

Abstract
Objective. To study the effect of the presence of fibromyalgia (FM) on common clinical disease activity indices in patients with psoriatic arthritis (PsA).
Methods. Seventy-three consecutive outpatients with PsA (mean age 51.7 yrs; 42 females, 57.5%) were enrolled in a prospective cross-sectional study. FM was determined according to American College of Rheumatism criteria (2010 and 1990). All patients underwent clinical evaluation of disease activity and completed the Health Assessment Questionnaire (HAQ), the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), the Dermatology Life Quality Index, and the Leeds Enthesitis Index (LEI). Disease activity was evaluated using the Composite Psoriatic Disease Activity Index (CPDAI), minimal disease activity (MDA), and the Disease Activity Index for Psoriatic Arthritis (DAPSA) scores.
Results. The overall prevalence of FM was 17.8% (13 patients), and all but 1 were women (12 patients, 92.3%, p = 0.005). CPDAI and DAPSA scores were significantly higher in patients with coexisting PsA and FM (9.23 ± 1.92 and 27.53 ± 19.23, respectively) than in patients with PsA only (4.25 ± 3.14 and 12.82 ± 12.71, respectively; p < 0.001 and p = 0.003). None of the patients with FM + PsA met the criteria for MDA, whereas 26 PsA-only patients did (43.3%, p = 0.003). HAQ, BASDAI, and LEI scores were significantly worse in patients with PsA and associated FM.
Conclusion. Coexisting FM is related to worse scores on all tested measures in patients with PsA. Its influence should be taken into consideration in the treatment algorithm to avoid unnecessary upgrading of treatment.
Psoriatic arthritis (PsA) is a chronic inflammatory disease that involves peripheral and axial joints, tendons, and entheses. It is present in up to 30% of patients with psoriasis1,2,3.
The recent availability of highly effective biological therapies has led to the clinical use of several indices to more accurately evaluate the disease activity and the response to treatment. The use of disease activity scores is well established in rheumatoid arthritis (RA) and it is the basis of the treat-to-target approach4. Similar recommendations based on the treat-to-target approach in spondyloarthritis (SpA) have been published5. However, the clinical evaluation of PsA is much more complex and includes numerous domains of disease activity. The most commonly used indices in the evaluation of PsA activity are as follows:
Composite Psoriatic Disease Activity Index (CPDAI)
Disease involvement is assessed in up to 5 domains: peripheral arthritis, skin, enthesitis, dactylitis, and spinal manifestations. Domains are scored from 0 to 3, and the scores are summed to give an overall composite score (range 0–15). The CPDAI has been validated in a large clinical trial dataset of Psoriasis Randomized Etanercept Study in Subjects with Psoriatic Arthritis (PRESTA)6,7.
Minimal Disease Activity (MDA)
Disease activity is evaluated to define disease remission or a low disease activity state. For a patient to achieve MDA, 5 of the following 7 criteria must be met: tender joint count (TJC) ≤ 1, swollen joint count (SJC) ≤ 1, Psoriasis Activity and Severity Index (PASI)8 ≤ 1 or body surface area ≤ 3, patient pain visual analog score (VAS) ≤ 15, patient global disease activity VAS ≤ 20, Health Assessment Questionnaire (HAQ) ≤ 0.5, and tender entheseal points ≤ 1. The MDA criteria have been validated in an observational cohort and infliximab study of PsA9,10 and used as the main target in the TICOPA study11,12.
Disease Activity Index for Psoriatic Arthritis (DAPSA) scores
This score comprises 68 TJC and 66 SJC, patient global pain, and C-reactive protein (CRP) level. The composite score is a simple sum of the scores and does not include skin assessment. The DAPSA score has been validated in a large clinical dataset of Infliximab Multinational Psoriatic Arthritis Controlled Trial (IMPACT 2)6,13.
Disease Activity Score of 28 joints (DAS28)14
This score was originally developed and is clinically used for RA. It integrates the activity score (swollen or tender) in 28 joints, CRP levels, and a VAS of disease activity for calculating the score based on a formula. The DAS28 score was reported to be useful for assessing arthritis in PsA clinical trials15.
Fibromyalgia (FM) is a complex chronic pain condition that affects about 2% of the adult population16. It is more prevalent in women than in men (3.4% and 0.5%, respectively)17. The chronic widespread pain is accompanied by many other symptoms, such as fatigue, headaches, irritable bowel syndrome, sleep alterations, depression, anxiety, and others18.
A previous study has reported the frequency of 10 or more tender points in patients with PsA to be 24%19. More recent data have shown an estimated prevalence of FM in patients with PsA of 16%–18%20,21. The presence of FM adds physical and mental burdens to patients with PsA22; however, it is not clear how the presence of FM may affect the evaluation of disease activity in PsA20,21,22,23 and the subsequent effect on patient management.
In our study, we investigated the effect of the presence of FM on common clinical disease activity indices in patients with PsA.
MATERIALS AND METHODS
Patients
A prospective cross-sectional study was conducted in our institution between February 2013 and October 2014. A total of 73 consecutive patients with PsA attending the outpatient clinic of the Department of Rheumatology at Tel Aviv Medical Center were evaluated. To be included in the study, the patients had to meet the Classification Criteria for Psoriatic Arthritis (CASPAR) criteria24. Exclusion criteria consisted of refusal to sign the written informed consent, and clinical or laboratory evidence of active infection.
Measurements
The study patients were evaluated during a single visit according to the following steps: First, they were interviewed for their sociodemographic data (age and sex) and disease duration. Next, they completed the HAQ for functional status, the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), and the Dermatology Life Quality Index (DLQI). Pain and patient’s global assessment of disease activity were measured using 1–100 VAS scales. Third, a trained doctor who was unaware of the previously collected data (demographics, questionnaires) performed a comprehensive physical examination of the subjects’ musculoskeletal system, in which several domains of PsA were recorded.
A total of 68 TJC/66 SJC were carried out for peripheral joint activity, and 73 patients responded to the PASI for skin disease, the Leeds Enthesitis Index (LEI), the Maastricht Ankylosing Spondylitis Enthesitis Score (MASES), and the Leeds Dactylitis Index (LDI)6,7,8,9,13,14,15. CRP (mg/dl) was measured using samples collected within 10 days of the evaluation visit.
Evaluation for the presence of FM was based on the 2010 American College of Rheumatism (ACR) criteria by recording the widespread pain index and the symptom severity (SS) scale25,26,27. The patients were also examined for the presence of pain in 18 FM tender points as recommended by the 1990 ACR criteria. Cases were considered positive for FM in the presence of at least 1 criterion.
Statistical analysis
All of the data were entered into a Microsoft Excel database and analyzed using SPSS for Windows, version 18.0. The variable scores of the group with FM and the group without FM were compared: The association between categorical variables was tested using Pearson’s chi-squared test or Fisher’s exact test. Quantitative variables were graphically and statistically tested with the Kolmogorov-Smirnov goodness-of-fit test for normality of distribution. Variables with a normal distribution were presented as the mean ± SD, and the between-group comparisons were performed using the Student’s t test. Non-normal quantitative variables were presented as the median (25th and 75th percentiles), and the between-group comparisons were performed using the Mann-Whitney U test. Values ≤ 0.05 were considered statistically significant (all the presented p values are 2-tailed). A multivariable linear regression model was built to evaluate the association of the presence of FM with the CPDAI, DAPSA, and DAS28 scores, adjusting for confounding variables.
RESULTS
The study population was composed of 31 men (42.5%) and 42 women (57.5%), with a mean age of 51.7 ± 13.5 years, and a mean disease duration before study entry of 10.3 ± 7.5 years. Thirteen of the 73 patients with PsA (17.8%) fulfilled the criteria for the diagnosis of FM. Twelve patients were positive for FM according to the 2010 ACR criteria whereas 6 patients complied with the 11/18 tender points of the 1990 criteria (only 1 patient was positive for the 1990 criteria but did not comply with the 2010 criteria; only 2 patients had < 7 tender points on their physical examination for FM tender points). Most of the patients with PsA and FM were women (12 patients, 92.3%, p = 0.005), resulting in a prevalence of FM among women with PsA of 28.6%. The demographic and clinical characteristics of patients with and without FM are shown in Table 1. There was no significant difference in mean age or disease duration between the groups.
Demographic and clinical characteristics of psoriatic arthritis patients with and without fibromyalgia.
Disease activity indices
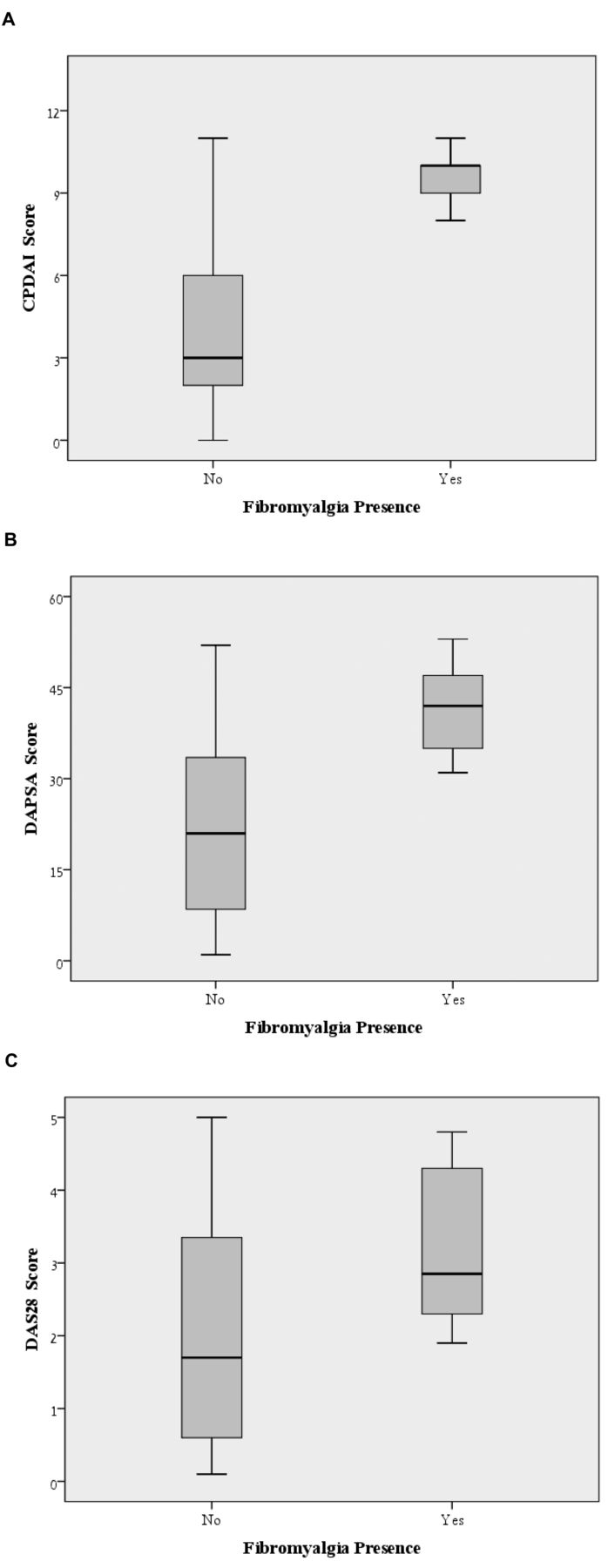
The CPDAI was 4.98 points higher in the group with PsA and FM compared with the PsA-only group (95% CI 3.17–6.8; p < 0.001). Likewise, the DAPSA was 14.71 points higher in the PsA and FM group (95% CI 5.09–24.33; p = 0.003). Further, the DAS28-CRP was 0.9 points higher in the FM group (95% CI 0.1–1.69; p = 0.027; Figure 1).
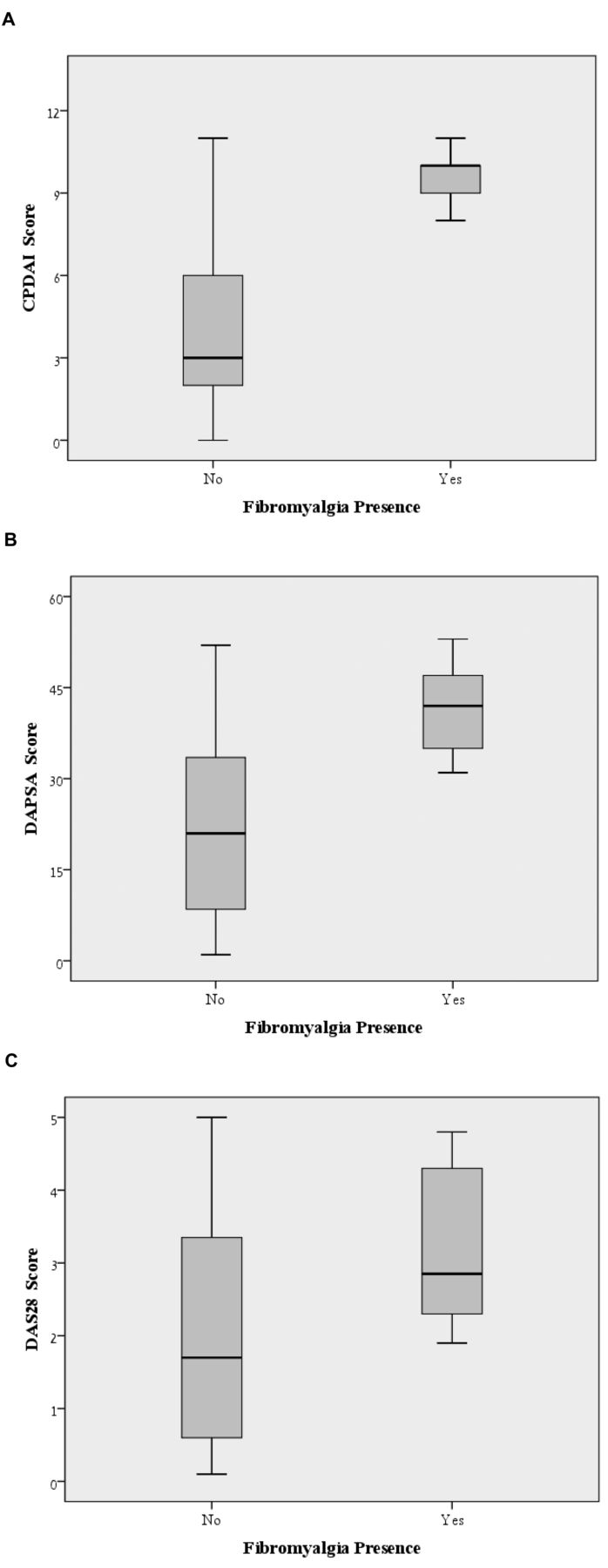
Plot of the CPDAI, DAPSA, and DAS28 scores of PsA patients with fibromyalgia (FM) and without FM. Boxes show median values (horizontal line) and 25th and 75th percentiles. Whiskers represent maximum and minimum values excluding outliers and extremes. A. The CPDAI median value was 10 (8.5–10*) for the group with PsA and FM compared to the PsA-only group, with CPDAI median of 3 (2–6*); p < 0.001. B. The DAPSA median value was 22.4 (16.5–30.6*) for the group with PsA and FM compared to the PsA-only group with DAPSA median of 10 (3–16.9*); p = 0.003. C. The DAS28 median value was 3 (2.6–4.2*) for the group with PsA and FM compared to the PsA-only group with DAS28 median of 1.5 (2.3–3.3*); p < 0.027. *25th to 75th percentiles. CPDAI: Composite Psoriatic Disease Activity Index; DAPSA: Disease Activity Index for Psoriatic Arthritis; DAS28: 28-joint Disease Activity Score; PsA: psoriatic arthritis.
None of the patients with PsA and FM met the criteria of minimal disease activity (MDA), whereas 26 PsA-only patients did (43.3%, p = 0.003). Moreover, patients with PsA who had associated FM had a significantly lower likelihood of achieving MDA (relative risk = 0.57, 95% CI 0.45–0.71; p < 0.0001).
HAQ, BASDAI, and LEI scores were significantly worse in patients with coexisting PsA and FM, but there were no significant differences between the groups in their CRP levels, PASI scores, and SJC. Table 2 provides a summary of the statistics for disease activity of the patients and for laboratory characteristics.
Common clinical disease activity indices in psoriatic arthritis patients with and without fibromyalgia.
The CPDAI, DAPSA, and MDA findings were calculated and compared by 3 additional points of reference: sex, disease duration (Group A = disease duration greater than the median duration of 9 years, and Group B = disease duration shorter or equal to the median duration of 9 years), and age (Group A = older than the median age of 52 years and Group B = younger or equal to the median age; Table 3). The CPDAI score was 2.16 points higher for the women (95% CI 0.53–3.79, p = 0.01). There was no other significant difference between the groups. The CPDAI, DAPSA, and MDA were also calculated and compared in the group of women to further explore the effect of sex. The results exhibited a similar trend as that in the combined study sample (Table 4). Finally, a model of multivariable linear regression with the CPDAI, DAPSA, and DAS28 scores is shown in Table 5. The results from this model indicated that FM presence is an independent predictor of worse scores on CPDAI, DAPSA, and DAS28 indices. CRP (mg/dl) and SJC, as expected, had significant correlations with CPDAI, DAPSA, and DAS28 indices. Sex as well as age had no significant correlations.
Comparison of common clinical disease activity indices in patients with psoriatic arthritis (PsA), according to sex, disease duration, and age.
Common clinical disease activity indices in female psoriatic arthritis patients with and without fibromyalgia.
Multivariable linear regression model with the CPDAI, DAPSA, and DAS28 scores as the dependent variable.
DISCUSSION
Our search of the literature failed to reveal any earlier published investigation of the direct effect of the presence of FM on commonly used clinical disease activity indices in patients with PsA. We assessed 73 patients with PsA for the coexistence of both conditions and the overall prevalence of FM was 17.8% (13 patients), with a significantly higher prevalence in women. Our analyses showed that FM is significantly associated with worse scores on CPDAI (4.98 points higher), DAPSA (14.71 points higher), and DAS28 (0.9 points higher).
Patients with PsA who had FM had a significantly lower likelihood of achieving MDA (RR of 0.57%). HAQ, BASDAI, and LEI scores were significantly worse in patients with PsA who had coexisting FM.
A treat-to-target strategy has been established for RA, and it is based on measuring disease activity and adjusting therapy accordingly. Adhering to this strategy has improved outcomes for patients with RA4. A treat-to-target approach has also been reported for SpA, including ankylosing spondylitis (AS) and PsA. The main target was defined as remission, with the alternative target of low disease activity5. The Tight Control of PsA (TICOPA) study has confirmed the benefit of using a treat-to-target approach in PsA. In that study, 206 patients with early PsA were randomized to either the tight control arm, with disease assessments every 4 weeks using MDA and escalation of therapies according to a protocol, or to standard care, with every-12th-week outpatient reviews for a 48-week study. Patients in the tight control arm showed a significant benefit in terms of peripheral joint disease activity, skin disease activity, and greater improvements in patient-reported outcomes, including quality of life and functional ability11,12.
FM frequently coexists with rheumatic diseases and has been found concurrently with RA, systemic lupus erythematosus, and Sjögren syndrome28. Ranzolin, et al29 demonstrated that the presence of FM in patients with RA is related to a higher DAS28. Azevedo, et al30 observed that patients with AS who had concomitant FM had higher scores on the BASDAI test compared to the scores of patients with AS who had no FM.
There are few published data on the prevalence and effect of FM in patients with PsA. Salaffi, et al20 found that the overall prevalence was 17.2% in patients with axial PsA, and much higher in women (34.2% vs 6.1% for men). Graceffa, et al21 found that a significant proportion (16%) of patients with PsA is also affected by FM, and that the presence of FM could predict a lower probability of achieving remission in patients with PsA. The data from our study revealed a similar FM prevalence in patients with PsA, and with a high predominance in women20,21,22,23,31.
Both PsA and FM share similar complaints among patients: extraarticular pain (which may originate from enthesitis, a common feature of PsA) and chronic back pain associated with morning stiffness (which may suggest axial involvement in patients with PsA). This overlap makes it very challenging to distinguish between PsA and FM18,20,31. Moreover, the evaluation for the presence of FM according to the 2010 ACR criteria is based on self-reporting of widespread pain and other symptoms such as fatigue. Fatigue and widespread pain are the 2 main symptoms of active PsA18,27. Thus, it is expected that subjects who fulfill the 2010 FM criteria would get worse scores on PsA activity indices.
In the case of enthesitis, patients with PsA who complain of widespread extraarticular pain may well have polyenthesitis, FM, or both. Marchesoni, et al32 suggested that power Doppler ultrasound assessment of the peripheral entheses can distinguish patients with PsA from patients with FM through the number and distribution of the involved sites, as well as the presence of inflammatory changes. However, this technique was not investigated for discriminating polyenthesitis and FM in the same patient with PsA.
Based on our results, we consider that when patients with PsA present with FM-type symptoms (e.g., increased extra-articular pain and fatigue) and high CPDAI or DAPSA scores, those symptoms should not be automatically attributed to increased PsA disease activity. In those cases, we recommend that FM should be ruled out before making any decisions on upgrading treatment or identifying patients as solely having refractory PsA. We also suggest that despite the increasing clinical use of the MDA measure11,12,33, MDA might not be suitable as a treatment target in patients with PsA and associated FM.
We are aware of some limitations in our study. The number of patients in the cohort is relatively small. In addition, FM symptoms may reflect depression and anxiety, which have not been evaluated in this cohort. However, the results we obtained showed differences that reached levels of significance, which probably indicates that the influence of FM on the investigated scores was real. Also, we did not inquire about the current therapy the patients were being given. By doing so, we may have had a better understanding of whether patients with PsA are treated excessively (such as with biological agents) because of the unidentified concomitant presence of FM.
Our data suggest that the coexistence of FM and PsA is related to worse scores on the CPDAI and DAPSA measurements, and that it could predict a lower probability to achieve MDA in patients with PsA. This should be taken into consideration in the treatment algorithm to avoid unnecessary upgrading of PsA treatment. We also recommend the performance of a study based on a larger number of patients to confirm our current findings.
Acknowledgment
Esther Eshkol is thanked for editorial assistance.
Footnotes
Work performed in partial fulfillment of Dr. Brikman’s MD thesis requirements of the Sackler Faculty of Medicine, Tel Aviv University.
- Accepted for publication April 20, 2016.








{kind=link}