug use between 2010 and 2015.
Methods. In this retrospective longitudinal outcome study, clinical and laboratory data were collected from 14 patients (7 men) aged median 38.5 years (range 13–70), with median disease duration of 14 years, and active FMF despite colchicine (n = 9) or both colchicine and anakinra (n = 5).
Results. All patients continued to receive canakinumab at last visit (median of 18 mos, range 13–53), which was initially given as monotherapy (n = 8) or in combination with colchicine and/or corticosteroids, every 4 (n = 7), 6 (n = 2), or 8 weeks (n = 5). Eleven patients (79%), including 6 receiving monotherapy, achieved complete clinical remission within 2 months (median), while normalization of all laboratory variables denoting inflammation occurred in 92% at 3 months (median). The remaining 3 patients achieved partial responses. Responses were sustained in all but 4 patients, who relapsed. Reducing the canakinumab administration interval from 8 or 6 weeks to 4 weeks led to suppression of disease activity in the relapsing patients. On the other hand, drug administration interval could be safely increased in 2 patients in remission. Corticosteroid doses were significantly reduced during followup. Canakinumab was well tolerated; 1 patient experienced a urinary tract infection and another one a viral gastroenteritis.
Conclusion. Treatment with canakinumab in an individualized dosing scheme results in rapid and sustained remission in colchicine-resistant FMF.
In recent years, advances in the understanding of the pathogenetic involvement of proinflammatory cytokines in familial Mediterranean fever (FMF), including excessive interleukin 1 (IL-1) activity because of inflammasome activation1,2, has opened a new, promising horizon in the treatment of these patients. Along this line, administration of the IL-1β inhibitor canakinumab, a human monoclonal antibody approved for use in cryopyrin-associated periodic syndromes, systemic juvenile idiopathic arthritis, and gout, seems to be a sound approach for patients with FMF refractory to colchicine3,4. Herein, we sought to describe the efficacy and safety of canakinumab in all adolescent and adult patients with FMF who started this treatment between 2010 and 2015 in our country.
MATERIALS AND METHODS
Patients
All adolescent and adult Greek patients with FMF for whom canakinumab was prescribed between January 2010 and January 2015 were identified from the files of the national drug association for off-label drug use. In total, there were 14 patients diagnosed and followed in 8 different medical centers in Greece. Information was initially retrieved retrospectively from the patient medical records and prospectively after January 2015. All patients fulfilled the Tel Hashomer criteria for a definite or probable diagnosis of FMF5 and all had, except for 1, at least 1 mutation in the MEFV gene6. Testing for other hereditary recurrent fevers revealed negative results in the TNFRSF1A, MVK, and CIAS1/NALP3/PYPAF1 genes in all patients7. Active disease resistant to colchicine (n = 9) or both colchicine and anakinra (n = 5) was the reason for canakinumab treatment, while 1 patient had also been treated with methotrexate, azathioprine, and infliximab in the past. Colchicine was discontinued in 7 patients at canakinumab initiation because of drug tolerance issues (mild diarrhea, n = 5; myalgias, n = 1; leukopenia, n = 1). In another 2 patients, the physician decided to discontinue colchicine at the time of initiating canakinumab because of its inefficacy. Canakinumab 150 mg subcutaneously was initially given every 4 (n = 7), 6 (n = 2), or 8 weeks (n = 5), because of logistic reasons, either as monotherapy (n = 8) or in combination with colchicine 1–2 mg/day (n = 5) and/or oral methylprednisolone (n = 5).
Clinical and laboratory data were recorded at treatment onset, 1, 3, 6, 12 months, and at last visit. After the relevant information was collected, each patient was contacted to have a final evaluation, performed for all cases by the same physician. Using the information retrieved from both the medical charts and the oral evaluation, the exact timepoints of partial and complete response as well as relapse were determined. Calculated for each patient were the FMF50, defined as at least a 50% improvement score of disease response8 and the visual analog scale (VAS) for the assessment of global patient well-being as well as VAS physician’s score (physician’s assessment of disease activity). Moreover, drug-related adverse events were recorded. The study was approved by the Laikon University Hospital scientific and ethics committee (#213-14) and each patient provided written informed consent to his/her responsible physician according to the Declaration of Helsinki.
Definitions
Active disease was considered as the presence of at least 1 disease-related symptom within the last month. Colchicine resistance was defined as active disease despite at least 3 months of treatment with colchicine. Complete response, clinical (CCR) or laboratory (CLR), was defined as the complete resolution of all disease-related symptoms. Partial clinical response (PCR) and partial laboratory response (PLR) were defined as improvement (of at least 30% for laboratory variables) in 1 or more related clinical or laboratory manifestations, respectively, but without complete resolution of disease activity. Relapse was defined as a worsening (of at least 30% for laboratory variables) in 1 or more related clinical and/or laboratory manifestations.
Statistical analysis
Patient characteristics were compared during followup using repeated measures mixed-model analysis in means of linear and generalized linear models. Results were considered significant with p value of 0.05 or less. Analyses were conducted in SPSS version 22. All p values are 2-tailed.
RESULTS
The patient characteristics at baseline and during followup are shown in Table 1, Figure 1, and Figure 2. The median patient age was 38.5 years (range 13–70 yrs). The median disease duration until canakinumab initiation was 14 years (range 7–37 yrs). All patients continued to receive canakinumab at last visit (median of 18 mos, range 13–53 mos). The median (range) duration of retrospective and prospective followup was 8 months (3–40 mos) and 10.5 months (10–13 mos), respectively.

Percentage of patients presenting the different clinical manifestations during followup. A. Fever (p value of the generalized linear model is 0.029). B. Joint involvement (p = 0.010). C. GI involvement (p = 0.030). D. Myalgias (p = 0.032). E. Serositis (p = 0.214). F. Exertional leg pain (p = 0.290). The percentages of patients with arthralgias and arthritis were 93% and 21%, respectively, at baseline, 57% and 21% at 1 month, 43% and 7% at 3 months, 36% and 7% at 6 months, 29% and 0% at 12 months, and 17% and 8% at last visit. GI: gastrointestinal.
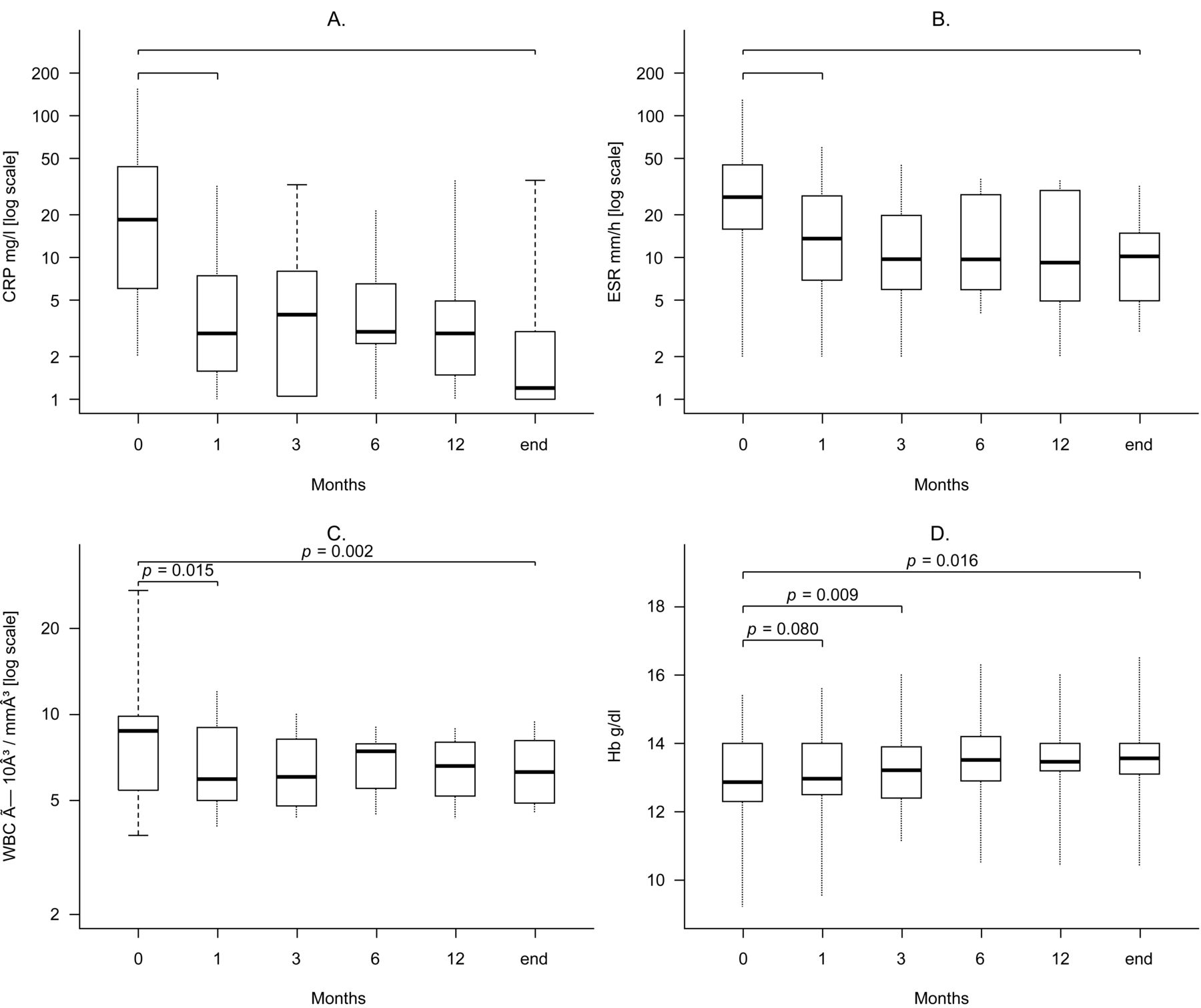
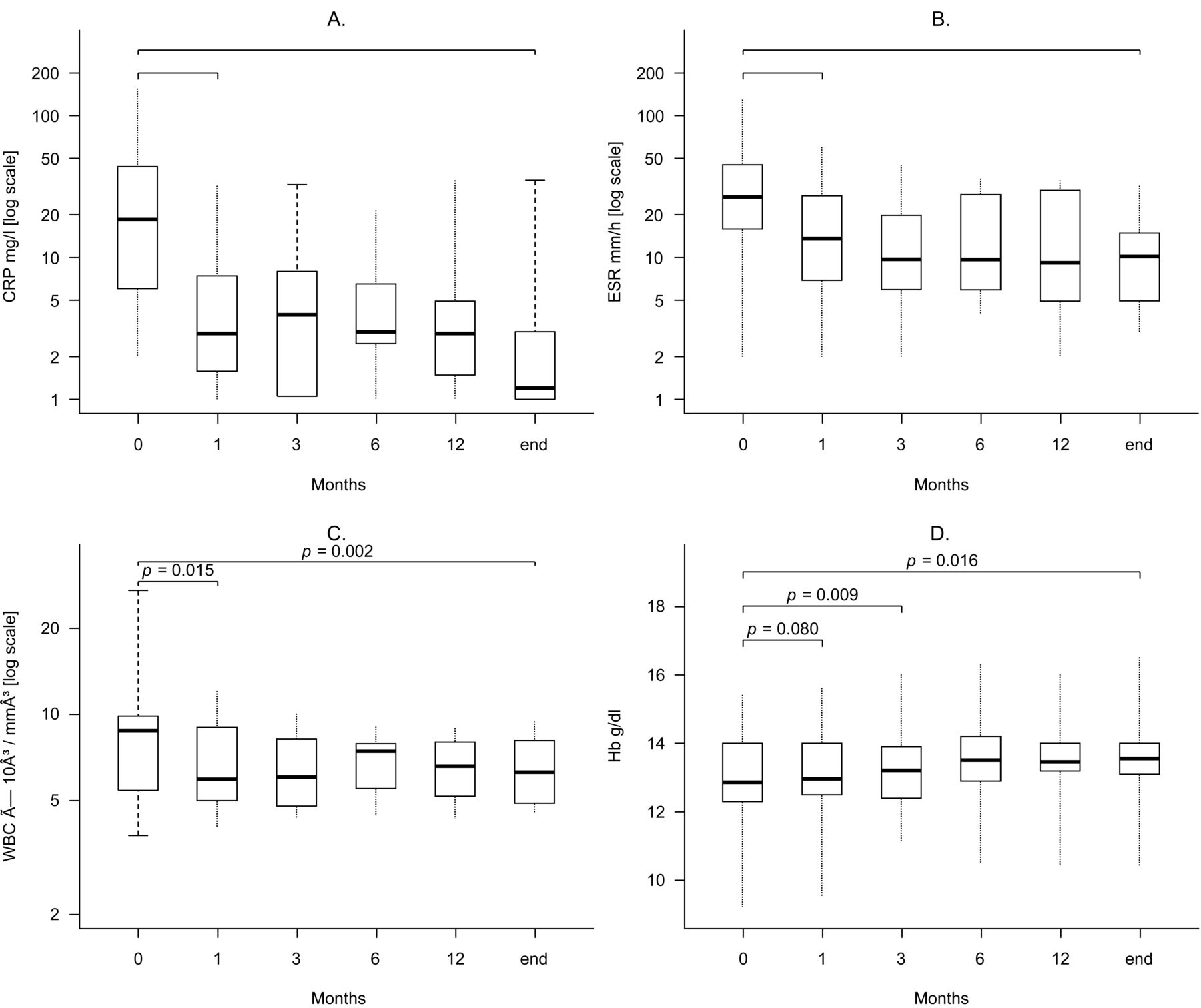
Laboratory variables during followup. A. CRP (p value of the mixed linear model is < 0.001). B. ESR (p = 0.009). C. WBC (p = 0.023). D. Hb (p = 0.046). The bottom and the top of the boxes show the first and third quartiles, and the band inside each box shows the second quartile (median). The ends of the whiskers represent minimum and maximum values. CRP: C-reactive protein; ESR: erythrocyte sedimentation rate; WBC: white blood cells; Hb: hemoglobin.
Patient characteristics and outcome.
Response
As shown in Figure 1 and Figure 2, most investigated variables improved within the first month of treatment and at each evaluation during followup compared with baseline (p values not shown). All patients showed a response to treatment. In 11 (79%) of the 14 patients, including 6 patients receiving monotherapy, clinical activity resolved completely, while the remaining 3 patients (21%) had a partial response and presented arthralgias (n = 2), abdominal pain (n = 1), exertional leg pain (n = 2), and/or testicular pain (n = 1; Table 1). In all patients with CCR and 2 of the patients in PCR, laboratory variables were normal. CCR was achieved within 1–12 months from the initiation of treatment and the median time was 2 months, whereas the median time to PCR was 1.5 months (range 1–3 mos). In 10 (91%) of the 11 patients, laboratory variables returned to normal; 1 patient (9%) showed a partial response with elevated C-reactive protein (CRP) levels and erythrocyte sedimentation rate (ESR; Table 1). Disease was clinically silent in all but 2 patients with CLR (Table 1). A complete response of all biological disease-related symptoms occurred within a median survival time of 3 months (range 1–16 mos), whereas a partial improvement in laboratory variables was observed within the first month of treatment in the 1 patient with PLR.
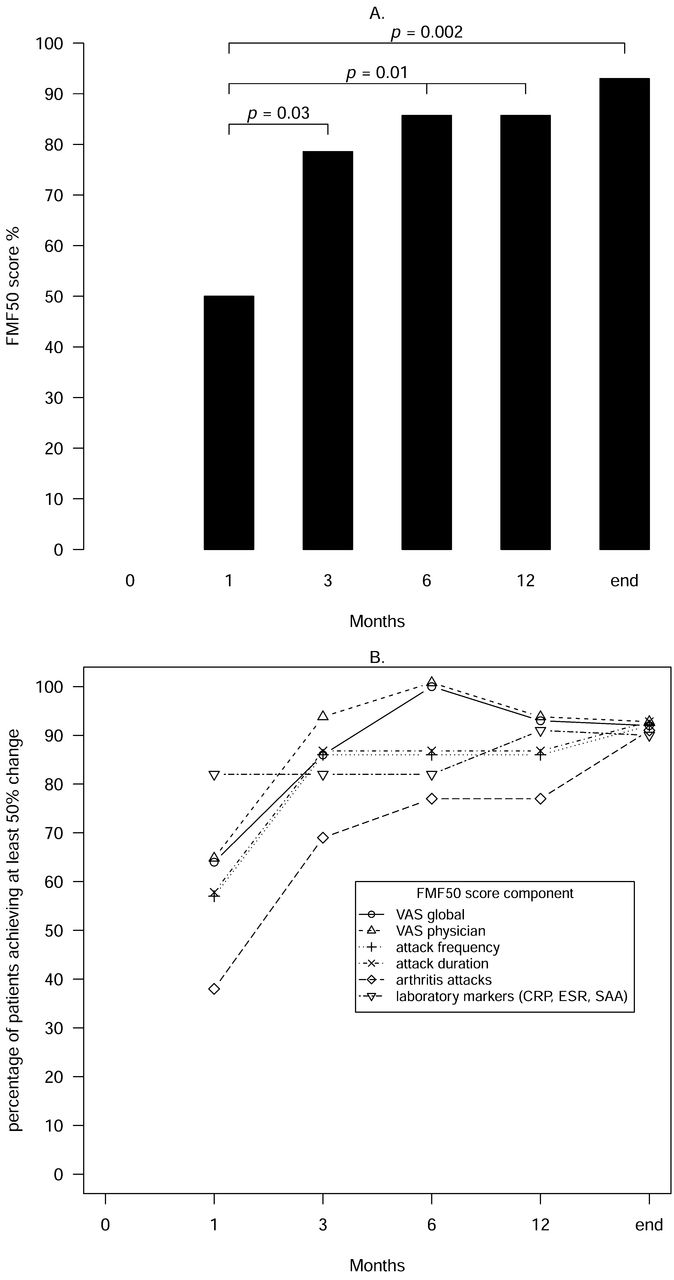
The percentage of patients achieving the FMF50 score was 50% at 1 month and increased to 86% at 1 year (p = 0.01) and 93% at the latest visit (p = 0.002; Figure 3).

FMF50 score during followup. A. Percentage of patients achieving the FMF50 score during followup (p = 0.030). B. Percentage of patients achieving the different components of the FMF50 score during followup (at least 50% improvement in the frequency of disease attacks, p = 0.060; duration of attacks, p = 0.060; arthritis attacks, p = 0.016; laboratory markers, p = 0.070; VAS global scores, p = 0.030; and VAS physician scores, p = 0.030). FMF50: familial Mediterranean fever score defined as at least 50% disease improvement; VAS: visual analog scale; CRP: C-reactive protein; ESR: erythrocyte sedimentation rate; SAA: serum amyloid A.
A significant decrease in VAS patient and physician scores was demonstrated within the first month of treatment (median 2.3 vs 8.8 and 2.0 vs 6.5, respectively, both p = 0.001) and was maintained until the latest visit (median 1.0 vs 8.8 and 1.0 vs 6.5, respectively, both p = 0.004).
Relapse
During followup, disease exacerbations occurred in 4 patients (29%). One patient in the PCR and PLR groups developed a self-limited, erysipelas-like erythema at 9 months of treatment. At 21 months of treatment, anemia persisted and inflammatory markers (CRP, ESR) increased further; his arthralgias and enthesitis deteriorated and fever episodes lasting 3 days every week developed (Patient 2, Table 1). In another patient in CCR and CLR for 14 months, fever reappeared (Patient 4, Table 1). A third patient, in complete remission of all disease-related manifestations for 8 months, presented fever and arthralgias (Patient 5, Table 1). The fourth patient in CCR for 10 months and CLR for 12 months, relapsed with arthralgias, maculopapular rash, and a slight increase in ESR and CRP levels (Patient 14, Table 1).
Alterations in the canakinumab administration interval during followup
The canakinumab administration interval was reduced from 8 to 6 weeks in 2 relapsing patients (Patients 4 and 5, Table 1) and both went into complete disease remission. In the 2 other patients with relapse (Patients 2 and 14, Table 1), the administration interval was shortened from 8 to 4 weeks. Patient 2 had a partial clinical response within the last 3 months of followup. The fever remitted, arthralgias became milder, and anemia was corrected, but there was no change in inflammatory markers. The simultaneous increase in the daily colchicine dose to 1.5 mg caused diarrhea. Patient 14 went into complete remission again. In another patient with persisting clinical and laboratory activity at 4 months (Patient 13, Table 1), the shortening of the drug administration interval from 8 to 4 weeks completely suppressed disease activity.
Two patients increased the interval between the canakinumab injections without complications. The first patient, being in CLR and PCR at 6 months of treatment, increased the drug administration interval from 4 to 6 weeks and went into complete disease remission with resolution of her arthralgias within the next 3 months. After another 3 months, the drug could be safely administered every 8 weeks (Patient 3, Table 1). The other patient increased the canakinumab administration interval from 6 to 8 weeks after 12 months of treatment (11 mos in remission; Patient 10, Table 1).
Concomitant treatment
Colchicine was administered as adjunct therapy at 1 mg/day (n = 4) or 2 mg/day (n = 1) during the whole followup in 5 patients. The mean oral methylprednisolone dose at baseline was 5.9 mg/day (range 0–32 mg/day) and was tapered in all patients until the end of followup.
Adverse events
One patient developed a lower urinary tract infection at 4 months of treatment, which resolved with antibiotics, and another had viral gastroenteritis at 18 months, which required short-term hospitalization.
DISCUSSION
In our present study, we assessed the efficacy and safety of the IL-1β inhibitor canakinumab in all adolescent and adult Greek patients with colchicine-resistant FMF (crFMF) who initiated treatment during a 5-year period. We note that genetic testing in the MEFV gene revealed only variants of uncertain significance such as R202Q or E148Q in 4 patients, whereas no variant was detected in 1 patient7. In these patients, the diagnosis relied on the clinical Tel Hashomer criteria, while a negative test for other hereditary recurrent fevers made a diagnosis other than FMF unlikely. Besides, the presence of rare undetected variants cannot be excluded7. Interestingly, it has been previously shown that the most frequent genotype in adult Greeks with typical FMF clinical picture is E148Q heterozygosity9. Moreover, the rate of homozygous mutation types (M694V or R202Q) was 97% among all compound homozygous mutation types in the Southeastern Mediterranean region of Turkey10. To our knowledge, ours is the largest series of crFMF treated with canakinumab reported in literature, because previous reports consisted of smaller patient series as well as case reports11–20,21.
All our patients continued to receive canakinumab until the last visit. A dramatic improvement in most disease-related manifestations, even severe such as aseptic peritonitis and meningitis, was evident from the first month of treatment. In particular, complete resolution of clinical symptoms occurred in 79% of patients within the first 2 months and was followed by normalization of acute-phase reactants and hematological variables within the first 3 months in 91% of patients. The rest of the patients showed partial responses. In recently published series of 9, 9, and 8 patients, respectively, a reduction in the frequency of attacks was observed in all patients11,15,17. The observation time in these studies was often shorter than a year, whereas the study by Eroglu, et al11 included both children and adolescents. Laboratory variables also normalized in the majority of the already published cases11,19,20. According to the available literature, the time to both clinical and serological response varied from a few days after the first injection up to 3 months of treatment11–20,21. Regarding the FMF50 score, a high percentage of patients, 93% in our cohort versus 100% in the study by Eroglu, et al11, achieved a response at last visit. At the same time, canakinumab had a positive effect on health-related quality of life measures, in line with previous reports11,13,15.
Relapses under canakinumab have been reported11,15,17. In our present study, the effect of canakinumab treatment was sustained until the latest visit in all but 3 complete responders. The fourth patient who experienced a disease flare was in partial response. We observed a slightly higher relapse rate of 29% compared with 22% in the study by Eroglu, et al11, and a lower one compared to other reports (44% and 50%)15,17. However, studies with a large number of patients and a long period of followup are still pending.
Regarding toxicity, canakinumab was safe and well tolerated by our patients. Only 1 severe gastrointestinal infection occurred, which remitted after hospitalization. We did not observe upper or lower respiratory system infections, headache, or local reactions to injections as reported in literature2,11,15,16, and none of the patients discontinued therapy because of adverse drug reactions.
Regarding the optimal scheme and duration of canakinumab treatment, there is no consensus yet. Canakinumab is usually given at the dose of 150 mg per injection, but the administration interval varies from 4 to 8 weeks11–20,21. In addition, in some cases, canakinumab has been administered for a limited time to treat an episode of FMF13,14,15,16, and in other series, including our present study, regularly to prevent disease recurrence17,19,20. In our hands, canakinumab was efficient even if initially administered every 8 weeks. Gradual reduction of canakinumab dosing seemed to be safe in 2 of our patients in remission. On the other hand, the shortening of interval between injections was efficient in controlling recurrent or persisting disease activity. Based on the current data, we suggest starting canakinumab every 8 weeks and shortening the interval between injections if disease activity persists, and increasing the interval in quiescent disease. Another interesting yet unanswered issue is whether the use of canakinumab in combination with colchicine improves its efficacy. Our study provides evidence that canakinumab monotherapy may be an effective therapeutic option, whereas combination with colchicine may be necessary when residual or recurrent disease activity is present20. However, the published recommendations for the practical management of FMF suggest the continuation of colchicine for as long as possible with anti-IL-1 medication for the prevention of secondary amyloidosis22. Further studies may give answers to these important issues.
Another highlighting point of our present study is the good efficacy of canakinumab in 5 anakinra-resistant cases. All of these patients went into complete disease remission. On the other hand, 3 of the 4 relapsing patients had been previously treated with the IL-1 blocker anakinra. Whether canakinumab has a better efficacy compared with anakinra remains to be tested. There is no randomized trial comparing the 2 drugs; however, efficacy of canakinumab in anakinra-resistant cases has also been previously reported11,12,13,14,18,20, while to our knowledge, the opposite has not been tested yet. Compared with the other IL-1 blockers, canakinumab has some differences. Unlike anakinra and rilonacept, which block the signals of both the IL-1α and IL-1β isoforms, it is highly specific for IL-1β, elevated in disease, and does not interfere with other IL-1–activated pathways. Because of its long half-life (26 days), there is no need for frequent injections. Indeed, safety data point toward a better cutaneous tolerance compared with anakinra16. Moreover, it should be considered when compliance problems are encountered. Nevertheless, canakinumab has not been tested in amyloidosis and endstage renal disease19,23,24. Whether long-lasting drugs should be used as a first-line treatment or only after having confirmed intolerance, inefficacy or even clinical benefit of silencing the IL-1 pathway with short-acting drugs needs to be discussed22. Future randomized trials will provide more information on these efficacy and safety drug issues.
Our results support the important involvement of IL-1 in the pathophysiological processes underlying FMF. Indeed, Kuijk, et al observed a reduction in serum IL-1α, IL-1β, and IL-18 after IL-1 blocking with anakinra25. Omenetti, et al26 showed that IL-1 secretion increased with both the number and penetrance of mutations, confirming the studies showing increased requirement of colchicine dosage and unresponsiveness in patients with homozygous M694V27 and supporting the possible better efficacy of IL-1 blockade in those patients. However, partial responders and nonresponders might suggest disease subtype heterogeneity and likely reflect different involvement of cytokines and pathological processes in these patients.
Finally, our results should be interpreted in the context of potential limitations. Our present study is a retrospective longitudinal outcome study. The colchicine dosage was not fixed and the decision on the administration of steroids was based on the physician’s judgment. Our patients had various MEFV gene mutations, which is a limitation to generalize our results to other patients with FMF. Moreover, the relatively small number of patients does not allow drawing definite conclusions on a better efficacy of canakinumab as adjunct to colchicine versus monotherapy or in colchicine only versus anakinra-resistant cases. Nevertheless, strengths of our study include the largest, until now, patient series, the longterm followup of at least 1 year, the evaluation of different dosing schemes, and the positive experience in anakinra-resistant cases.
Canakinumab, administered in an individualized dosing scheme, results in rapid and sustained remission in crFMF. Its efficacy together with the favorable safety profile encourages further use of canakinumab in adolescents and adults with FMF refractory to colchicine and/or anakinra.
Footnotes
Supported in part by ELKE grant 917, National and Kapodistrian University of Athens.
- Accepted for publication October 9, 2016.








{kind=link}
{kind=link}
{kind=link}